9.5 Anti-Ulcer Medications V2
Learning Objectives
By the end of this section, the learner will:
- Identify the characteristics of antacid medications to treat hyperacidity conditions.
- Identity the characteristics of H2 receptor antagonist medications, including mechanism of action, onset and duration of action and nursing considerations.
- Identity the characteristics of proton pump inhibitor medications, including mechanism of action, onset and duration of action and nursing considerations.
- Articulate important client teaching experiencing hyperacidity for health promotion and medication safety.
- Apply clinical judgment for anti-ulcer medications including key assessments, administration, interventions and evaluation.
Hyperacidity Medication Classes
The goal of drug therapy is to alleviate symptoms, promote healing, prevent complications and prevent reoccurrence. Most medications do not alter the disease process, but create conditions to promote healing (Rosenjack Burcham & Rosenthal, 2019).
In this unit we will focus on the commonly used agents that are available over-the-counter or by prescription. The four main classes of anti-ulcer medications:
- Antacids,
- Antisecretory: H2 antagonists, Proton pump inhibitors (PPI’s),
- Mucosal protectants
Non-drug Therapy: along with taking medications to minimize symptoms or to promote healing, the client should be looking at lifestyle factors that may have contributed to their hyperacidity symptoms.
What role does diet, lifestyle, smoking and alcohol have? Refer back to the previous unit, 9.3 to check your answers.
Nursing Process and Clinical Judgment
Nursing Assessment (recognizing cues)
Self-report of symptoms (may include: epigastric pain, nausea, bitter taste in mouth, pain increases when supine, dysphagia, bloating, etc)
- What alleviates the discomfort?
- What exacerbates or triggers the symptoms?
- What remedies have you tried (OTC meds, home remedies, non-pharmacological)?
Objective cues:
- Abdominal assessment
- Vital signs
- Pain characteristics
- Nutritional history
This list is not exclusive; other assessments may be added depending on presenting symptoms.
Hypothesis
Based on reported symptoms,
Acute epigastric pain from GERD related to reflux symptoms as evidenced by:
- Burning pain in esophagus and stomach
- Pain increases when lying down
- Pain minimal when avoids certain foods such as caffeine and high-fat foods
Planning and Interventions
Three ways to promote healing/prevention of symptoms:
- Reduce gastric acidity – antisecretory agents (PPI, H2 antagonists), antacids, misoprostol
- Enhance mucosal protectants (sucralfate and misoprostol)
- Eradicate H. Pylori – antibiotics, antisecretory (PPI)
Depending on causative factors/symptom history, the treatment plan will include lifestyle changes (avoiding triggers and use non-pharmacological interventions) and start a trial of OTC anti-ulcer medications. This can be antacids, OTC PPI or H2RA.
Client teaching:
- Encourage diet modifications as prescribed
- General information about:
- Diagnosis and treatments
- Recognition of symptom progression
- Diet and lifestyle changes
- Support resources available
- Medications:
- Take medication as directed
- Report any medication side effects
- Call the provider if:
- Your pain or symptoms worsen
There are questions or concerns about the condition or increasing of symptoms.
Evaluation:
Symptom management – did the meds relieve the symptoms? What changes did the client make to their diet?
If no relief from symptoms, a prescriber may plan for testing such as a H. Pylori test or endoscopy to rule out other causes. They may write a prescription for a PPI or a H2 RA, and possible further testing to rule out other causative factors (ie. H. Pylori).
Some clients will be ordered a PPI for 6-8 weeks, then reassess symptoms. Refer to the PPI section for risk of long-term use of PPIs and the process of deprescribing PPIs (Bartels, 2024; Sealock, & Seneviratne, 2021).
Antacids
The use of antacids to control acid-related discomfort spans centuries. In ancient Greece, coral was crushed and given to those with dyspepsia: Coral is calcium carbonate.
There are many benefits to taking antacids, and these include that they are inexpensive, relatively safe and readily available. Due to their neutralizing abilities, they are widely used and available OTC for dyspepsia and acid indigestion.
Today, there are four main classes of antacids. These are:
- Aluminum based
- Magnesium based
- Calcium Based
- Sodium bicarbonate based
<p”>Antacids are alkaline compounds that neutralize stomach acid. They all differ in their acid neutralizing capacity (ANC), onset and duration of action, effect on the bowel (constipation vs. diarrhea) and other systems. The antacids most widely used have aluminum hydroxide and magnesium hydroxide in the formulation.
Refer to the Comparing Antacid Medications table for comparisons of the different antacids.
Drug Interactions:
Consider the strong possibility of drug interactions when taking antacids with other drugs. By raising gastric pH, antacids can influence the dissolution and absorption of many other drugs. Many drugs when combined with antacids have a decreased effect due to decreased absorption of that drug, from raising the gastric pH, chemically inactivating the drug or increasing the urinary pH leading to increased excretion. For example, some anti infectives such as tetracycline and ketoconazole will be less effective if taken at the same time as an antacid. Vitamin B12 malabsorption occurs when stomach acidity is altered, which in turn, can impact bone density.
Other drugs effected by antacids include thyroid hormones, or cardiovascular meds such as captopril or digoxin. Due to a long list of meds impacted by antacid use, nurses need to consider the best timing of a clients medications. What would be an important advice to a client? Or when you are administering meds to a client in the hospital?
Example in Practice:
A nurse is preparing the scheduled morning medications for a client. The client expressed they are experiencing heartburn and the nurse checks the orders and sees an antacid is ordered prn. Recognizing the potential for drug interactions, the nurse administers the scheduled meds at a separate time from the antacid.
Give any med 2 hours before or one hour after giving an antacid.
Antacid Medication Cards

Downloadable file (.docx): Calcium Carbonate – Antacid Medication Card

Downloadable file (.docx): Magnesium Hydroxide – Antacid Medication Card

Downloadable file (.docx): Aluminum Chloride – Antacid Medication Card

Downloadable file (.docx): Sodium Bicarbonate – Antacid Medication Card
Additional Antacid considerations
Combined formulas: Many antacids are formulated in combination with a second antacid. For example, Magnesium hydroxide and Aluminum hydroxide are combined to create a balanced formula. This combination is beneficial to improve the acid neutralizing action and can minimize some side effects. Magnesium is well known for its laxative effect, but combined with aluminum phosphate, which can cause constipation, the bowel effects are minimized.
Simethicone:
Many antacids also contain simethicone; an antiflatulent used for gas relief. This med decreases the surface tension of gas bubbles in the GI tract, dispersing the gas bubbles and then removed with belching or flatulence. It does not reduce the production of gas in the GI tract (Curtis & Akhondi, 2023).
Take as prescribed: Clients should be reminded to take OTC meds appropriately as prescribed and should not exceed the maximum dose. If symptoms persist or not effectively relieved, they should see their health care provider.

Andrea’s note: Jessica – Image from the current OER — ok to use?
Jessica – Nov 13, 2025: @Copyeditor could you please verify if the image above can be used?
Clinical Reasoning and Decision Making 1
Would you recommend this med?
A 72 year-old client attends a home health clinic for IV antibiotic therapy from a blood infection from an insect bite. She reports to the nurse she is concerned about an unrelated acid reflux issue. She reports 8/10 heartburn, mostly in the evening and sometimes it keeps her up at night.
History: hypertension, occasional constipation, osteoarthritis Rt knee, mild renal insufficiency. Otherwise, healthy. She is on two meds for hypertension and takes Ibuprofen as needed.
VS: HR 82 reg, BP 152/82, RR 16 breaths/min, T 37.6 C
The nurse recommends: Milk of Magnesium (magnesium hydroxide) 30 mLs po before bedtime.
a. Is this a good recommendation? Explain your answer.
b. What client teaching is important?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 9: Gastrointestinal Medications Answer Key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition sections at the end of the book.
Lifespan Considerations
Hyperacidity relief during pregnancy
Heartburn or hyperacidity is a common symptom experienced with pregnant clients. Heartburn is especially prevalent in this population: 22% of pregnant clients experience heartburn in the first trimester, going up the 60-72% in the third trimester (Garg, Narang & Taneja, 2022).
Causative factors for heartburn include the increased levels of female hormones including progesterone which can reduce lower esophageal sphincter pressure (Garg, Narang & Taneja, 2022). Antacids are first line treatment after lifestyle modifications are no longer effective. The only antacid not recommended is sodium bicarbonate, due to risk of fluid overload. If symptoms persist despite antacid use, then H2 RAs are an option following prescriber advice.
Anti-Secretory Medication: H2-Receptor Antagonist (H2RA)
H2RA’s are a well tolerated, effective option, if antacids are not effective. H2RA’s have been around for many years, and there are a number of meds under this classification. It is available OTC or by prescription, depending on the medication. The two we will review are cimetidine and famotidine. Ranitidine, previously a popular option, was taken off the market a few years ago due to impurities in the manufacturing process.
Uses:
H2RA Famotidine is used for a number of conditions including GERD, active duodenal ulcers, peptic ulcer disease and other hyperacidity conditions such as Zollinger-Ellison syndrome.
It is available OTC for the treatment of GERD, as well as it is given IV in the hospital setting for stress ulcer prophylaxis and upper GI bleeds.
Cimetidine is used for peptic ulcer disease, GERD and erosive esophagitis, but is used short term due to a number of side effects and drug interactions. It is also used for other conditions such as urticaria, mastocytosis, and erythropoietic protoporphyria (Pino & Azer, 2023).
A comparison of the two meds can be found below.
Diagram of a parietal cell and the action of a H2RA on the H2 receptors.
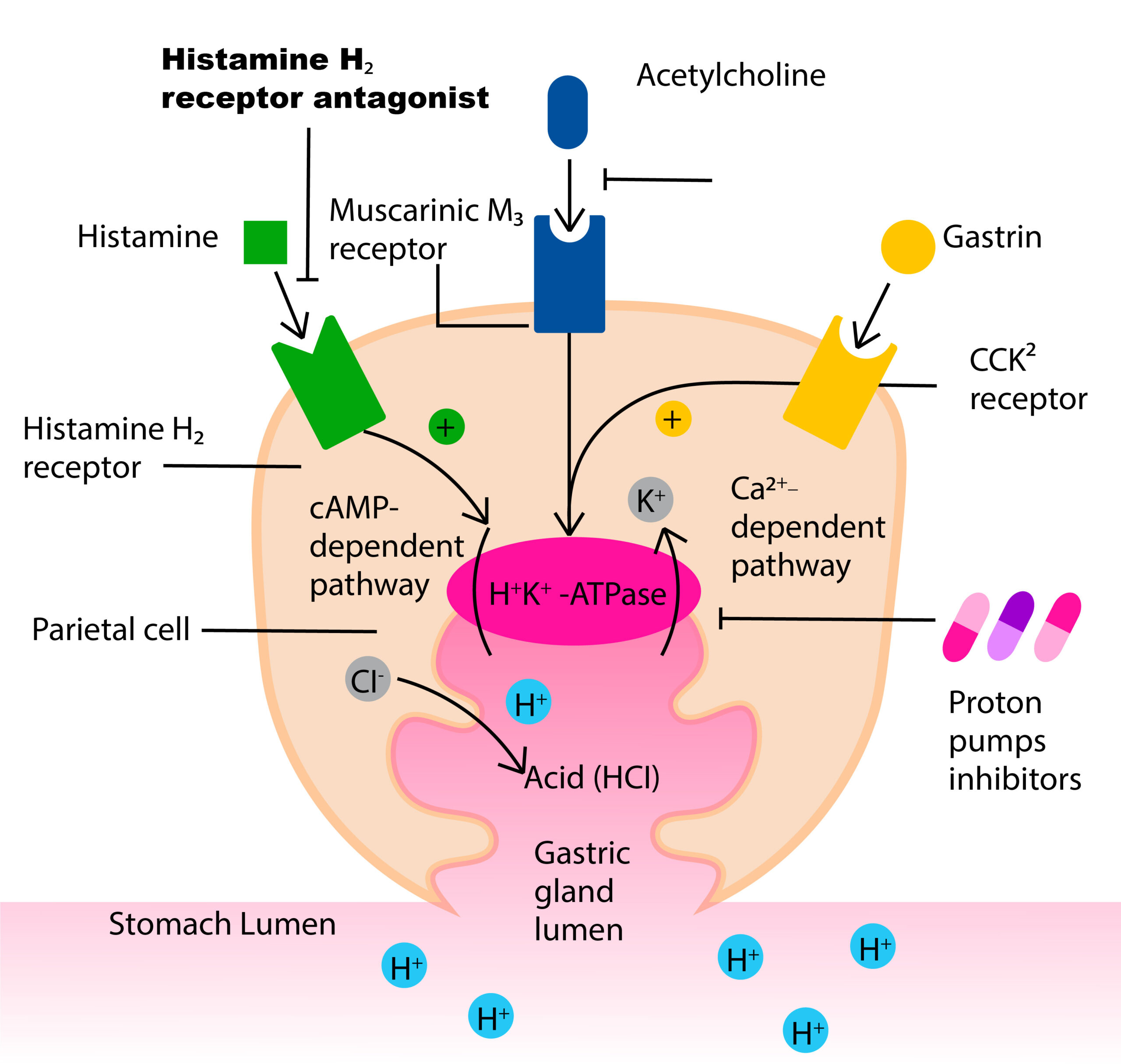
Parietal cells are located in the fundus and body regions of the stomach and are responsible for secreting hydrochloric acid via the hydrogen-potassium adenosine triphosphatase (H+/K+ ATPase) proton pump. Parietal cells secrete acid in response to three types of stimuli:
- Histamine, stimulates H2 histamine receptors
- Acetylcholine (Ach) (from parasympathetic activity from the vagus nerve and enteric nervous system) stimulates M3 receptors.
- Gastrin stimulates CCK2 receptors.
Activation of histamine through H2 receptor causes increases in the intracellular cAMP level, while ACh through M3 receptor and gastrin through CCK2 receptor increases intracellular calcium level. Through the combined actions, the proton pump moves hydrogen out of the parietal cell into the lumen in exchange for K+. Cl- moves into the lumen through Cl- channels. H+ and Cl- combine to produce HCL in the gastric lumen of the stomach (Wikipedia contributors, 2025, October 4).
H+ + Cl- → HCl
This results in an acidic gastric fluid with a pH 1-2.
Comparison of two H2RA medications:
Two common H2RA’s, Cimetidine and Famotidine, that are available OTC or by prescription. Both meds are effective at reducing HCL production. Famotidine is often a drug of choice due to being more potent, less drug interactions and other adverse effects.
| Cimetidine | Famotidine |
| Less potent |
More potent
Longer duration of action |
| Drug interactions Potent inhibitor of P 450 enzymes leading to drug interactions (increased concentration of warfarin, tricyclic antidepressants, lidocaine, calcium channel blockers, oral sulfonylureas, phenytoin, theophylline, benzodiazepines, and beta-blockers). |
No inhibition of P450 enzyme in liver, no drug interactions.
|
| Antiandrogenic effects · results in gynecomastia, impotence, and ↓ libido in males. All reversible once med is stopped. |
No anti-adrenergic effects
|
|
Crosses blood-brain barrier
· results in confusion, dizziness, and headaches |
|
| Slow absorption if taken with food |
Can take with food
|
| Avoid in the elderly (on Beers Criteria) due to more side effect risk and risk of cognitive impairment. |
Safe with the older adult and pediatric clients over 1 year of age
|
| Common side effects: GI: constipation, nausea and vomiting Musculoskeletal pain, myalgia/reversible myalgia Rash Fatigue, confusion Cimetidine→ ↓ creatinine clearance. Reversible once med is stopped. Monitor renal function. Decrease dosing due to prolonged effect |
Anxiety, headache,
Diarrhea, constipation Dizziness |
| Similarities of the two medications: | |
| Both meds safe during pregnancy | |
| Impairs B12 absorption; take B12 supplement.
Preexisting liver and kidney disease may require dosage adjustment. Famotidine is supported by evidence as safe for use in pediatric clients younger than 1 year old, as well as in geriatric clients (McCuistion, Vuljoin-DiMaggio, Winton, & Yeager, 2018) |
|
A common H2-receptor antagonist is famotidine (see Figure 9.5d).[6]
Our prototype will be Famotidine

Downloadable file (.docx): H2 Receptor Antagonist_Famotidine
Nursing Considerations:
- Monitor for abdominal pain, symptom relief
- Check renal panel and CBC before treatment.
- Obtain med profile, including OTC and herbal remedies.
Client Teaching:
- Oral suspension: shake vigorously 5-10 seconds prior to use
- Explain importance of lifestyle changes (smoking cessation, avoid NSAIDs, avoid trigger foods).
- Advise client to eat small, frequent meals than larger meals
- Increase fluid and fiber to decrease risk of constipation
- Avoid alcohol that can cause gastric irritation.
- If taking for a long time, B12 levels will decrease. Advise to increase B12 levels by including foods such as red meat, poultry, fish and eggs.
(Adams et al, 2018; McCuistion, Vuljoin-DiMaggio, Winton, & Yeager, 2018)
Proton Pump Inhibitors
Proton pump inhibitors (PPI) are the most effective anti-ulcer drugs available to suppress gastric acid secretion. They are used commonly for GERD, PUD and H. Pylori treatment, as well as other hypersecretory conditions. There are a few different PPIs available, both OTC and by prescription, but most are very similar in their effects. Prescribers may choose one over the other due to prescriber preferences, cost, dosing and client therapeutic response.
Proton pump options: pantoprazole, omeprazole, rabeprazole, lansoprazole. All PPI end in suffix ‘azole’
Our prototype will be pantoprazole
Indications for use
Pantoprazole is used in the treatment of GERD (regurgitation, heartburn) by blocking the production of hydrochloric acid and allowing time for the gastric mucosa to heal. It is also used for treatment of hypersecretory conditions, such as Zollinger-Ellison syndrome, and erosive esophagitis. It is also used for the treatment of H. Pylori infections, NSAID induced ulcers and preventing duodenal ulcers (Bernshteyn, Patel, Masood, 2025).
Andrea’s note: This pic is from the current OER
Mechanism of Action
PPIs bind irreversibly to the hydrogen-potassium ATPase enzyme system (proton pump) of the parietal cell, inhibiting the secretion of hydrochloric acid, the final step in gastric acid production. Due to the irreversible binding to the proton pump, it has a long duration of action up to 24 hours. Refer to the diagram located in the H2RA section.
Pantoprazole has a rapid onset of action, with the maximal effect occurring between 2 and 6 hours after administration. It can be given orally, both immediate release or delayed release options. It is also used intravenously with bleeding ulcers in the hospital setting. PPIs have a long duration of action due to the irreversible binding of the PPI to the proton pump. Although the half life is 2 hours, the irreversible binding to the proton pump means the body must create new proton pumps to resume acid production. The drug’s effect on stomach acid continues long after it has been cleared from the bloodstream (Bernshteyn, Patel, Masood, 2025).
Nursing Considerations
- Enteral administration: mix delayed-release granules with applesauce or apple juice and give by mouth or feeding tube.
- Drug interactions: can interfere with liver metabolism of other drugs. Check for drug compatibility.
- Monitor for symptoms of GI bleeding (black tarry stools, coffee ground emesis).
- IV administration can potentially exacerbate zinc deficiency.
- Check baseline liver function tests (ALT, AST) and renal function.
- Long term therapy can lead to vitamin deficiencies.
- If long term use, monitor bone density.
- Safe during pregnancy, but always consult health care provider prior to taking the PPI.
(Adams et al, 2018; McCuistion, Vuljoin-DiMaggio, Winton, & Yeager, 2018).
Adverse effects of Proton Pump Inhibitors
PPIs are a relatively safe medication if used correctly. Side effects can include diarrhea, headache, upper respiratory tract infection, and abdominal pain. These are often self-limiting.
Longterm complications:
Long term use of PPIs can lead to numerous adverse effects.
- Diarrhea that does not resolve, especially with hospitalized clients. The diarrhea can be attributed to Clostridium difficile.
- Small-intestinal bacterial overgrowth, due to reduction of hydrochloric acid allowing overgrowth of bacteria.
- Numerous vitamin deficiencies including vitamin B12, iron, calcium, magnesium. Hypomagnesemia can result in tetany, seizures or arrythmias.
- Bone demineralization, leading to higher risk of bone fractures. This risk is significant for the older adult and those with renal insufficiency.
- Drug interactions: diminished absorption of medications such as clopidogrel. Other drug interactions include warfarin and antiretrovirals.
- Interstitial nephritis – slight risk for acute kidney injury (AKI) and interstitial nephritis.
- Older adult: PPI in the older adult for longer than 8 weeks can lead to higher risk of Clostridium difficile infection and bone density loss which can lead to higher risk of bone fractures. As such, PPIs are on the Beers Criteria for inappropriate med with the older adult.
Client Teaching:
- Can take with or without food, but do not crush or chew. Preferable to take 30 minutes prior to meals.
- Avoid NSAIDs, alcohol or foods that cause gastric irritation.
- Advise clients to take PPIs as prescribed and do not take longer than 8 weeks unless advised by their health care provider.
- Report persistent diarrhea and abdominal pain.
Bernshteyn, Patel, Masood (2025); Sealock & Seneviratne (2021).
Treatment of H. Pylori
Following the diagnosis of H. Pylori, the recommended treatment includes two antibiotics and a PPI taken for 10 days. If the triple therapy is not effective, bismuth salicylate may be added to the regime. H. Pylori has become increasingly difficult to treat, so some changes to treatment include adding a third antibiotic and these are taken for 14 days (Canadian Digestive Health Foundation, 2025).
Mucosal Protectants
Sucralfate is a mucosal protectant to treat duodenal ulcers. It is also used off label for other medical conditions such as GERD, epithelial wounds, chemo-induced mucositis, and burn wounds. It forms a protective layer, enhancing bicarbonate production and has anti-peptic properties making it ideal for gastric ulcer healing. It further fosters tissue growth and regeneration. It is used for short term treatment to help heal ulcers, not prevent ulcer formation.
Mechanism of Action
Sucralfate covers the ulcer site in the GI tract and protects it against further attack by acid, pepsin, and bile salts. It works several ways once ingested:
- It forms a chemical reaction over the ulcerated site, forming a protective barrier. It binds to positively charged proteins in exudates, locally forming a thick viscous substance (Kudaravalli, Patel, & John, 2024).
- It stimulates the production of mucus and bicarbonate, which further fortify the stomach’s protective lining.
- It increases growth factors such as epidermal and fibroblast growth factors, promoting healing by facilitating tissue regeneration and repair.
It is minimally absorbed by the gastrointestinal tract. It is considered a relatively safe medication but some side effects and drug interactions occur.
Nursing Considerations
Onset of action is 1-2 hours, with a duration of 6 hours.
Considered safe with pregnancy, as not systemically absorbed.
Caution with clients with chronic renal failure: use cautiously with clients with chronic renal failure or those receiving dialysis due to impaired excretion of small amounts of absorbed aluminum that can occur with sucralfate.
Side effects:
- Constipation (primary side effect)
- Nausea, gas, indigestion
- Hyperglycemia with diabetic clients.
- Rash
- Dizziness, drowsiness
- Headache
Drug interactions:
- Sucralfate can decrease the serum concentrations of many medications, including digoxin, levothyroxine, furosemide, quinolones, oral phosphate supplements, warfarin. Ensure a 2-hour gap from administering these medications.
- Multivitamins can increase the serum concentration of sucralfate.
- Antacids can reduce efficacy by decreasing the binding ability of sucralfate to gastric ulcers. Do not take antacids within 15 minutes of taking sucralfate.
Client Teaching
- Take on an empty stomach, 2 hours after or 1 hour before meals.
- Take this med as prescribed, and for the full length of time, even if symptoms improve.
- If taking other meds, drug interactions may occur. Follow pharmacy guidelines when taking other meds.
- If pregnant or breastfeeding, ensure to check with your health care prescriber.
Anti-flatulent
Gas is a common issue that occurs in the GI tract due to digestive processes and the swallowing of air. Gaseous distension can also occur with post operative clients. For clients who have troublesome gas, simethicone is an antiflatulent that is commonly found in other OTC antacids (see Figure 9.5f). It is a relatively safe medication and can be used in infants and children.
Indications
Simethicone is used to treat the symptoms of gas such as uncomfortable or painful pressure, fullness, and bloating.
Mechanism of Action
Simethicone works by altering the elasticity of the mucous-coated gas bubbles, which cause them to break into smaller bubbles, thus reducing pain and facilitating expulsion.
Specific Administration Considerations
Simethicone is usually taken four times a day, after meals and at bedtime. For liquid form, shake drops before administering. It may cause minor side effects such as diarrhea, nausea, vomiting and headache.
Client Teaching
Clients can be instructed about other measures to assist with gas expulsion such as changing position, ambulation, avoiding the use of straws, and tapering intake of beans and cruciferous vegetables (Adam Medical, 2019; Lilley, Collins & Snyder, 2014; McCuistion, Vuljoin-DiMaggio, Winton & Yeager, 2018).
Comparing Medication Tables
To help with comparing the medications and to learn important considerations for each medication, refer to the medication tables Chapter 9 Comparing Antacids Medication table and Chapter 9 Comparing Anti-ulcer Medications Table
The medication cards are also intended to assist students to learn key points about each medication. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication. Basic information related to each class of medication is outlined below.
A client who recently underwent surgery has a medication order for daily pantoprazole. The nurse reviews the client’s medical history and finds no history of GERD or peptic ulcer disease. The client does not report any symptoms of heartburn, stomach pain, or sour stomach. The nurse reviews the physician’s orders for an indication for this medication before calling the provider to clarify.
What is the likely indication for this drug therapy for this client?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the “Answer Key” sections at the end of the book.
Interactive Activity
References
A.D.A.M. Medical Encyclopedia [Internet]. Atlanta (GA): A.D.A.M., Inc.; ©2019. Heartburn; [reviewed 2019 May 10; cited 2019 October 27]. https://medlineplus.gov/ency/anatomyvideos/000068.htm ↵
Adams, M., Urban, C., El-Hussein, M., Osuji, J. & King, S. (2018). Chapter 34: Pharmacotherapy of Peptic Ulcer Disease. In Pharmacology for Nurses. A pathophysiological approach (2nd Canadian ed.). Pearson Canada Inc: Ontario.
Bartel, E. (2024). Nursing guide to gastroesophageal reflux (GERD): nursing diagnosis, interventions and care plans. GERD: Nursing Diagnosis & Interventions | Nurse.com
Bernshteyn, M., Patel, P. & Masood, U. (2025, July 6). Pantoprazole. National Library of Medicine, StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK499945/
Canadian Digestive Health Foundation (2025). Peptic Ulcer and H. Pylori. www.cdhf.ca
DailyMed from US National Library of Medicine. www.dailymed.com
Drugs.com (2025). Sucralfate. https://www.drugs.com/mtm/sucralfate.html#before-taking
Garg, V., Narang, P. & Taneja, R. (2022). Antacids revisited: review on contemporary facts and relevance for self-management. Journal of International Medical Research, 50 (3), 1-22. DOI: 10.1177/03000605221086457
Ingold, C & Akhondi, H. (2023). Simethicone. National Library of Medicine, StatPearls [Internet]. Simethicone – StatPearls – NCBI Bookshelf
Lilley, L., Collins, S., & Snyder, J. (2014). Pharmacology and the Nursing Process. pp. 782-862. Elsevier. ↵ UPDATE
McCuistion, L., Vuljoin-DiMaggio, K., Winton, M, & Yeager, J. (2018). Pharmacology: A patient-centered nursing process approach. pp. 443-454. Elsevier. ↵
Pino, M. & Azer, S. (2023). Cimetidine. National Library of Medicine. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK544255/
Pujitha Kudaravalli, P., Patel, P., John, S. (2024, February 28). Sucralfate. National Library of Medicine. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK551527/
RNPedia. (2021). https://www.rnpedia.com
Sealock, K. & Seneviratne, C. (2021). Lilley’s Pharmacology for Canadian health care practice (4th Ed). Elsevier. ↵
Wikipedia contributors. (2025, October 4). Parietal cell. In Wikipedia, The Free Encyclopedia. Retrieved 21:14, October 25, 2025, from https://en.wikipedia.org/w/index.php?title=Parietal_cell&oldid=1315098778
This work is a derivative of Daily Med by U.S. National Library of Medicine in the public domain. ↵
“My Still LIfe” by Bast Productions is licensed under CC BY-NC-ND 2.0 ↵
Media Attributions
- Figure 9.5a Coral. Coral Image: https://commons.wikimedia.org/w/index.php?curid=36517926
- Figure 9.5b Example of Antacid tablets bottle “Antacid-L478.jpg” by Midnightcomm is licensed under CC BY-SA 3.0
- Figure 9.5c Parietal cell. Image made by TRU Open Press
- Figure 9.5d OTC Famotidine. A common H2-receptor antagonist is famotidine
- Figure 9.5e OTC Omeprazole”Prilosec Box 001” by cygnus921 is licensed under CC BY 2.0 ↵
- Figure 9.5f OTC Simethicone “Gelusil Antacid and Anti-Gas” by Wellspring Pharmaceutical is licensed under CC BY 2.0 ↵
hypersecretory condition of the hormone gastrin due to a tumour of the pancreas or duodenum. Gastrin is the hormonal signal for increasing hydrochloric acid, so when with an increase in acid it overcomes protective defences, leading to multiple gastric and duodenal ulcers. Treatment is aggressive use of acid suppression drugs (Adams et al, 2018).

{kind=link}