5.6 Antidepressants
Antidepressants are used to treat depression and other mood disorders, as well as other medical conditions such as migraine headaches, chronic pain, and premenstrual syndrome. Antidepressants modulate neurotransmitter activity, often increasing NT levels in the CNS. The primary NTs include serotonin (5-HT), dopamine, and norepinephrine. Treatment is based on the belief that alterations in the levels of these neurotransmitters are responsible for causing depression (Lilley et al, 2014).
This unit will discuss four classes of antidepressants: tricyclic antidepressants (TCAs), selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and monoamine oxidase inhibitors (MAOIs). These medications are compared in Table 5.6 at the end of this unit.
Other antidepressants not covered, but warrant a brief mention are:
Norepinephrine Dopamine Reuptake Inhibitor: bupropion
- Used for major depressive disorder, seasonal affective disorder, smoking cessation.
- Well tolerated with common side effects of headache, agitation, dry mouth and weight loss.
Serotonin-antagonist-and-reuptake-inhibitor: trazodone
- Used monotherapy or in combination with other psychotherapeutics to treat depression.
- Also blocks the histamine and α-1-adrenergic receptors although MOA not completely understood.
- Used for insomnia at low doses. Also used off label for Alzheimer’s, anxiety, bulimia, and fibromyalgia.
TCAs and MAOIs are referred to as first-generation antidepressants because they were first marketed in the 1950s. SSRIs, SNRIs, and other miscellaneous medications such as bupropion are called second-generation antidepressants and are popular because of fewer side effects like sedation, hypotension, anticholinergic effects, or cardiotoxicity (McCuistion et al, 2018).
For more information on different types of anti-depressants, watch this video.
Pharmacology – Antidepressants, SSRI, MAIO, TCA, SNRIs by Simple Nursing, is licensed under a Standard YouTube license
Principles of Pharmacotherapy
All antidepressants (AD) work to increase the availability of one or more of the neurotransmitters, serotonin, norepinephrine and dopamine. They work slightly different in targeting these neurotransmitters to alter mood and cognition. There are also many off label uses.
They all target certain symptoms with the aim of improving self-concept, sleep disturbances, appetite disturbance, fatigue, psychomotor retardation or agitation (Halter, Pollard & Jacubec, 2019). The overall goal of AD is complete remission of symptoms.
They all work equally well and all have side effects. Usually a client will trial a few different ADs before the most effective one is found. Considerations include tolerability, safety, drug interactions, history of past response and adverse effects, client preference and cost (Rosenjack Burchum & Rosenthal, 2019). Some side effects are beneficial. For example, for a client with fatigue, a drug that causes CNS stimulation would be chosen such as fluoxetine or bupropion. For a client with insomnia, a drug that causes sedation would be chosen, such as mirtazapine or trazadone.
To modulate the neurotransmitters effect on receptors, this takes time. They block or inhibit the NT within hours, but the therapeutic effects can take a few weeks. Symptoms resolve slowly, with initial responses in 1 to 3 weeks. Maximum responses can be 12 weeks. Clients are typically on an AD at least a month to see if any therapeutic benefit is observed. An adequate trial is 3 months and if an improvement in symptoms, then 4-8 weeks. Most clients are on the AD for 6 to 9 months after depressive symptoms improve. When antidepressants are discontinued, they are usually tapered over several weeks to avoid withdrawal (Halter, Pollard & Jacubec, 2019).
Treatment starts with a low dose to minimize side effects and then gradually increased. Depending on the client response, they are either switched to a different AD in the same class or another one is added from a different class. As mentioned, there are four main classes of antidepressants as well as atypical antidepressants. Each class has many types of medications. For example, tricyclic antidepressants have 9 different meds, although some are less used due to side effects or are used to target certain symptoms.
Two safety risks with most antidepressants are suicidal ideation and serotonin syndrome.
Suicide Risk
Safety warnings are in place for all classes of antidepressants used with children, adolescents, and young adults for a higher risk of suicide. All clients receiving antidepressants should be monitored for signs of worsening depression or changing behavior, especially when the medication is started or dosages are changed.
Antidepressants can increase the risk of suicide in the early stages of treatment before the full effects of the meds occur. Prior to starting on any AD, a person may feel very depressed, hopeless and even suicidal, and also have no energy or motivation. After starting on the med, the person’s depressive feelings start to improve and they get more energy, they may still feel very hopeless. They may consider suicide as a way out and now have more energy to carry through with their plan.
Close monitoring by health care providers, one week prescription of antidepressants at a time, and close monitoring and support by family and friends to ensure a safety plan is in place.
Serotonin Syndrome
Also known as serotonin toxicity, this potentially fatal condition arises from excessive serotonergic activity in the CNS, related to the therapeutic use of medications, drug interactions or from an intentional overdose. It is most common with SSRIs, SNRIs or MAOIs in combination of another serotonergic med, such as tramadol (analgesic), dextromethorphan (cough reliever), or illicit drugs (cocaine, MDMA).
Clients may experience mild to fatal symptoms, such as altered mental status (agitation, anxiety, confusion), autonomic dysfunction (sweating, fever, high blood pressure, tachycardia), neuromuscular excitation (tremor, rigidity, hyperreflexia, clonus) and /or gastrointestinal symptoms (nausea, vomiting, diarrhea).
In its most severe form, it can resemble neuroleptic malignant syndrome (NMS), which includes hyperthermia, muscle rigidity, autonomic instability with possible rapid fluctuation of vital signs, and mental status changes.
Symptoms can occur within one hour of ingestion of the excess medications, and depending on the dose, can begin with diarrhea, insomnia, tremor and shivering. Once recognized, treatment is often supportive and discontinuation of the implicated medications (Simon, Torrico, & Keenaghan, 2024).
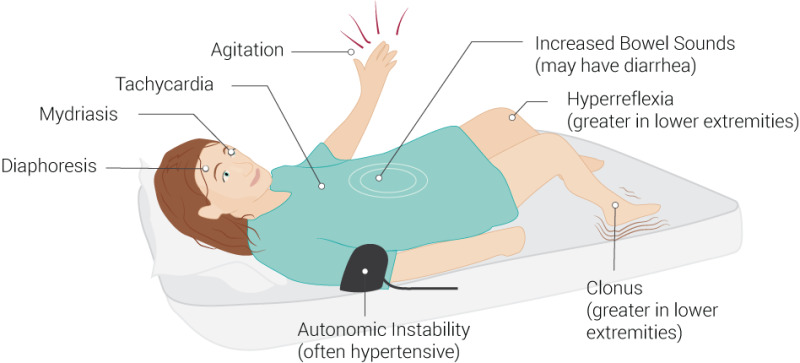
Image 5.6a: Symptoms of serotonin syndrome
Palmer, B. (2021). File:SerotoninSyndrome.jpg – Wikimedia Commons This file is licensed under the Creative Commons Attribution 4.0 International license.
Watch the video to learn more: Rhesus Medicine (2022). Serotonin Syndrome Explained. Serotonin Syndrome Explained (Serotonin Toxicity)
Tricyclic Antidepressants
Tricyclic antidepressants (TCAs) were one of the original first-generation antidepressants. Due to the safer profile of SSRIs and SNRIs, TCAs are now used second-line for treating depression but are used more commonly to treat neuropathic pain and insomnia.
Indications for Use
TCAs are used to treat major depressive disorder but only as a second line option. Although TCAs are very effective at treating depression, the safety concern of a higher risk of suicide and fatality with overdose, makes it a second-line treatment option.
There are many off-label uses including chronic neuropathic pain conditions (myofascial pain, diabetic neuropathy, postherpetic neuralgia), fibromyalgia, bipolar disorder, ADHD and insomnia. The TCA Imipramine is used as a second line treatment for nocturnal enuresis in children when the first-line therapy with desmopressin is ineffective (Moraczewski, Awosika & Aedma, 2023).
Mechanism of Action
Tricyclic antidepressants are so named due to the three rings in their chemical structure. They inhibit the reuptake of norepinephrine and serotonin at the presynaptic neuronal membrane resulting an increase of these NTs in the CNS synapses, intensifying their effects. Some TCAs such as amitriptyline, also has an affinity for muscarinic M1 receptors and histamine H1 receptors. TCA thus can cause sedation and anticholinergic side effects.
Watch the video for Mechanism of Action: Antidepressant Mechanism of Action: TCA
https://www.youtube.com/watch?v=AxsYh-ptasM
Pharmacokinetics
TCAs are rapidly absorbed and highly lipophilic thereby able to cross the blood brain barrier easily. Half-live is 24 hours, therefore once a day dosing. TCAs are lipophilic but each med in this class have different levels of lipophilicity. They all distribute widely throughout the tissues, including the CNS. They have moderate to high protein binding. Most have hepatic metabolism through P450 system. Renally excreted.
TCAs have a variable half life between 10-50 hours, depending on the drug. Dosages are always started at the lowest dose and titrated depending on the response (Moraczewski, Awosika & Aedma, 2023).
Nursing Considerations
Administration: oral form, readily absorbed. Peak levels obtained in 2-8 hours.
- If taken with food, absorption can be decreased and onset of action delayed.
- Usually administered at bedtime due to sedating effects. Night time dosing also reduces the intensity of side effects.
- Once a day dosing due to the long half-lives.
- Dosing is very individualized due to variable client response and risk of adverse effects.
Hepatic and renal insufficiency may warrant lower dosages and more frequent monitoring.
Tapering of Doses: After prolonged administration, abrupt cessation of treatment may produce nausea, headache, and malaise. The dose should be gradually tapered, but transient symptoms may still occur.
Lifespan considerations:
- TCAs should not be used in children for depression due to safety concerns.
- Pregnancy: There is a risk of congenital malformations (eye, ear, face defects). In addition, TCAs have been linked to preterm delivery, low birth weight, neonatal withdrawal syndrome, and persistent pulmonary hypertension in newborns. Overall, TCAs are not typically considered safe medication during pregnancy and should be avoided.
- Older Adult: Geriatric clients are particularly sensitive to the anticholinergic side effects of tricyclic antidepressants. Peripheral anticholinergic effects include tachycardia, urinary retention, constipation, dry mouth, blurred vision, and exacerbation of narrow-angle glaucoma. Central nervous system anticholinergic effects include cognitive impairment, psychomotor slowing, confusion, sedation, and delirium. Elderly clients taking amitriptyline may be at increased risk for falls. Elderly clients should be started on low doses of amitriptyline and observed closely.
Drug Interactions
TCAs can interact with many drugs. Ensure to complete a thorough medication profile. If both meds are needed, more frequent monitoring is required.
- Antidepressants: TCAs should be used cautiously with other antidepressants, if required, due to the risk of increasing serotonin levels, such as SSRIs, SNRIs and MAOIs. Serotonin Syndrome is a life-threatening condition if not recognized early (see box below).
- MAOIs: concurrent use can cause hypertensive crisis.
- Anticholinergic drugs: taking an anticholinergic drug such as antihistamines, can increase adverse effects of dry mouth, urinary retention, constipation, blurred vision and confusion.
- Anticoagulants: Concurrent use of warfarin or heparin, may increase the risk of bleeding. This might result from either the inhibition of platelet aggregation by certain TCAs or the displacement of warfarin from plasma proteins by specific TCAs.
- Anti-hypertensives: TCAs may cause additive or antagonistic effects with beta-blockers, calcium channel blockers, or clonidine. Monitor BP and HR closely.
(Sheffler; Patel & Abdijadid, 2023; Moraczewski, Awosika & Aedma, 2023).
Adverse/Side Effects
Side effects: most common are orthostatic hypotension, sedation and anticholinergic effects:
- Anticholinergic adverse effects such as constipation, urinary retention, photophobia, blurred vision, tachycardia, and drowsiness. This is due to TCAs blocking the muscarinic cholinergic receptors.
- Orthostatic hypotension: Blockage of alpha adrenergic and dopaminergic receptors can cause cardiac conduction disturbances and hypotension. Instruct clients to get up slowly, and lie down if symptoms of dizziness occur. For clients in the hospital, take BP and HR regularly, lying/sitting/standing positions to assess for low BP or high HR.
- Sedation: Histaminergic blockage can cause sedation.
- Seizure risk: serotonergic blockade can alter the seizure threshold for clients with seizure disorders.
- Higher risk of suicide: monitor closely the first 6 months for signs of worsening depression or changing behavior, especially when the medication is started or dosages are changed.
TCAs are contraindicated in the following conditions:
- Myocardial infarction
- Pregnancy, lactation
- Preexisting cardiovascular disorders, especially with preexisting bundle-branch block (may lead to heart block). TCAs decrease vagal influence on the heart and slow conduction in the bundle of His leading to higher risk of dysrhythmias. Monitor ECG before and periodically after the start of treatment for any clients at risk.
- Angle-closure glaucoma
- Prostate hypertrophy
- History of seizures.
- Hepatorenal diseases.
Overdosage
Death may occur from overdosage with this class of drugs. Multiple drug ingestion (including alcohol) is common in deliberate tricyclic antidepressant overdose. If an overdose occurs, consult with a Poison Information Center (1-800-567-8911).
TCA overdose – high risk of fatality.
TCA is unique among the ADs due to the lethal outcome in overdose situations. This is due to a number of reasons: TCAs are readily absorbed within a few hours and have a high volume of distribution in the body due to being highly lipophilic. TCAs have a narrow therapeutic index so overdosing on less than 10x the usual dose can be toxic. TCAs normally effect many receptors, not just SE and NE, but also histamine, alpha-adrenergic, and muscarinic receptors. In an overdose, the typical effects of blocking these receptors are amplified, but also sodium and potassium is also blocked in the cells leading to cardiac dysrhythmias from widening QRS, and eventual torsade’s de pointes. Sodium bicarbonate is an antidote to correct the metabolic acidosis and improve dysrhythmias, along with other supportive measures to manage the hypotension and seizures (Khalid & Waseem, 2023).
Watch the video to help remember key points of TCA Toxicity:
TCA Toxicity MADE EASY! TCA Toxicity MADE EASY! (with a FUN visual MNEMONIC) by AJmonics on Youtube.
Client Teaching:
- Due to the increased risk of suicidality with antidepressants, clients and their family members or caregivers should be instructed to immediately report any sudden changes in mood, behaviors, thoughts, or feelings. Mood elevation may take 7-28 days with 6-8 weeks for full effect (McCuistion et al, 2018; Lilley, Collins & Snyder, 2014).
- Inform of common side effects such as drowsiness, dizziness and hypotension and these will subside after a few weeks.
- Refrain from alcohol use as this may increase CNS depression and reduce the effectiveness of ADs.
- Take full dose at bedtime to minimize side effects. If dose is missed, take within 3 hours or wait until next scheduled dose. Do not double up dosages.
- Do not suddenly stop the med, as may experience nausea, nightmares, cold sweats within 2-4 days.
Halter, Pollard & Jacubec, 2019
Tricyclic Antidepressants Medication Card

Downloadable file (.docx): Tricyclic Antidepressants Medication Card
Selective Serotonin Reuptake Inhibitor (SSRI)
Selective Serotonin Reuptake Inhibitors (SSRIs) are second-generation antidepressants first introduced in 1987. They are the most prescribed antidepressant. Two common SSRIs are fluoxetine and citalopram. Fluoxetine will be our prototype med.
Indications for Use
SSRIs are primarily used to treat depression but are also used to treat obsessive-compulsive disorder, bulimia, panic disorder, posttraumatic stress disorder, other forms of anxiety, premenstrual syndrome, and migraines.
Mechanism of Action
SSRIs selectively block the reuptake of serotonin (5-HT) resulting in the increased concentration of serotonin in the synapse and increased activation of postsynaptic 5-HT receptors. The therapeutic effects are due to the adaptive cellular changes that occur with a prolonged reuptake blockage, not just the actual biochemical effect.
SSRIs have little effect on other neurotransmitters, such as dopamine, norepinephrine, acetylcholine or histamine, leading to fewer side effects.
Nursing Considerations
- Oral administration only, may take up to 6 weeks before the patients feel the effects of treatment.
- Caution if client has hepatic disease, anticipate dose reduction.
- Caution if taking other CNS medications; may cause additive sedative effects.
- Risk of serotonin syndrome with drug interactions or overdose. Monitor for symptoms.
- Monitor for increased risk of suicidal ideation, especially when therapy is initiated.
- SSRIs also have the potential to prolong the QT interval, which can lead to fatal arrhythmia, and torsade de pointes.
- Fatal overdose is rare compared to other antidepressants.
- Monitor weight before and during therapy.
Drug Interactions
Increased bleeding risk: concomitant use of fluoxetine and NSAIDs, aspirin, warfarin, or other drugs that affect coagulation. Monitor for signs of bleeding. Monitor INR more closely if client on warfarin, possible dosage reduction.
Adverse/Side Effects
SSRI’s are considered relatively safe and better tolerated than TCAs or MAOIs. Common side effects include nausea, agitation, insomnia, and sexual dysfunction (anorgasmia, impotence, delayed or absent ejaculation).
Other side effects include rash, mania, seizures, and weight gain.
High Alert Med:
- Higher risk of suicide, as with all classes of antidepressants used with children, adolescents, and young adults. Clients receiving antidepressants should be monitored for signs of worsening depression or changing behavior, especially when the medication is started or dosages are changed.
- Serotonin Syndrome: The development of a potentially life-threatening serotonin syndrome or neuroleptic malignant syndrome (NMS)-like reactions has been reported with SNRIs and SSRIs, particularly with concomitant use of serotonergic drugs, drugs that impair the metabolism of serotonin (including MAOIs), or with antipsychotics or other dopamine antagonists. See Serotonin Syndrome at the beginning of this unit for details of presenting symptoms.
Tapering of med for discontinuation: Abrupt discontinuation may discontinuation syndrome (dizziness, insomnia, nausea, agitation), so a gradual reduction in the dose rather than abrupt cessation is recommended whenever possible (Lilley et al, 2014; McCuistion et al, 2018).
Client Teaching
- Clients should be careful to take medications as directed. Abrupt discontinuation may cause anxiety, insomnia, and increased nervousness.
- Take the medication in the morning as they may cause insomnia if taken in the evening.
- Orthostatic blood pressure changes are possible during medication therapy. Advise client to change positions slowly.
- Anticipate increased drowsiness and dizziness at beginning of therapy.
- Avoid alcohol or other CNS depressant drugs.
- Clients, family, and caregivers should monitor clients carefully for suicidality.
- Inform client of side effects and monitor.
- Sexual dysfunction: sexual problems are underreported. Inform client of the probability and encourage reporting any issues. Depending on the severity, solutions can include a drug holiday for a few days or the addition of another medication such as bupropion or nefazadone.
- Weight gain is common, advise client to monitor weight.
- Some SSRIs should not be taken with grapefruit juice due to its effect on the CYP3A4 enzyme that affects the bioavailability of the medication. Consult with prescriber or pharmacist for drug specific guidance.
- Due to the risk of insomnia, recommend to the client to use a sleep diary to track their sleep. Also, to practice good sleep hygiene such as going to bed at a set time, avoiding stimulating activities/substances such as caffeine, nicotine or screen time and having a dark quiet room.
Example in Practice:
A 30-year-old client has been diagnosed with depression following a month of persistent depressive symptoms including hopelessness, anorexia, fatigue. She has started psychotherapy and the prescriber has started her on the SSRI: citalopram 20 mg po once a day in the morning. The nurse has provided some health teaching. The client understands this medication when she states that it may take a few weeks to start to feel a bit better, but knows it can take up to a few months. She knows to take the med in the morning, and not to double up if she misses a dose. She doesn’t like the idea about gaining weight but she will weigh herself every few weeks to see if she is affected. She knows not to stop taking the med if she doesn’t like the side effects and will see the prescriber first so she can be slowly taken off the med. She plans to keep her next appointment in a week and will let her mother know the plan, who is her primary support person.
Serotonin Selective Reuptake Inhibitors Medication Card
Medication cards like this are intended to assist students to learn key points about each medication. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication. Basic information related to each class of medication is outlined below.

Downloadable file (.docx): Serotonin Selective Reuptake Inhibitors Medication Card
Serotonin Norepinephrine Reuptake Inhibitor (SNRI)
The two most common SNRIs are venlafaxine and duloxetine. They are structurally different although both block the NE and SE receptors. Both are used for major depression, but venlafaxine is also approved for other conditions such as anxiety disorders.
Mechanism of Action
SNRI’s inhibit the reuptake of serotonin and norepinephrine, with weak inhibition of dopamine reuptake. It has minimal effects on other neurotransmitters, such as histamine or cholinergic receptors.
Indications for Use
Both SNRIs are indicated for the treatment of a major depressive disorder. Venlafaxine is also used for generalized anxiety disorder, social phobias and panic disorders. Duloxetine has also been approved for non-psychiatric conditions such as diabetic neuropathy and fibromyalgia.
Nursing Considerations
- Oral administration with immediate release and extended-release formulations. Take with food
- SNRIs are contraindicated with MAOIs or within 14 days of use of an MAOI.
- Dosage adjustment is required for use in clients with renal and/or liver disease. Do to hepatotoxicity risk, do not give to clients with liver disease or those who consume large amounts of alcohol.
- Elderly clients are at greater risk for developing hyponatremia.
- Use with caution with other serotonin medications to avoid serotonin syndrome.
- Do not abruptly discontinue med, as can lead to withdrawal syndrome. Symptoms include anxiety, agitation, tremors, headache, vertigo, nausea, tachycardia and tinnitus. Taper dose when discontinuing.
- Pregnancy: late pregnancy use of Venlafaxine may result in neonatal abstinence syndrome characterized by irritability, abnormal crying, tremor, respiratory distress and seizures.
(Halter, Pollard & Jacubec, 2019; Rosenjack Burchum & Rosenthal, 2019)
Adverse/Side Effects
Common side effects include nausea, dry mouth, insomnia, constipation, reduced appetite, fatigue, increased sweating.
May cause increase in blood pressure. Monitor BP before treatment starts and periodically throughout treatment.
High Alert Med: As with all classes of antidepressants, there is a high risk of suicide if used with children, adolescents, and young adults.
Monitor for signs of worsening depression or changing behavior, especially when the medication is started or dosages are changed. Dose is started low, and tapered up depending on the effect.
Drug Interactions: increased risk of serotonergic and anticoagulant effects, especially with the concomitant use of fluoxetine and NSAIDs, aspirin, warfarin, or other drugs that affect coagulation. Monitor for bleeding. If client on warfarin, increase frequency of INR monitoring, and possible dose reduction.
Client Teaching
- Clients should be careful to take medications as directed.
- If discontinuing the med, must be tapered prior to discontinuation.
- Inform client of possible side effects, such as increased drowsiness or dizziness.
- Use of SNRI medications with alcohol or other CNS depressant drugs should be avoided.
- Suicide risk: at the start of therapy and throughout, family and caregivers should monitor clients carefully for suicidality.
(McCuistion et al, 2018: Lilley et al, 2014)
Serotonin Norepinephrine Reuptake Inhibitor: Venlafaxine Medication Card
Medication cards like this are intended to assist students to learn key points about each medication. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication. Basic information related to each class of medication is outlined below.

Downloadable file (.docx): Serotonin Norepinephrine Reuptake Inhibitor – Venlafaxine Medication Card
Monoamine Oxidase inhibitors (MAOI)
Monoamine oxidase inhibitors (MAOIs) have been used since the 1950s and are a first-generation antidepressant. They were used successfully to treat severe melancholic depression but fell out of favour due to adverse effects and the discovery of new antidepressants. A significant disadvantage to MAOIs is their potential to cause a hypertensive crisis when taken with stimulant medications or foods containing tyramine. Today, nonselective MAOIs have fallen out of use due to the dietary and drug restrictions, but can be for atypical depression as a second or third choice after other antidepressants have been tried.
Mechanism of Action
The mechanism of action of MAOIs is not fully understood but is presumed to be linked to the potentiation of monoamine neurotransmitter activity in the central nervous system resulting from its inhibition of the enzyme monoamine oxidase (MAO). MAOIs prevent the breakdown of monoamine neurotransmitters, NE, dopamine, and serotonin, resulting in increased concentrations of these NTs in the brain and subsequent improved mood. But they also prevent the breakdown of tyramine, resulting in tyramine being absorbed and taken up by adrenergic neurons which causes a massive release of NE leading to hypertension (McCuistion et al, 2018).
MAOIs (tranylcypromine) have originally been non-selective and irreversible, meaning they prevent the breakdown of both MAO-A and MAO-B. Irreversible binding to the receptor means that the effect will last until the enzyme is eventually replaced. This formulation causes the most adverse effects of hypertensive crisis. New formulations have created reversible and selective MAOIs (moclobemide) or selective to MAO-B (selegiline).
Monoamine Oxidase Enzyme
Is a mitochondrial enzyme that is found in most tissues. MAO enzymes degrade monoamines which are located in the liver and in nerve endings that release the neurotransmitters NE, 5-HT and dopamine. They exist in two forms: MAO-A responsible for the catabolism of NE and 5-HT in the brain. In the intestine, MAO-A metabolizes tyramine of ingested food. MAO-B which is selective for dopamine metabolism.
Indications for Use
MAOIs are indicated for the treatment of major depressive disorder or atypical depression in adult clients who have not responded adequately to other antidepressants. Depending on the med, they are also used off label to treat Parkinson’s disease, mood disorders such as anxiety or obsessive-compulsive disorder.
Selegiline at low doses – MAOI-B selective: treats Parkinsons Disease
Selegiline at high doses – MAOI-A and B non-selective: treats depression
Phenelzine – MAOI A and B non-selective: treats depression
To learn more about MAO inhibitors, watch the following YouTube video by Osmosis: Video: Monoamine oxidase inhibitors | Osmosis
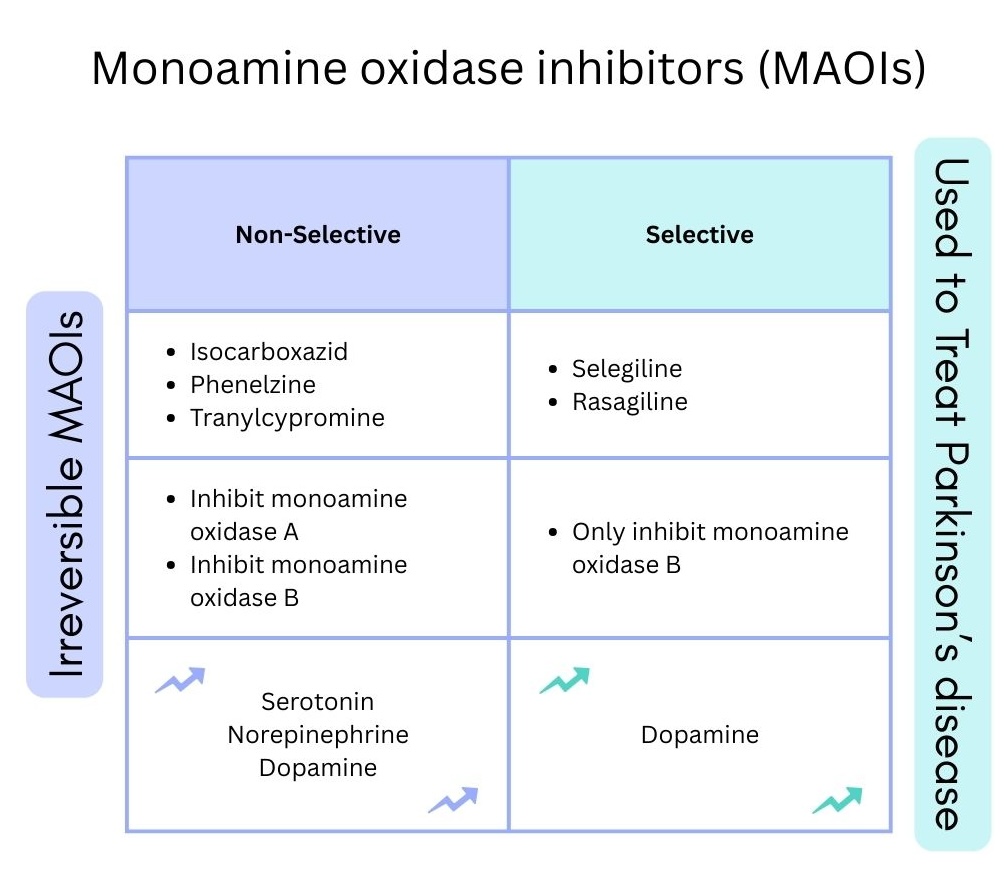
Comparison between non-selective and selective MAOIs. Non-selective MAOIs, irreversibly inhibit MAOI-A and MAOI-B, leading to an increase in serotonin, norepinephrine and dopamine. Selective MAOI’s, that only inhibit MAOI-B, and only increase dopamine, making it a good option for the treatment of Parkinson’s disease.
Nursing Considerations
Administration: oral or transdermal patch (Selegiline)
- Selegiline transdermal patch: apply q 24 hours to upper arm, upper torso or upper thigh. Common reaction is a localized rash, may apply a topical glucocorticoid as needed.
- may take up to 4 weeks to see effect. Energy may increase before mood, therefore caution with suicidal risk.
- Wash out period of 2 weeks is required if the antidepressant is changed to another med.
Risk of Hypertensive Crisis with foods containing tyramine. Many foods contain the monoamine tyramine (see list below) so these foods should be avoided for non-selective MAOIs.
Lifespan considerations:
- Safety has not been established with the pediatric population.
- The elderly population is at increased risk for postural hypotension and serious adverse effects.
Misuse and dependence have been reported.
Should not be used for clients with hepatic or renal disease.
Drug Interactions
There are many drug interactions so a thorough medication profile and health teaching is important.
- Antidepressants: most antidepressants inhibit the reuptake serotonin, so if taken with MAOI, there is a risk of serotonin syndrome. If a switch to a different AD is required, a washout period of 2 weeks is required.
- Sympathomimetics: Cold remedies containing amphetamines (phenylephrine, ephedrine) or other adrenergic meds can lead to a hypertensive crisis as they add to the pro-noradrenergic actions of MAO inhibition. Inform clients that taking any OTC meds for decongestants or cough suppression should be discussed with the physician or pharmacist.
- Antibiotic Linezolid: Patients taking MAOIs or other serotonergic psychiatric medications should avoid taking the antibacterial drug linezolid. This antibiotic has MAOI activity as it selectively prevents bacterial protein synthesis through the inhibition of monoamine oxidase. There may be increased risk of serotonin syndrome.
- Other drugs that should be avoided are H2 Receptor Antagonist Cimetidine and synthetic opioids such as tramadol or methadone.
(Edinoff et al, 2022)
Tyramine rich foods
Many foods contain tyramine and usually this monoamine is metabolized by the liver and gut and therefore never reaches a high concentration. But, if the client is on a non-selective MAOI, tyramine is not metabolized, leading to high levels and high blood pressure.
Many foods contain tyramine and include old cheese, yeast products, pickled foods, red beans, red wine, yogurt, and smoked meats.
Although a very effective antidepressant, MAOI meds have been mostly replaced with other antidepressants due to the strict diet that would be required while on this med.

Figure 5.6e Tyramine rich foods include smoked meats, old cheese and pickled foods.
Image by BobPetUK https://www.flickr.com/photos/22179048@N05/5947451320
Adverse/Side Effects
Early in treatment, side effects are common and include orthostatic hypotension, daytime fatigue, insomnia, nausea, constipation and dry mouth.
Long term effects include weight gain and sexual dysfunction.
High Alert Med: The risk of suicide are in place for all classes of antidepressants used with children, adolescents, and young adults. Clients receiving antidepressants should be monitored for signs of worsening depression or changing behavior, especially when the medication is started or dosages are changed.
Risk of hypertensive crisis: This is defined by severe hypertension (blood pressure greater than 180/120 mm Hg) with evidence of organ dysfunction. Symptoms may include occipital headache (which may radiate frontally), palpitations, neck stiffness or soreness, nausea or vomiting, sweating, dilated pupils, photophobia, shortness of breath, or confusion. Either tachycardia or bradycardia may be present and may be associated with constricting chest pain.
Risk of serotonin syndrome: Risk if higher doses or concurrent use of other serotonergic medications. Monitor for symptoms including neuromuscular, autonomic, gastrointestinal or altered mental status.
Client Teaching
- Clients should be careful to take medications as directed. It may take up to 4 weeks to see the effects of the drug. They should avoid abrupt cessation of therapy to avoid withdrawal symptoms.
- Inform client of diet restrictions if taking a non-selective MAOI. Dietician consult may be required.
- Inform client to not take any OTC medications (cough and cold remedies) unless first consulting the prescriber or pharmacist.
- Clients should avoid alcohol, other CNS depressants, and tyramine-containing products for two weeks after therapy is discontinued.
- Clients should be advised regarding the signs of hypertensive crisis and to immediately report headache, chest or throat tightness, and palpitations to the provider.
Monoamine Oxidase Inhibitors Medication Card
Now let’s take a closer look at a medication grid that compares these classifications of anti-depressants (Lilley et al, 2014; McCuistion et al, 2018).
Medication cards like this are intended to assist students to learn key points about each medication. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication. Basic information related to each class of medication is outlined below.

Downloadable file (.docx): Monoamine Oxidase Inhibitors Medication Card
Herbal Preparation: St. John’s Wort Benefits and Dangers
St. John’s Wort is a plant with yellow flowers that has been used for a long time for traditional medicinal purposes. It is currently available OTC as a herbal supplement. It can be taken for mild depression and other ailments. But it comes with a warning, as it interacts with many drugs. Clients on serotonergic antidepressants should not take St John’s Wort as it can increase serotonin levels leading to serotonin syndrome. It also interacts with oral contraceptives, warfarin, statins and digoxin. For nurses, ensuring to ask about herbal supplements or any OTC medications will help ensure client safety with any med.

File:Common St. John’s-Wort (Hypericum perforatum) – London, Ontario.jpg – Wikimedia Commons CC BY-SA 4.0
To support your learning, you can access the Chapter 5 Comparing Antidepressant Medications Table. This is a downloadable and editable document to allow you to update and add content.
Clinical Reasoning and Decision-Making Activity 5.6
1.A 32-year-old female visits the nurse practitioner with concerns about “feeling tired all the time,” “having difficulty concentrating,” “problems sleeping,” and “just generally feeling down.” The nurse practitioner prescribed fluoxetine.
The client tells the nurse, “One of my friends told me I have to be careful or I might get serotonin syndrome if I take medication.”
a. What places a client at risk for serotonin syndrome, and what symptoms should the nurse teach the client about this condition?
b. The nurse knows that anyone starting an antidepressant is at risk for suicidal thoughts. How should the nurse therapeutically discuss this potential adverse effect with the client?
c. What potential common side effects should the nurse discuss with the client?
The client states, “I can’t wait to feel better again. How soon will this medication work?”
d. What is the nurse’s best response?
2. You are working with a client who is being treated for treatment resistant depression. Their mood has been very low with anhedonia, decreased ability to function, fatigue and hopelessness. They wish that they will go to sleep and not wake up. They do not have any active plans to harm themselves. They do not have any symptoms of psychosis. They report watching TV throughout the day and have difficulties sleeping at night. They average 5 hours of interrupted sleep at night and a 45 min nap in the day time.
They have been prescribed venlafaxine ER 300 mg OD and have been taking the medication at bedtime.
What education can you provide for the client?
3.On your next appointment the client tells you that their family physician has prescribed aripiprazole. They noticed on the handouts from the pharmacist that it is an antipsychotic medication and are concerned because they do not have symptoms of psychosis.
What information can you provide the client.
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the “Answer Key” sections at the end of the book.
Interactive Activities
References
- Edinoff, A.N, Swinford, CR, Odisho, A.S, Burroughs, C.R, Stark, C.W, Raslan, W.A, Cornett, E.M, Kaye, AM, Kaye ,A.D. (2022). Clinically Relevant Drug Interactions with Monoamine Oxidase Inhibitors. Health Psychology Research, 10(4):39576. doi: 10.52965/001c.39576. PMID: 36425231; PMCID: PMC9680847.
- Halter, M., Pollard, C. & Jacubec, S. (2019). Varcarolis’s Canadian Psychiatric Mental Health Nursing. A clinical approach (2nded.). Elsevier: Canada.
- Hodnet, R. (2015). Common St. John’s-Wort (Hypericum perforatum) – London, Ontario.jpg File:Common St. John’s-Wort (Hypericum perforatum) – London, Ontario.jpg – Wikimedia Commons
- Jordan Moraczewski; J., Awosika, A.O., & Aedma, K. (2023). Tricyclic Antidepressants. National Library of Medicine. StatPearls [internet]. Tricyclic Antidepressants – StatPearls – NCBI Bookshelf
- Lilley, L., Collins, S., & Snyder, J. (2014). Pharmacology and the Nursing Process. pp. 246-272. Elsevier. ↵
- McCuistion, L., Vuljoin-DiMaggio, K., Winton, M, & Yeager, J. (2018). Pharmacology: A patient-centered nursing process approach. pp. 227-305. Elsevier. ↵
- Muhammad M. Khalid; M. & Waseem, M. (2023). Tricyclic Antidepressant Toxicity. National Library of Medicine. Tricyclic Antidepressant Toxicity – StatPearls – NCBI Bookshelf
- Rosenjack Burchum, J., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
- RNpedia. (2022). Antidepressants. https://www.rnpedia.com/nursing-notes/pharmacology-drug-study-notes/antidepressants/ ↵
- RNpedia. (2021). https://www.rnpedia.com
- Simon, L., Torrico, T., & Keenaghan, M. (2024). Serotonin Syndrome. National Library of Medicine. Serotonin Syndrome – StatPearls – NCBI Bookshelf
Media
-
- Pharmacology – Antidepressants, SSRI, MAIO, TCA, SNRIs by Simple Nursing, is licensed under a Standard YouTube license
- Watch the video to learn more: Rhesus Medicine (2022). Serotonin Syndrome Explained. Serotonin Syndrome Explained (Serotonin Toxicity)
- Image 5.6a: Symptoms of serotonin syndrome
- Palmer, B. (2021). File:SerotoninSyndrome.jpg – Wikimedia Commons This file is licensed under the Creative Commons Attribution 4.0 International license.
- Watch the video for Mechanism of Action: Antidepressant Mechanism of Action: TCA
- https://www.youtube.com/watch?v=AxsYh-ptasM
- 5.6b: comparison between selective and non-selective MAOIs (TRU Open Press)
- BobPetUK at https://www.flickr.com/photos/22179048@N05/5947451320
- File:Common St. John’s-Wort (Hypericum perforatum) – London, Ontario.jpg – Wikimedia Commons CC BY-SA 4.0

{kind=link}
_-_London,_Ontario.jpg){kind=link}