7.5 Antiarrhythmics V2
Antiarrhythmics
An arrhythmia is any deviation from the normal rate or pattern of a heartbeat. This includes heart rates that are too slow (bradycardia), too fast (tachycardia), or irregular. The terms dysrhythmia (disturbed heart rhythm) and arrhythmia (without rhythm) are traditionally used interchangeably in clinical practice despite their difference in meaning.
The ECG is used to identify and monitor an arrhythmia. See more information about ECGs in the “Review of Basic Concepts” section and an overview of arrhythmias in the “Common Cardiac Disorders” section.
Antiarrhythmic medications regulate heart rate and rhythm by manipulating the conduction of electrical signals to change the heart rate or to attempt to revert an arrhythmia to a normal sinus rhythm. Treating the arrhythmia depends on the symptoms the client is experiencing and the potential severity. The treatment is directed at the cause and antiarrhythmic medications is one treatment option. Depending on the rhythm and severity, other treatments include cardioversion, pacemakers, catheter ablation and implantable defibrillators.
All antiarrhythmic medications have a risk of producing an arrhythmia so careful monitoring is required. This can include continuous or intermittent ECG analysis, blood pressure, heart rate, and other physical changes such as chest pain, respiratory status (SOB, dyspnea, lung sounds, hypoxia), neurological changes (LOC, syncope, confusion) and fluid status. Some antiarrhythmic medications are used during emergency situations such as cardiac arrest, whereas others are used long-term, such as those that control atrial fibrillation.
Most antiarrhythmic drugs are grouped into 4 main classes (Vaughan Williams classification) based on their dominant cellular electrophysiologic effect or mechanism of action (Merck Manual, 2023). Some drugs have more than one mechanism of action and fit into more than one category.
Vaughan Williams Classification of Antiarrhythmic Drugs
Drs. Singh and Vaughan Williams developed the classification system in 1970. It classifies antiarrhythmic drugs based on their dominant cellular electrophysiologic effect. The four classes of drugs also have subclasses (1A, 1B etc). Due to the evolving understanding of physiology and the development of new drugs, this drug classification system has some limitations. Some drugs are not included, and many drugs could fit into more than one class due to having more than one mechanism of action. For example, amiodarone, a class III drug, also has sodium and calcium-channel blocking actions. Some revisions have occurred to reflect current research. Despite its limitations, it is the classification system that is still predominately used.
Vaughan Williams Classification of Antiarrhythmic Drugs
| Class | Action/ Drug | Mechanism of Action |
| I | Sodium channel Blockers
Ia: Quinidine, Procainamide Ib: Lidocaine, Phenytoin Ic: Propafenone, Flecainide |
Sodium channel blockers (membrane-stabilizing drugs).
Block fast sodium channels and slow conduction in fast-channel tissues (working atrial and ventricular myocytes, His-Purkinje system). Class I drugs are subdivided into subclasses Ia, Ib, and Ic. |
| II | Beta Blockers
Acebutolol Propranolol Sotalol |
Affect sinoatrial [SA] and atrioventricular [AV] nodes.
Action: decrease rate of automaticity, slow conduction velocity, and prolong refractoriness.
|
| III | Potassium channel blockers
Amiodarone, Sotalol |
Prolong action potential duration and refractoriness in slow- and fast-channel tissues.
|
| IV | Calcium channel blockers
Verapamil, Diltiazem |
Non-dihydropyridine calcium channel blockers.
Action: depress calcium-dependent action potentials in slow-channel tissues resulting in a decrease the rate of automaticity, slow conduction velocity, & prolong refractoriness.
|
| V | Adenosine | Diagnose and terminate SVT |
Class I – Sodium Channel Blockers
Class I antidysrhythmic medications slow conduction and prolong depolarization by decreasing sodium influx into cardiac cells. There are three subgroups of sodium channel blockers: Class IA, IB, and IC. Procainamide is an example of a Class IA antidysrhythmic. Lidocaine is an example of a Class IB medication that is also used as a local anesthetic. Flecainide is an example of a class IC antidysrhythmic.
Mechanism of Action
Sodium channel blockers block fast sodium channels, by slowing the conduction and prolongs depolarization by decreasing sodium influx into cardiac cells. The conduction rate and automaticity are decreased. They work on atrial and ventricular myocytes and His-Purkinje system. On an ECG, you will see a widening of the P wave or QRS complex, prolonged PR interval or a combination (Merck Manual, 2023). The different subclasses of class I drugs, relates to the kinetics of the sodium channel effects based on the heart rate.
Class IA drugs have intermediate kinetics, so their fast-channel tissue conduction slowing effects may or may not have an effect on normal rhythm at a normal rate. Class IA drugs block repolarizing potassium channels, prolonging the refractory periods of fast-channel tissues. On the ECG, the QT-interval will be prolonged even at normal rates. This class of drugs are used for fast rhythms such as supraventricular tachyarrhythmias (atrial fibrillation, atrial flutter, atrial tachycardia) and ventricular tachyarrhythmias (ventricular tachycardia and ventricular fibrillation)
Class IB drugs have fast kinetics, so their effects are only on fast heart rates. They have minimal effects on atrial tissue. They are used to suppress ventricular tachyarrhythmias such as ventricular tachycardia or ventricular fibrillation.
Class IC drugs have slow kinetics, and their effects are evident with all heart rates. They are more potent than class IB antiarrhythmics. They are used for both atrial and ventricular tachydysrhythmias (atrial fibrillation, atrial flutter, ventricular tachydysrhythmias).
This can help explain why physicians may choose one drug class over another when treating a dysrhythmia.
Indications for Use: Procainamide
Depending on the subclass, the use will be different as outlined above. We will examine class 1a drug Procainamide in this unit.
Procainamide is used for chemical cardioversion in treating atrial flutter and atrial fibrillation, in terminating ventricular tachycardia, supraventricular arrhythmias, and in restoring sinus rhythm in Wolf-Parkinson-White syndrome (Patel & Goyal, 2024).
Nursing Considerations
Administration:
- Procainamide is given IV or PO with the onset of action in 10 to 30 minutes.
- IV: can be given IV direct or infusion. A loading dose of IV procainamide is 10 to 17 mg/kg and administered at a rate of 20 to 50 mg/min (100 mg q 5 minutes). A maintenance dose would follow.
- Oral: for supraventricular arrhythmia, based on weight and given in divided doses every 6 hours. For example: 50 mg/kg/24 hours divided into doses every 6 hours. Do not crush extended-release tablets.
Metabolized by the liver and renally excreted. Half-life is 3 hours.
Monitoring:
- Continuous ECG monitoring. Assess for heart block, PVCs, greater than 50% QRS widening.
- Monitor blood pressure. If greater than 15 mmHg drop, notify MD.
- During IV administration: client on bedrest to avoid hypotension.
- Monitor CBC, platelets, electrolytes
- Monitor urine output
(Vallerand & Sanoski, 2024)
Sodium channel blockers are contraindicated in clients who have a history of thrombocytopenia, myasthenia gravis or electrolyte imbalances (particularly hypokalemia and hypomagnesemia)
Use cautiously with clients who have a serious heart block rhythm and do not have an artificial pacemaker, such as a 2nd degree heart block.
There is an increased risk for toxicity with clients who have heart failure and renal or hepatic dysfunction due to drug accumulation. Dose reduction for renal impairment and up to 50% dose reduction with liver disease.
Children: can be given but safety not fully evaluated.
Pregnancy: crosses the placental barrier
Grapefruit juice should be avoided by clients taking this medication.
Drug Interactions:
These drugs interact with many drugs, including cardiac glycosides, cimetidine, anticonvulsants, nifedipine, and warfarin. A complete med profile is needed before initiating therapy.
Adverse/Side Effects
Side effects:
- Hypotension
- Nausea, vomiting, diarrhea
- Fever
- Premature ventricular contractions (PVCs)
Adverse Effects:
Adverse effects include cardiac toxicity, bradycardia, drug-induced lupus erythematosus-like syndrome, and blood dyscrasias.
- Cardiac side effects: QRS, QTc, and PR prolongation which can worsen when levels of procainamide rise. Can lead to torsade’s de pointes. ECG monitoring is important during treatment. Procainamide infusion may also increase the number of PVCs.
- Drug-induced lupus erythematosus-like syndrome (rare): can occur with chronic use.
- Blood dyscrasias (rare): bone marrow depression, leading to pancytopenia or agranulocytosis, thrombocytopenia.
(Pritchard & Thompson, 2023)
Client Teaching
- Instruct client to take med exactly as prescribed
- Take with food to minimize GI upset
- Monitor pulse and blood pressure as recommended
- Report any fever, joint pain or rash to their health care provider
- Report immediately any shortness of breath, signs of bleeding, bruising, persistent headache.
- May experience dizziness so take precautions to avoid falls.
- Inform prescriber if you are pregnant or plan to become pregnant
- Caution with using CNS depressants such as alcohol, may contribute to dizziness. Avoid caffeine and tobacco.
(Medline Plus, 2026)
Class II – Beta Adrenoreceptor Antagonists (Beta Blockers)
Beta blockers are used widely for cardiovascular disorders. They are first-line antiarrhythmic therapy because of their excellent safety profile and effectiveness in treating ventricular arrhythmias. In the heart, they are used to decrease conduction velocity, automaticity, and the refractory period of the cardiac conduction cycle. Beta blockers can be used for many cardiovascular issues such as heart failure, arrythmias, myocardial infarction, hypertension and angina.
Non-selective Beta-1 and Beta-2 include labetalol, propranolol, timolol, carvedilol, and sotalol. Selective Beta-1 drugs include acebutolol, metoprolol, bisoprolol and esmolol. Each med is used for slightly different purposes. For example, propranolol is used for many conditions such as hypertension, heart failure, MI, and arrythmias, whereas sotalol is used mostly for arrhythmias (Kabunde, 2023).
Beta-1 selective medications, such as metoprolol, that are used to treat hypertension will be reviewed in the Antihypertensive section later in this chapter.
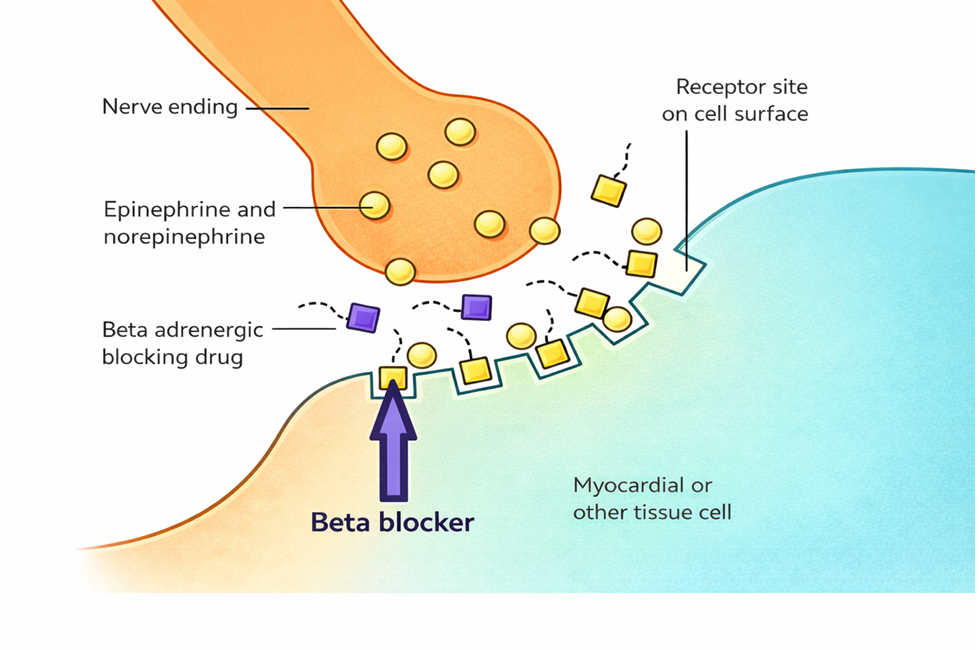
Recall… sympathetic adrenergic nerves release norepinephrine (NE) and epinephrine. Beta receptors bind NE that is released from sympathetic adrenergic nerves and also binds to NE and epinephrine that is circulating in the blood.
- Increases heart rate and blood pressure – this increases cardiac output and workload of the heart.
- Increases strength of heart contractions – this helps increase cardiac output
- Bronchodilation – bronchioles will dilate so breathing is easier and more oxygen enters the blood. More oxygen is needed as the myocardium needs it for this nervous system response
- Increases blood sugar – for energy via glycogenolysis in the liver.
Beta blockers will block many of these actions by competing for the binding site on beta-adrenergic nerves. This is helpful for conditions where the workload of the heart needs to be decreased or the heart is beating too fast.
Mechanism of Action
Non-selective beta-adrenergic antagonists block both beta-1 and beta-2 receptors. An example is propranolol. They will target the heart, kidneys, and lungs as well as the GI system and vascular smooth muscle. In the heart, they decrease the rate of automaticity, slow conduction velocity and prolong refractoriness. This results in a slower heart rate, PR interval lengthened, and the AV node transmits rapid atrial depolarizations at a lower frequency (Merck Manual, 2023).
Beta-1 adrenergic antagonist, as its name implies, selectively blocks only the beta-1 receptors so the effects are specific to cardiac cells. An example is metoprolol.
Our prototype medication will be sotalol. Sotalol is also a Class III antiarrhythmic with potassium channel blocking abilities and also has beta-adrenergic blocker properties.
Indications for Use
Class II drugs are used primarily to treat supraventricular tachycardias and to slow the ventricular response rates with atrial fibrillation or atrial flutter. Sotalol specifically is used for hemodynamically stable ventricular tachycardia and maintaining sinus rhythm is paroxysmal atrial fibrillation (Mubarik, Patel & Cassagnol, 2024).
Nursing Considerations
Administration: Oral or intravenous. Slow IV infusion to avoid hypotension. Peak effects for both IV and oral routes are similar, with oral route 2-3 hours and IV route 2 hours. Oral route BID dosing.
Oral administration – food or antacids will decrease absorption by up to 20%. Give on empty stomach
Pre-Treatment:
- Obtain full medical history and med profile.
- Baseline ECG, blood pressure and heart rate. If QTc is greater than 450 ms, drug will be held.
- Labs: renal (creatine clearance), electrolytes (normal se magnesium and potassium levels). If renal insufficiency, avoid using this med (Merck Manual, 2023).
Monitor:
- Monitor ECG and blood pressure. ECG assessed prior to therapy and 2-4 hours after each dose. Assess for QT prolongation.
- Apical pulse prior to dose. If less than 50 bpm, hold the med and consult with the prescriber. Check agency policy or orders for parameters with holding the med.
- Monitor electrolytes. Contraindicated with hypokalemia. Magnesium and potassium may be administered if low. May increase potassium levels and uric acid levels.
- Monitor blood glucose levels, may cause hyperglycemia.
- Anticipate client in the hospital for 2-3 days during dosage adjustments
- Monitor intake/urine output and daily weights. Assess for fluid overload (dyspnea, crackles, edema).
Contraindicated with bradycardia, 2nd or 3rd degree heart block, heart failure or conditions that lead to bronchospasm. Also, contraindicated with labile diabetes due to hypoglycemic effects.
Drug Interactions: calcium channel blockers, digoxin, clonidine.
Older adult: if renal insufficiency, dosage reduction required.
Genetic differences: some clients with Asian heritage metabolize and excrete propranolol faster and are also more sensitive to the drug. Caution with overdosage. Dose reduction of up to 50% and closer monitoring for adverse effects (Adams et al, 2019).
Adverse/Side Effects
Side effects:
- CV: Bradycardia, dizziness, fatigue, palpitations, cold hands/feet.
- Resp: Bronchospasm (contraindicated In clients with asthma)
- Other: hypoglycemia, thyroid abnormalities, erectile dysfunction
Adverse Effects:
- Bradydysrhythmias, heart failure, pulmonary edema
High Alert Med: This drug can cause arrhythmias. This medication lengthens a client’s QTc interval. Initiation of this medication requires a client to be in a facility to determine baseline QT and intermittent QT interval checks. QT interval checks are done 2-4 hours after each dose. If the QT corrected interval is greater than 500 msec, the dosing must be changed. Risk of Torsade de Pointes or new ventricular tachycardia/ fibrillation (Mubarik, Patel & Cassagnol, 2024).
Client Teaching
- Clients should be instructed regarding the significance of compliance with therapeutic drug regimens and should take medications as prescribed, even if not symptomatic.
- Clients or family members may need instruction on how to take pulse rate and blood pressure. They should receive parameters regarding reporting to their healthcare provider. They should report any pulse rate less than 50 bpm and significant changes in blood pressure.
- Inform client that meds can cause dizziness and visual changes. Clients may also notice orthostatic blood pressure decrease with position changes and should be advised to change positions slowly. If the client notices irregular, fast heart rate or experiences any fainting episodes, they should notify their healthcare provider immediately.
- May also mask the signs of hypoglycemia (no tachycardia or elevated BP), so diabetic clients must use extra caution to monitor for low blood sugar.
- Inform client of potential side effects, such as increased cold sensitivity.
- Inform health care provider if plan to take any new meds including OTC or herbal supplements.
- Do not abruptly discontinue med.
Unbound Medicine, n.d.; Vallerand & Sanoski, 2024.
Metoprolol Medication Card
Now let’s take a closer look at the medication card for metoprolol. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.

Downloadable file (.docx): Metoprolol Medication Card
Class III – Potassium Channel Blockers
Class III medications prolong repolarization by blocking the potassium channels in cardiac cells that are responsible for repolarization. They are used for emergency treatment of tachydysrhythmias. Amiodarone is an example of an antidysrhythmic that has predominantly Class III properties. Sotalol is also considered a class III med, with class II properties.
Mechanism of Action
Class III medications prolong repolarization by blocking the potassium channels in cardiac cells that are responsible for repolarization. By prolonging the refractory period, the QT interval is prolonged and makes the cell less excitable. They suppress tachyarrhythmias caused by re-entry mechanisms resulting in stabilization of the dysrhythmia (Klabunde, 2023).
Reentry Mechanisms in the heart
In very simple terms, reentry circuits are a condition due to a change in heart signaling. It is impaired conduction in the heart that can occur in a small region of the heart (local reentry) or it can occur between the atria and ventricles (global reentry). It can lead to very fast heart rates. Antiarrhythmic drugs or electrical cardioversion are given to alter the effective refractory period or conduction velocity or to eliminate reentry mechanisms.
To help understand this concept, watch the video: Cardiology: Re-entry Circuits #cardiology #ubcmedicine [9:02] by UBC Medicine – Educational Media (2017) on YouTube.
Our prototype medication will be amiodarone. Amiodarone also has sympatholytic, sodium and calcium antagonistic properties that decrease AV sinus node conduction (Patel & Goyal, 2024). It inhibits adrenergic stimulation.
Indications for Use
Amiodarone is used for many tachydysrhythmias that have not responded well to other antiarrhythmics. It is used for ventricular tachycardia, including ventricular fibrillation; atrial fibrillation and flutter. It has become the drug of choice for atrial dysrhythmias in clients with heart failure. It suppresses the arrythmia by 1. slowing the sinus rate, 2. increasing the PR and QT intervals, 3. decreasing peripheral vascular resistance, leading to vasodilation.
Pharmacokinetics:
Amiodarone is absorbed in the GI tract slowly. It is highly protein bound, distributed and accumulates in body tissues. It is metabolized by the liver and almost completely excreted in the bile. It has a very long half-life of 13-107 days.
Nursing Considerations
Administration: oral, IV or intraosseous (children). Depending on the rhythm (severity and type), oral or IV administration will be initiated.
- Oral: onset of action is 2-3 days, with a slow variable onset and a peak effect of 1-3 weeks. Duration of action can be months due to its long half-life. Give with meals to minimize GI upset.
- IV: onset of action is 2 minutes, with a peak effect 20 minutes. Typically, a loading dose (150 mg IV over 10 minutes) is followed by a continuous infusion (540 mg over the next 18 hours). The continuous infusion is then followed by oral administration. Amiodarone solution mixed in a glass bottle or polyolefin bottle to prevent absorption. IV tubing needs an in-line filter.
Pre-Treatment:
- Obtain full medical history and med profile.
- Labs: electrolytes (potassium, calcium and magnesium), liver panel and thyroid function. Correct hypokalemia and hypomagnesemia before therapy initiated.
- Baseline ECG, blood pressure and heart rate.
- Continuous ECG monitoring should be initiated.
Monitor:
- Monitor ECG continuously during IV therapy or initiation of oral therapy. Assess for rate and rhythm changes such as PR interval prolongation, slight QRS widening, T wave reduction or QT prolongation.
- Report any bradycardia or increase in arrythmia immediately. Rate reduction or discontinuation of drug may be required.
- Monitor blood pressure. Hypotension may occur in the first few hours after initiating therapy.
- Monitor electrolytes. Hypomagnesemia, hypokalemia or hypocalcaemia can decrease med effectiveness.
- Monitor liver function: if AST and ALT three times above normal, dose reduction likely.
- Assess respiratory function: report dyspnea, tachypnea, or crackles
- Long term: monitor thyroid function tests, assess for pulmonary conditions (interstitial pneumonitis), vision changes.
Pregnancy: Amiodarone can cause fetal injury when administered to a pregnant client.
Older Adult: Use cautiously in clients with decreased hepatic or cardiac function.
Drug Interactions:
Read drug label information carefully due to several potential drug interactions.
- Increases risk of increased QT prolongation with macrolides, fluoroquinolones
- Increases effects of digoxin 2-3-fold and other cardiac meds (i.e. Lidocaine)
- Increases effects of warfarin. Warfarin dosing should be decreased and INR monitored closely.
- St John’s Wort: may decrease the effects of amiodarone by inhibiting enzymes that metabolize it in the GI tract. Avoid St John’s Wort.
- Grapefruit juice will inhibit metabolizing enzymes in GI tract. Avoid use while on amiodarone.
Caution use with clients with heart failure, thyroid disease, coronary refractive laser surgery, severe pulmonary or liver disease.
(Adams et al, 2018; Kelly & Morgan, 2023; Vallerand & Sanoski, 2024)
Adverse/Side Effects
Side effects:
- Corneal microdeposits, photosensitivity, vision changes
- Neuro: tremor, confusion, dizziness, fatigue, peripheral neuropathy, poor coordination, gait issues.
- CV: bradycardia, hypotension
- GI: anorexia, constipation, nausea
Adverse Effects:
High Alert Med: Amiodarone has several fatal toxicities such as pulmonary toxicity, exacerbation of arrhythmia, liver injury, and heart block. Clients who require initiation of this therapy should be hospitalized and monitored closely in a critical care area.
Acute respiratory issues such as pulmonary fibrosis and acute respiratory distress syndrome. Frequent assessment for pulmonary toxicity (crackles, decreased breath sounds, pleuritic friction rub, fatigue, cough, hypoxia). Chest Xray q 3-6 months while on long term therapy.
CV: AV heart block, Prolonged QT interval (with potential for Torsade’s des Pointes)
(Adams et al, 2018; Kelly & Morgan, 2023; Vallerand & Sanoski, 2024)
Client Teaching
- Clients should be advised to closely follow the recommended dosing regimen. If one dose of medication is missed, the client should follow the normal dosing schedule and resume with the next dose. If more than one dose of medication is missed, the client should call the healthcare provider for guidance.
- Clients should be compliant with all follow-up appointments and monitoring.
- Monitor pulse daily. Report any changes.
- Clients should avoid drinking grapefruit juice during medication therapy.
- Some clients may experience photosensitivity and protective measures should be taken such as protective clothing and sunblock up to 4 months after therapy discontinues.
- Inform client of potential side effects and report to their health care provider any changes. Side effects may not appear for days, weeks or months.
Amiodarone Medication Card
Now let’s take a closer look at the medication card for amiodarone. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.

Downloadable file (.docx): Amiodarone Medication Card
Class IV – Calcium Channel Blockers
The class IV antiarrhythmics, calcium channel blockers, are widely used for cardiovascular disorders. These medications increase the refractory period of the AV node by slowing the influx of calcium ions, thus decreasing the ventricular response and the heart rate.
Calcium channel blockers can be divided into two distinct classes: one that blocks calcium channels in the heart, called non-dihydropyridines (verapamil, diltiazem) and the other that blocks calcium channels in the vascular smooth muscle, dihydropyridines (amlodipine, nifedipine). In this unit, we will examine the class that effects the heart and is used as an antiarrhythmic to control supraventricular tachycardias.
Later in this chapter, we will examine calcium channel blockers that relax the vascular smooth muscle and is used for hypertension. See the “Anti-hypertensives” section later in this chapter for more information.
Mechanism of Action
Diltiazem and verapamil both have a greater affinity to cardiac conduction cells. They decrease conduction velocity and slow the conduction through the AV node by binding to the L-type calcium channels on cardiac myocytes and cardiac nodal tissue. These channels regulate the influx of calcium into cells which stimulates muscle contraction and has a role in pacemaker currents and phase 0 of action potentials. When these calcium channels are blocked, the results are decreased myocardial force contractility (negative inotropy), decreased heart rate (negative chronotropy), and decreased conduction velocity (negative dromotropy), particularly at the atrioventricular node (Klabunde, 2023).
In this unit, our prototype drug will be diltiazem.
Indications for Use
Both diltiazem and verapamil are both equally effective. Both are used to treat arrythmias such as acute and chronic atrial fibrillation and atrial flutter, and other supraventricular tachycardias. Verapamil is more selective to the myocardium and is less effective as a systemic vasodilator drug. It is effective in treating angina (reversing coronary vasospasm and reducing myocardial oxygen demand) and treating arrythmias.
Diltiazem has more vasodilator actions, so it is also be used for hypertension (Klabunde, 2023). Other uses are to treat Raynaud’s syndrome, angina pectoris prophylaxis, migraine prophylaxis and pulmonary hypertension (Talreja & Cassagnol, 2023).
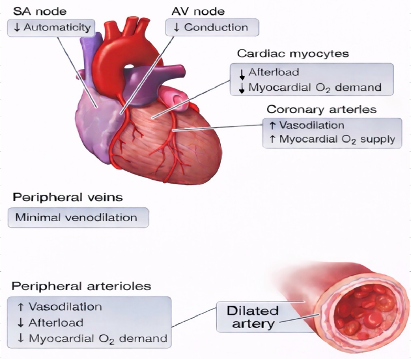
Calcium Channel Blockers:
Non-dihydropyridines: diltiazem and verapamil
| Cardiac Effects | Vascular Effects |
| ↓contractility | Smooth muscle relaxation
Vasodilation – ↓afterload, ↓myocardial oxygen demand
Venodilation – minimal venous tone effects
|
| ↓heart rate
|
slows the heart rate |
| ↓conduction velocity
|
the speed of the electrical impulses that travel through the heart will be slower. |
Nursing Considerations
Administration: oral and IV.
- Oral: Immediate release (IR), ER, CR formulas. IR onset of action 30-60 minutes.
- Metabolized by P450 enzymes and an inhibitor on CYP3A4, so drug interactions possible.
No dose adjustments for renal insufficiency. No dose adjustments with hepatic disease, unless severe.
Avoid with clients with hypotension (<SBP 90), acute myocardial infarction, conduction defects or clients with 2nd or 3rd-degree heart block or sick sinus syndrome.
Do not give concurrently with beta blockers as both meds depress cardiac electrical and mechanical activity.
Monitor:
- blood pressure before and after dose for hypotension.
- heart rate and ECG. Hold dose if apical rate lower than 50 bpm or per orders. Assess for ECG changes.
- Assess for chest pain: precipitating factors, quality, radiation, location, duration, severity.
- Assess for adverse effects such as signs of heart failure (SOB, edema, fatigue)
Adverse/Side Effects
Side effects: peripheral edema, bradycardia, dizziness, headache, and fatigue.
Adverse Effects: congestive heart failure, myocardial infarction, and hepatotoxicity.
- It can worsen signs and symptoms of heart failure due to the negative inotropic effect. Clients may experience bradycardia, worsening 1st degree AV block, syncope, hypotension.
(Talreja & Cassagnol, 2023)
Client Teaching
- Clients should be advised to closely follow the recommended dosing regimen.
- Clients or family members may need instruction on how to take a pulse rate and should report any pulse less than 50 bpm.
- Clients should also be advised that this medication may cause dizziness and visual changes.
- Clients may also notice orthostatic blood pressure decrease with position changes and should be advised to change positions slowly.
- Clients should be advised to avoid grapefruit juice during medication therapy.
- They should also monitor for gingival sensitivity and be sure to maintain good oral hygiene.
- Clients may also notice increased photosensitivity and should take protective measures.
To help with comparing the medications and to learn important considerations for each medication, refer to the Chapter 7 CV Medications anti-arrythmics and anti-anginals
Clinical Reasoning and Decision Making Learning Activities
A client has been started on a beta blocker: metoprolol a few months ago. What will be important assessments to evaluate the effectiveness of this med?
- A client is taking a beta blocker: propranolol for hypertension and they are now prescribed sulfonylurea as an additional diabetic treatment. Which is the best response to this treatment plan: (Choose the best answer)
- Propranolol will suppress the insulin release from the pancreas, and thereby decrease the sulfonylurea effect. The dose will need to be increased.
- Taking both meds will have a synergistic effect as they both have an effect on the pancreas, so decrease both dosages.
- Taking both meds will have little effect, except monitor blood sugar levels more closely.
- There is no concern with taking either of these medications except increased nausea if taken together.
- A patient is prescribed a Calcium Channel Blocker Non-D: verapamil. The nurse completes an assessment prior to administering the medication. What assessment finding would lead the nurse to hold the med and contact the prescriber?
- The nurse is providing some health teaching for a client taking a calcium channel blocker: Verapamil. What would be important dietary information the client should be aware of?
- A nurse is administering amiodarone with a client in ventricular tachycardia. What is an expected finding?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 7: Cardiovascular Medications Answer key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
References
Adams, M., Urban, C., El-Hussein, M., Osuji, J., & King, S. (2018). Pharmacology for nurses: A pathophysiological approach (2nd Canadian ed.). Pearson Canada.
Kelly, L., & Morgan, B. (2023). Amiodarone. London Health Sciences Centre. https://www.lhsc.on.ca
Klabunde, R. (2023). Antiarrhythmic drugs. Cardiovascular pharmacology concepts. https://cvpharmacology.com
Marian University. (2010, October 15). Beta-blockers: Function and effects. Marian University science blog. https://marianuniversityscienceblog.wordpress.com/2010/10/15/beta-blockers-function-and-effects/
MedlinePlus. (2026). Procainamide. U.S. National Library of Medicine. https://medlineplus.gov
Mubarik, A., Patel, P., & Cassagnol, M. (2024). Sotalol. In StatPearls. U.S. National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/
Patel, P., & Goyal, A. (2024). Antiarrhythmic medications. In StatPearls. U.S. National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/
Pritchard, B., & Thompson, H. (2023). Procainamide. In StatPearls. U.S. National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/
Talreja, O., & Cassagnol, M. (2023). Diltiazem. In StatPearls. U.S. National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/
UBC Medicine – Educational Media. (2017, February 14). Cardiology: Re-entry circuits #cardiology #ubcmedicine [Video]. YouTube. https://www.youtube.com/watch?v=yLI4yj1TZhc
Unbound Medicine. (n.d.). Unbound Medicine. https://www.unboundmedicine.com/ucentral
Vallerand, A. H., & Sanoski, C. A. (2024). Davis’s Canadian drug guide for nurses (19th ed.). F. A. Davis.
Media Attributions
- 7.5a Beta adrenergic blocker mechanism of action is adapted by Sheila Odubote, TRU Open Press, from MU Science Blog, 2010.
- 7.5b non-dihydropyridines calcium channel blockers effects on the heart and blood vessels is adapted by Sheila Odubote, TRU Open Press.
