6.5 Non-Steroidal Anti-Inflammatory Medication V2
Learning Objectives
- Describe the cyclooxygenase pathway and the mechanism of action of NSAIDs.
- Describe the primary effects and indications for use of acetaminophen, ASA and Ibuprofen, including important adverse effects and nursing considerations.
- Compare and contrast the NSAIDs: Ibuprofen, diclofenac, ketorolac and COX-2 inhibitor, celecoxib.
Non-Steroidal Anti-Inflammatory Medication (NSAIDs)
Non-steroidal anti-inflammatory medications are widely used for their analgesic, antipyretic and anti-inflammatory actions. They are used to treat mild to moderate pain for many conditions including headaches, general aches, dysmenorrhea, arthritis, and sprains. They are considered safe if used correctly and well-tolerated. As an OTC medication they are used extensively.
Although there are over twenty types of NSAIDs available in Canada, they all work similarly, and that is blocking the group of enzymes called cyclooxygenase (COX). The categories of NSAIDs we will examine are:
- Non-selective NSAIDs (COX 1 and 2 inhibitor):
- Acetylsalicylic acid (ASA)
- Ibuprofen, diclofenac, naproxen, ketorolac
- Selective NSAIDs (COX 2 inhibitor) – Celebrex
Acetaminophen is often discussed with NSAIDs as it has an effect on the cyclooxygenase pathway, although with notable differences and lacks anti-inflammatory properties. We will begin this unit with examining the cyclooxygenase inhibition.
What is cyclooxygenase?
Cyclooxygenase (COX) is responsible for the synthesis of prostaglandins and other related compounds (prostacyclin, thromboxane A2) of the inflammatory process. The immediate precursor of prostaglandins (PG), arachidonic acid, is derived from membrane phospholipids and is catalyzed by two COX enzymes, COX 1 and COX 2.
COX 1 is found in all tissues and is considered the housekeeping enzyme. It maintains homeostasis of organs. For example, it maintains gastric mucosa (increases bicarbonate, increases cytoprotective mucous in the stomach to provide a protective barrier and promotes submucosal blood flow), stimulates platelet aggregation (COX promotes synthesis of TXA2) and maintains renal blood flow through vasodilation.
COX-2 is the inflammatory enzyme and is considered inducible, meaning it is produced when there is tissue injury. When tissue is injured, it has a role in inflammation by promoting fibroblasts, leukocytes and macrophages to the injured area. COX 2 enzyme is more specific to the synthesis of PGs that cause pain and inflammation. It sensitizes receptors to painful stimuli. It is also present in the brain and mediates fever.
COX-2 also has a compensatory role. In health conditions where there is a compromised renal perfusion (heart failure, renal failure), COX-2 produces vasodilatory prostaglandins that increase blood flow and helps to preserve kidney function. In health conditions with compromised circulation, COX-2 also regulates renin release from the juxtaglomerular cells in the kidneys, helping to maintain blood pressure and sodium balance. Other non-inflammatory roles are it regulates female reproduction and bone formation (Rosenjack Burchum & Rosenthal, 2019; Qureshi, O. & Dua, A., 2024).
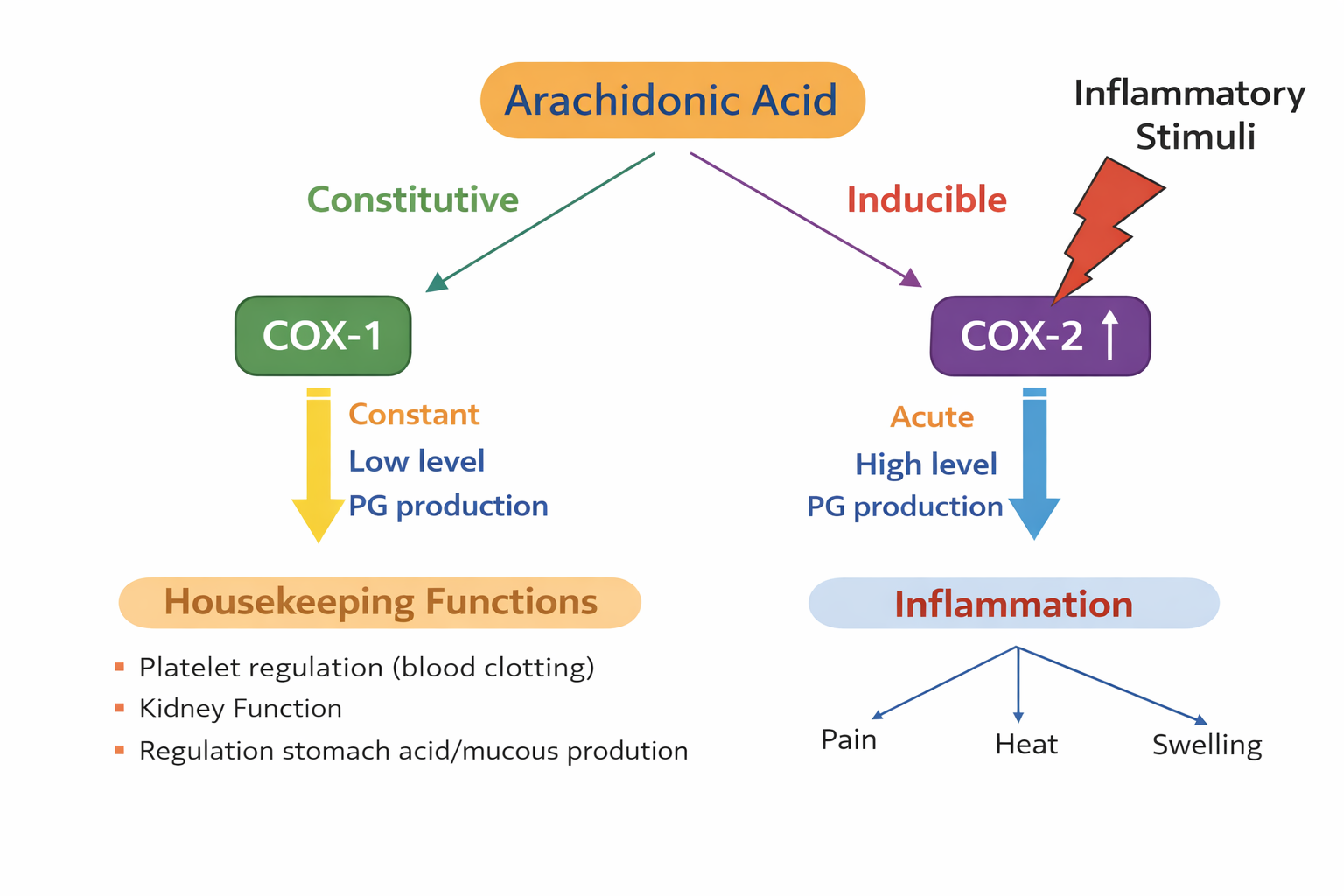
6.5a Cyclooxygenase Pathway. (Sheila Odubote/ TRU Open Press)
COX 1, the housekeeping enzyme, has a role in promoting renal blood flow, gastric mucosa acid protection, and platelet aggregation. COX 2, increases prostaglandins during an inflammatory process, leading to pain, heat and swelling.
So, what happens when COX 1 or COX 2 are inhibited by NSAIDs?
| Location | Type | COX Function | Effect of Inhibition by NSAIDs |
| Stomach | 1 | Gastric protection
↑bicarbonate, ↑mucous, ↓HCl |
Gastric irritation, ulcer formation |
| Platelets | 1 | Platelet aggregation | Risk of bleeding, ASA: protection against MI & TIA |
| Kidney | 1&2 | Maintains renal function:
↑renal vasodilation ↑renal perfusion |
Renal impairment
(vasoconstriction, ↓blood flow to kidney) |
| Injured tissue | 2
|
Inflammation and pain | ↓inflammation, analgesia |
| Brain/CNS | 2
|
Fever and pain | ↓fever, analgesia |
ASA and other NSAIDs relieve pain by inhibiting the biosynthesis of prostaglandin by different forms of the COX enzyme. As a result of the inhibition of COX-1 by an NSAID, there is decreased protection of the stomach lining, resulting in gastric irritation and bleeding. Further, there is an anti-platelet effect, particularly with ASA.
When COX-2 is inhibited, it results in the desired effects of decreased pain, swelling and fever. It can also decrease renal blood flow, along with COX 1 inhibition. For most clients, but this is only a concern if someone has renal impairment.
You can watch this video about the mechanism of NSAIDs.
Acetaminophen
Acetaminophen is a widely used analgesic and antipyretic medication, effective for treating mild-moderate pain and fever. It is available over the counter or it can be provided through prescription if combined with an opioid medication. It is referred to as paracetamol in many countries.
Mechanism of Action
The mechanism of Acetaminophen is still somewhat unknown. It inhibits the cyclooxygenase pathways and the synthesis of prostaglandins that serve as mediators of pain and fever primarily in the CNS (Frandsen & Pennington, 2018). Acetaminophen does not inhibit COX by binding to an active site of COX 1 or COX 2 (as with other NSAIDs), instead it appears to reduce the activity of COX through a pathway still not known. It also appears to inhibit the COX pathway in the central nervous system but not in peripheral tissues, thereby lacking any anti-inflammatory properties. For anti-pyretic effects, it acts directly on the hypothalamic heat-regulating center to cause vasodilation and sweating, to help dissipate the heat (RNpedia, 2025). Due to acetaminophen’s inhibitory action on COX, it is categorized as a non-steroidal anti-inflammatory drug that lacks anti-inflammatory properties (Gerriets et al, 2024).
Indications
Acetaminophen is used to treat mild pain and fever. It is also indicated for pain related to arthritis and rheumatic disorders however, it does not have anti-inflammatory properties.
It can be administered orally, rectally or intravenously. For the oral route, it comes in many formulations such as tablets, capsules or liquid form (syrup, suspension). IV route is rarely used and has not shown superior efficacy compared to oral or rectal routes (Gerriets et al, 2024).
It is safe for all ages, but dosing considerations are important to avoid the risk of hepatotoxicity.
Nursing Considerations
Taken as recommended, acetaminophen is a safe, well-tolerated medication. If dosage amounts are exceeded, or if the client has liver impairment or drinks alcohol in excess, then the risk of hepatotoxicity is a possibility.
Administration: oral or rectal.
- Oral route: rapidly absorbed orally, achieving peak plasma concentration in 30-60 minutes. Give drug with food if GI upset occurs.
- Rectal route: it bypasses first pass effect and is a good choice for clients NPO, dysphagia, or children who cannot manage oral administration.
- Metabolism: It is metabolized in the liver and excreted by the kidney, with 90% eliminated within 24 hours (Gerriets et al, 2024).
Health history prior to administration:
- Assess for chronic health issues: caution or contraindication for any client with impaired hepatic function, chronic alcoholism or renal insufficiency.
- Check allergy status for an allergy to the medication.
Monitor for effectiveness in lowering pain and fever.
If overdose or toxicity occurs, N-acetylcysteine is the antidote.
Pediatric clients:
The recommended dosage for children aged 2-12 is 12.5 mg/kg every 4 hours or 15 mg/kg every 6 hours. The maximum daily dose should not exceed 75 mg/kg. Weigh the child before administering to ensure accurate weight. Use a second nurse verifier for drug calculations.
Adults or adolescents over 50kg
The recommended dosage is 4000mg /day. Do not exceed 1000mg per dose with minimum dosing interval of 4 hours. Ie. 1000mg q 6 hours prn OR 650 mg q 4 hours prn.
Clients with hepatic impairment
If mild, dosage will be reduced. If sever liver impairment, it is contraindicated. Consult a health care prescriber with any client with liver impairment.
Clients with renal impairment
If creatinine clearance is less than 30mLs/min, then dosing intervals may be lengthened. Consult a health care prescriber.
Pregnancy
Acetaminophen is safe for pregnant clients. There have been some observational studies associated with prenatal acetaminophen exposure and the risk of neurobehavioural effects, but the current recommendations from the Government of Canada (2025) is that there is “no conclusive evidence that using acetaminophen as directed during pregnancy causes autism or other neurodevelopmental disorders.” Advise pregnant clients to take only as prescribed and if pain or fever last longer than five days, seek out health care provider advice. Acetaminophen is safe with breastfeeding.
Drug Interactions
For clients receiving warfarin for anticoagulant therapy, taking acetaminophen for a prolonged time at the maximum dosing, can lead to an elevated international normalized ratio (INR), resulting in increased risk of bleeding. Advise all clients on warfarin to check with their prescriber before taking acetaminophen for a prolonged period of time (Gerriets et al, 2024).
Overdose or Toxicity of Acetaminophen
N-acetylcysteine (NAC) is the only antidote.
In the early stages of overdose or toxicity, symptoms are often mild, with abdominal pain and nausea that can last 12-24 hours. If labs are drawn, AST/ALT will be elevated. After 24 hours, the client will become quite unwell with nausea, vomiting, jaundice, abdominal pain and hypotension. Management will include administering IV or oral N-acetylcysteine, but likely IV as vomiting is common. Other treatments will include airway management, IV fluids and vasopressors. Administering N-acetylcysteine within 24 hours of overdose is highly effective. NAS will prevent the hepatic metabolites from forming,
Acetylcysteine is also used as a mucolytic agent to thin viscous secretions.
(Ershad, M., Naji, A., Patel, P. & Vearrier, D., 2024)
Adverse Effects
As discussed, acetaminophen is a safe medication if used as recommended and if the client has no renal or liver dysfunction. Some clients experience a headache, rash, nausea or constipation. Hypersensitivity reactions may occur and include rash, fever or reddened skin.
Example in Practice: Safety with Acetaminophen
Some medications are combined with acetaminophen and are prescribed “as needed,” so the nurse must calculate the cumulative dose of acetaminophen over the previous 24-hour period.
Example 1:
Percocet 5/325 contains a combination of oxycodone 5 mg and acetaminophen 325 mg and could be ordered 1-2 tablets every 4-6 hours as needed for pain. If 2 tablets are truly administered every 4 hours over a 24-hour period, this would add up to 3900 mg of acetaminophen, which would exceed the recommended guidelines for a geriatric client and could cause liver damage.
Example 2:
A client had surgery and is discharged home with a prescription:
Tylenol #3 1-2 tabs q 4-6 hours as needed.
(Tylenol #3: Codeine 30 mg and acetaminophen 300 mg and caffeine 15 mg)
This client typically takes acetaminophen 975 mg three times a day for arthritic pain. They continue with this dose as well as take the Tylenol #3. If the client takes the Tylenol #3 to the maximum amount, this will be over the maximum dosing of 4000 mg /day and put the client at risk for overdose.
Client Teaching
Acetaminophen is well-tolerated and typically has few side effects if used as directed. Important considerations for clients include:
- Medications should be taken as directed and the dosing schedule should be adhered to appropriately. This is particularly important for pediatric and older adult populations.
- Pediatrics: available in rectal and oral formulation. Dosages are based on weight so ensure an accurate weight before dose. Follow the instructions on the package insert and ask for advice from a health care provider.
- Older adult: do not exceed 3200 mg /day, due to possibility of renal insufficiency, which may prolong the drug’s effects.
- Adults: recommended daily dose is 1000mg every 6 hours or 650 mg every 4 hours. Do not exceed 4000 mg/day.
- Avoid using other over-the-counter medications that include acetaminophen as overdosage will occur.
- Report a rash, unusual bleeding or bruising, yellowing of skin or eyes or a change in urination.
- Avoid drinking more than 3 or more alcoholic drinks every day while on this med. Risk of liver damage can occur (Vallerand & Sanoski, 2019).
- If you take acetaminophen for fever, if the fever lasts longer than three days or exceeds 39.5C, see your health care provider.

To prevent overdosing of acetaminophen, teach clients to not take Tylenol tablets along with any combined formulations that include acetaminophen. For example, cough and cold remedies.
Andrea’s note: Jessica -I retrieved this from wikepedia:
File:Extra Strength Tylenol and Tylenol PM.jpg This file is licensed under the Creative Commons Attribution-Share Alike 4.0 International, 3.0 Unported, 2.5 Generic, 2.0 Generic and 1.0 Generic license. 2008 https://commons.wikimedia.org/wiki/File:Extra_Strength_Tylenol_and_Tylenol_PM.jpg
Jessica / Tue Dec 16, 2025: @Copyeditor please find above the source of the image.
Acetaminophen Medication Card
Now let’s take a closer look at the medication card for acetaminophen (McCuiston, Vuljoin-DiMaggio, Winton, & Yeager, J., 2018; Vallerand & Sanoski, 2021). Medication cards like this are intended to assist students to learn key points about each medication. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication. Basic information related to each class of medication is outlined below.

Downloadable file (.docx): Acetaminophen Medication Card
Clinical Reasoning and Decision-Making Activity 1
Your client is admitted to the hospital with acute liver failure due to acetaminophen toxicity. Your client reveals that they have had a cold for several days and have been taking over-the-counter cold medications and acetaminophen for a headache. They also mention that every night after work they drink a “few” beers.
What client education about acetaminophen should be provided?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 6: Pain and Mobility Medications Answer Key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
NSAIDs: Acetylsalicylic Acid
Acetylsalicylic acid (aspirin) is a non-opioid NSAID analgesic and anti-pyretic. It is also used for its cardioprotective anti-platelet effects. ASA provides excellent pain relief especially for clients with conditions such as rheumatoid arthritis or other inflammatory health conditions.
Mechanism of Action
ASA irreversibly inhibits the blocking of COX-1 and COX-2 which results in blocking the synthesis of thromboxane 2 (TXA2). Thromboxane induces platelet aggregation leading to clot formation, constriction of blood vessels and plaque deposition. By blocking TXA2, platelets won’t clump together and vasodilation occurs leading to improved blood flow. Both these actions are beneficial for atherosclerotic vessels (Rosenjack Burcham & Rosenthal, 2019).
The irreversible inhibition is what sets ASA apart from other NSAIDs. Although it takes one hour post ingestion to block platelets, due to irreversible inhibition of COX, it is inhibited for the life of the platelet which is about eight days. This provides the sustained effect of inhibiting platelet aggregation after one dose. Other NSAIDs do not have this sustained effect and are not used for cardiac prevention.
Other ASA effects are inhibiting COX-2 and PG in the hypothalamus thereby decreasing fever. Inhibiting PG will have the anti-inflammatory and analgesic effects. ASA is a good choice for mild inflammation.
Indications for Use
ASA is used for the treatment of mild to moderate pain, fever, inflammatory conditions. The analgesic effects of ASA are mostly in the peripheries, and is ideal for joint and muscle pain and headaches. It does not treat visceral pain. ASA does well in lowering fever in adults by lowering the set point of the hypothalamus by inhibiting COX-2.
For clients with inflammatory conditions, ASA is a drug of choice. To suppress inflammation, larger doses are often prescribed than if treating pain or fever. For clients impacted with dysmenorrhea, ASA inhibits prostaglandins in the uterine smooth muscle.
Cardioprotective Effects
One of the beneficial effects of ASA is the thrombotic effects and is routinely recommended for clients at greater risk of myocardial infarction (MI) or stroke. This includes clients with ischemic stroke, transient ischemic attacks, acute MI and previous MI. It is also prescribed for higher risk clients as a primary prevention of MI (Rosenjack Burcham & Rosenthal, 2019). For anti-platelet effects, the dose of 81 mg once a day is sufficient, as higher doses will increase the risk of GI bleeding without more cardioprotective effects.
Colorectal and other Cancer Protection
The use of low dose ASA to decrease the risk of colorectal cancer has shown beneficial effects although the exact mechanism of action is still unclear. Some studies have found that “aspirin may prevent certain types of cancer through its immunomodulatory effects, regulating cellular metabolism, affecting DNA repair, reducing inflammation and preventing platelet activation” (Sun et al, 2025). In simpler terms, aspirin suppresses COX-1 formation of prostaglandins and also COX-2 suppression of tumorigenesis. COX-2 promotes tumour growth and metastases, so inhibiting this enzyme slows tumour growth. It has been shown that daily ASA reduces the risk of colorectal cancer (CRC) by 24% and CRC-associated mortality by 35% over an 8–10-year period (Garcia-Albeniz & Chan, 2012). For other cancers, low dose ASA has shown to reduce the risk of death in solid tumour cancers, 50% reduction in prostate cancer in men over 60, and in women, reduced the risk of breast cancer especially those with hormone receptor positive cancers (Rosenjack Burcham & Rosenthal, 2019). ASA is showing promise as an adjunct to other existing therapies such as immunotherapy and cytotoxic chemotherapy for the treatment of cancer progression and metastasis (Sun et al, 2025).
Dosages
- 81 mg po once a day – for cardioprotective effects. A larger does is not needed to inhibit platelet aggregation.
- 325-650 mg po q 4-6 hour (2600 mg/day) for pain and fever.
- 3000-4000mg per day for inflammatory conditions such as rheumatoid arthritis.
Nursing Considerations
ASA is rapidly absorbed in the small intestine after oral administration. ASA has a short life, converted to salicylic acid within 15-20 minutes. It is highly bound to albumin, and rapidly distributed to all body tissues. It is renally excreted (Rosenjack Burchem & Rosenthal, 2019).
Children
ASA is safe for most adults and children older than 14 years of age. It is contraindicated with children due to the risk of Reye’s syndrome. If a child needs analgesic or pain relief, then acetaminophen or ibuprofen can be used safely.
Pregnancy and Breastfeeding
ASA is not considered safe for pregnant women, especially after 20 weeks of pregnancy. It crosses the placenta, and can potentially cause low birth weight, still birth, and renal issues on the fetus. For the mother, it can suppress contractions, so need to avoid in the third trimester. It can also be found in breast milk and not recommended.
Older Adult
Older adults are more susceptible to negative GI and CNS effects of anti-inflammatories. If the client has renal insufficiency, then ASA will not be readily excreted, prolonging the duration of action.
Reye Syndrome is a rare but life-threatening illness that occurs almost exclusively in children, mostly in the age range 2-14 years of age. It usually begins after the child recovers from a viral infection, such as influenza or chickenpox, and is then characterized by symptoms of encephalopathy and fatty liver degeneration. The child rapidly worsens with symptoms of nausea and vomiting, confusion, seizures and loss of consciousness. It has been linked to the child taking ASA (salicylate) following a viral infection. Symptoms start 1-2 weeks after the child has recovered from the viral infection. Death occurs in 20-40% of the cases with children who survive are left with significant brain damage (Nemours KidsHealth, 2023).
Adverse/Side Effects
ASA is typically well tolerated but may cause toxicity, intolerance or hypersensitivity.
The most common adverse effects for gastric distress, heartburn and nausea. If taken with food or if the client uses enteric coated ASA, these effects can be minimized.
GI bleeding
GI bleeding is common and the client may experience dark, tarry stools. Typically the amount of bleeding is very minimal, but if on ASA for a long period of time, it may produce anemia. If the client is on ASA for a long period of time, even if low doses, the risk of gastric ulceration, perforation and bleeding is a possibility. The chance for bleeding is higher if a client:
- takes a higher dose or takes it for a longer time than directed
- takes other drugs containing prescription or nonprescription NSAIDs (aspirin, ibuprofen, naproxen, or others)
- has had stomach ulcers or bleeding problems
- takes a blood-thinning (anticoagulant) or steroid drug
- is age 60 or older
- smokes cigarettes
- has 3 or more alcoholic drinks every day while using this product
To minimize the risk of gastric ulcers, clients can take a proton pump inhibitor to reduce the hydrochloric acid in the stomach. Other meds such as histamine receptor antagonists or misoprostol are beneficial.
Contraindications
ASA is contraindicated if the client has a bleeding disorder such as hemophilia, vitamin K deficiency, or a recent history of bleeding in the stomach or intestine. High doses of ASA should be held prior to surgery for one week. It does not need to be held for minor procedures such as dental procedures (Rosenjack Burchem & Rosenthal, 2019).
Renal Impairment
Extra caution should be advised for clients at higher risk of impaired renal function from ASA use. ASA can cause irreversible renal impairment resulting in salt and water retention and edema. Clients most at risk are advanced age, history of renal insufficiency or liver impairment or heart failure.
Hypersensitivity reactions
Hypersensitivity reactions are less common, but are more likely with clients with a history of asthma, rhinitis and nasal polyps (Rosenjack Burchem & Rosenthal, 2019). This NSAID-induced respiratory disease begins within one hour of ingestion. Symptoms begin with diffuse watery rhinorrhea and can eventually lead to urticaria, bronchospasm and shock. This is not the same as an allergic reaction but due to the inhibition of COX-1 which triggers the production of leukotrienes. Clients who are allergic to any NSAID should not take aspirin as there is cross-reactivity.
Toxicity
If ASA levels climb above therapeutic levels, salicylism can occur. Cues can include tinnitus (ringing in the ears), sweating, headache, nausea and dizziness. If a mild case, then withhold ASA, and once symptoms reside, then ASA can resume but with smaller doses.
If severe, the client can experience hyperthermia, tachypnea, high anion gap metabolic acidosis, hypokalemia, seizures and cerebral edema. If these cases, salicylate toxicity is treated based on salicylate concentration, acid-base and electrolyte status (Arrif & Aggarwal, 2023).
Client Teaching
Clients should be made aware of the potential risks to avoid gastric distress, GI bleeding and other adverse effects.
- Use only the recommended dosage depending on the reason for use.
- Monitor for side effects such as nausea, gastric irritation, and occasional blood in stools. Report persistent symptoms such as ongoing bleeding or fever longer than 3 days.
- Monitor for adverse effects such as tinnitus and hold ASA until seen by their prescriber.
- If the client has asthma or rhinitis, be aware of hypersensitivity reaction cues such as diffuse watery rhinorrhea, itching and bronchospasm.
- Do not give ASA to children.
- If going for surgery, discuss with health care provider for the need to hold ASA one week prior to surgery.
- Avoid consuming alcohol greater than 3 drinks a day while on ASA
- Do not take ASA while pregnant. If taking ASA for inflammatory conditions, and under the supervision on their prescriber, ASA may be taken up to the third trimester.

Downloadable file (.docx): ASA Medication Card
Clinical Reasoning and Decision-Making Activity 2
A client asks why aspirin is given to prevent a heart attack or stroke. What is the nurse’s response?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the “Answer Key” sections at the end of the book.
NSAIDs: Ibuprofen
Ibuprofen is one of the most widely used pain reliever, anti-pyretic, and anti-inflammatory medications. Ibuprofen works by inhibiting COX-1 and COX-2 enzymes, leading to an inhibition of prostaglandin synthesis. See above for details about the mechanism of action. Other similar NSAIDs include naproxen, ketorolac, and indomethacin, which will be briefly discussed.
Indications for Use
Ibuprofen is used to treat mild to moderate pain and fever, inflammatory disorders including rheumatoid arthritis and osteoarthritis, and pain associated with dysmenorrhea. The route is oral, although it can be given intravenously in a hospital setting for clients who cannot take anything by mouth.
Nursing Considerations
Ibuprofen is a widely used, relatively safe medication if taken as instructed. It is used for all ages. Although a relatively safe medication, it has the potential for adverse effects. A thorough med profile, assessment and monitoring should be completed. For long term use, completing renal and hepatic panel, along with a CBC is recommended (Adams et al, 2019). Health conditions that may warrant further review before starting on NSAIDs include a history of alcoholism, congestive heart failure, peptic ulcer disease and renal disease.
Infants 6 months or older
Pregnancy
During pregnancy, women should consult with their health care provider to ensure the safety of taking NSAIDs during this time. If the benefit outweighs the risk, the lowest dose for the shortest period of time is recommended.
- Avoid first trimester due to increased risk of miscarriage and malformations
- Avoid after 20 weeks gestation as associated with fetal renal problems, low amniotic fluid, impaired lung maturation and limb contractures (Government of Canada, 2020).
- After 28 weeks gestation, there is an increased risk of premature closure of the fetal ductus arteriosus. Fetal and neonatal adverse effects affecting the brain, kidney, lung, skeleton, gastrointestinal tract and cardiovascular system have also been reported after prenatal exposure to NSAIDs (Antonucci et al, 2012).
Breastfeeding
Ibuprofen is safe for breastfeeding with negligible amount excreted in breast milk (NGO & Bajaj, 2024).
Older adult
Due to possible renal insufficiency in the older adult, Ibuprofen should be used at the lowest dose and for short periods. Monitor the client for indications of further renal impairment such as reduced urine output and elevation in serum creatinine and blood urea nitrogen (Rosenjack Burchum & Rosenthal, 2019).
Directions for use
NSAIDs are typically very well tolerated, especially if used as directed and for short term use. If taken on an empty stomach, it can cause gastric irritation. Take with food, although food will delay absorption and maximum effect (Ngo & Bajaj, 2024).
Drug Interactions
NSAIDs can interact with many drugs (Ngo & Bajaj, 2024; Rosenjack Burchum & Rosenthal, 2019).
- Anticoagulants: it can increase the risk of bleeding if taking warfarin, heparin or other anticoagulants
- ACE inhibitors:Ibuprofen may reduce the antihypertensive effects of ACE inhibitors.
- Lithium: it can increase the plasma levels of lithium by inhibiting renal PG synthesis, leading to lithium toxicity.
- Herbal supplements: taking certain supplements can increase the risk of bleeding, including garlic, ginger and gingko biloba. Ensure to ask about any supplements the client may be taking.
Adverse/Side Effects
Side effects: Although well tolerated, possible side effects include headache, constipation, dyspepsia, and nausea.
Adverse effects: For clients who take Ibuprofen on a regular basis or larger doses, the risk of adverse effects can occur.
- Gastric irritation, abdominal discomfort and the risk of GI bleed due to the decrease in prostaglandins role in maintaining a healthy gastric mucosa.
- Hypersensitivity reactions: clients with a history of asthma or rhinitis are more at risk for a reaction. Monitor for a rash. In severe reactions, anaphylaxis and reactions with eosinophilia and systemic symptoms (DRESS) can occur and often in relation to clients on other meds such as sulfa derivatives, antimicrobials or anticonvulsants (Ngo & Bajaj, 2024).
- Renal failure: NSAIDs decrease renal perfusion impacting renal function. If a client takes larger doses, uses Ibuprofen regularly, or takes one of the stronger forms of NSAIDs, a higher risk of renal failure can occur.
Box Warnings
- Cardiovascular thrombotic events: Ibuprofen increases the risk of serious cardiovascular events such as myocardial infarction and stroke. The risk is higher is the client takes more than is directed or takes it for longer than directed.
- Coronary artery bypass: Ibuprofen administration is not advised during the perioperative period for patients undergoing coronary artery bypass graft (CABG) surgery.
Stomach bleeding warning: The chance for bleeding is higher if the client:
- is age 60 or older
- has had a history of stomach ulcers
- takes an anticoagulant or steroid med
- takes other drugs containing prescription or nonprescription NSAIDs (aspirin, ibuprofen, naproxen, or others)
- has 3 or more alcoholic drinks every day while using this product
- takes a higher dose or for a longer time than directed
Client Teaching
- Consume the medication with a full glass of water and remain upright for 30 minutes following medication administration.
- Avoid the use of alcohol while taking this medication.
- Avoid using the medication for longer than 10 days on a regular basis.
- Monitor for a rash, visual changes, tinnitus, weight gain, or influenza-like symptoms, these should be reported to the healthcare provider immediately.[8]
NSAIDs: Ketorolac and Diclofenac
Other NSAIDs are often taken for inflammatory or analgesic purposes. Ketorolac and Diclofenac will be reviewed. Both have the same mechanism of action as already discussed.
Ketorolac
Ketorolac is an NSAID that is commonly used to treat “breakthrough” pain that occurs during the treatment of severe acute pain being treated with opioids. It is a powerful analgesic with minimal anti-inflammatory properties. Its analgesic effects are similar to opioids but without the adverse effects of respiratory depression or abuse potential.
Indications for Use
Ketorolac is indicated for the short-term (up to 5 days in adults) management of moderate to severe acute pain that requires analgesia at the opioid level. There is a higher risk of cardiac thrombotic events, renal failure, peptic ulcers and risk of bleeding if taken longer than 5 days. Give orally following IV or IM ketorolac.
Dosage
It can be give orally, nasal spray, IM or IV routes.
- Oral dosing: 10 mg q 4-6 hours prin
- IV/IM dosing: 60 mg x 1 or 30 mg q 6 hour prn
(Rosenjack Burchum & Rosenthal, 2019)
Example in Practice
A client comes to emergency department for severe lower back pain following over-exerting themselves doing physical work. After an assessment is completed, the physician writes the following order: Ketorolac 60 mg IM now. The RN administers the Ketorolac and the client is to be sent home with a prescription of Ketorolac 10 mg po q 4-6 hours prn x 5 days.
The client asks why they are given the IM dose first. The nurse explains that it is given to raise the blood levels of ketorolac quickly to achieve faster pain relief. The additional oral doses at home maintains the blood levels.
The nurse will be providing some instructions for the client. The nurse tells the client to use the med only as prescribed and not to take more than indicated. They should avoid using other NSAIDs such as ibuprofen to avoid adverse effects. They are to avoid drinking alcohol. If they develop a rash, blood in their stool, or abdominal pain, they need to return to the ED or see their health care prescriber.
Nursing Considerations
Ketorolac is safe for most adults. It is not considered safe for pregnant or breastfeeding women. In general, ketorolac should be avoided by older adults due to high risk of toxicity. If necessary for use in older adults, the dosage should be reduced. It can be given to children, with weight adjusted dosing.
Adverse/Side Effects
As Ketorolac is a stronger formulation than Ibuprofen, the adverse effects are more of a concern, and as such, this med is for short term use only. Adverse effects listed for Ibuprofen also pertain to ketorolac. Adverse effects include drowsiness, headache, GI bleed, abnormal taste, dyspepsia, nausea, Stevens-Johnson syndrome, edema, and renal failure.
It is contraindicated if active peptic ulcer disease. Older adults are at greater risk of adverse effects.
Client Teaching
- Along with the previously discussed side/adverse effects, ketorolac may cause dizziness or drowsiness.
- Avoid alcohol or other aspirin-containing products unless directed by their healthcare provider.
- If the client notices rash, visual changes, tinnitus, weight gain, or influenza-like symptoms, these should be reported to the healthcare provider immediately.
Mahmoodi, Patel & Kim, 2024; Rosenjack Burchum & Rosenthal, 2019)
Diclofenac
Diclofenac is used to treat pain and inflammation related to inflammatory disorders such as rheumatoid arthritis and ankylosing spondylitis. It also is used to treat dysmenorrhea, migraines and mild-moderate pain related to sprains.
Dosing: Diclofenac can be taken orally, topical ointment, transdermal or suppository.
- Acute pain: 18-35 mg TID
- Inflammatory conditions: 35 mg TID
- Dysmenorrhea or post-partum: suppository route is an option for localized effect.
- Pain due to sprains/strain: Topical ointment for localized effect. Potential risk for dry skin or contact dermatitis.
All side and adverse effects, contraindications and drug interactions for NSAIDs apply to diclofenac.
NSAID: Celecoxib
Celecoxib is a COX-2 inhibitor and the only drug in this class available in Canada. It was developed under the premise that inhibiting COX-2 only to achieve the analgesic, anti-inflammatory effects would be more beneficial than also inhibiting COX-1 which causes the gastric irritation and anti-platelet effects. Unfortunately, other versions of COX-2 inhibitors caused a double-fold increase in the risk for myocardial infarction and stroke, especially if taken for a long duration of action. As of 2004, only celecoxib is available.
Mechanism of Action
Celecoxib specifically inhibits the enzyme COX-2 that is required for the synthesis of prostaglandins.
Indications for Use
Celecoxib is used to treat the pain associated with osteoarthritis, rheumatoid arthritis (including juvenile), and ankylosing spondylitis. It also relieves the pain associated with dysmenorrhea.
Nursing Considerations
- Celecoxib is considered safe for children 2 years or older.
- Dosage adjustment is required for clients with hepatic impairment (see Box Warning). Monitor AST and ALT levels.
- Labs: may cause hypophosphatemia, hyperkalemia and increased BUN.
- Contraindicated for use during pregnancy, especially after 20 weeks due to risk of fetal renal impairment.
- Older adults are more susceptible to negative side-effects of anti-inflammatories.
- Use cautiously with clients with cardiovascular disease, as risk of MI or stroke increases.
Adverse/Side Effects
Adverse effects are similar for all NSAIDs. Adverse effects include hypertension, peripheral edema, increased liver enzymes, abdominal pain, dyspepsia, gastroesophageal reflux disease, vomiting, and diarrhea.
Gastrointestinal Bleeding, Ulceration, and Perforation: NSAIDs cause an increased risk of serious gastrointestinal (GI) adverse events including bleeding, ulceration, and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms.
High Alert Med: Increased risk of cardiovascular (CV) events and gastrointestinal bleeding, ulceration, and perforation. Health Canada has also issued a safety review of celecoxib (Health Canada, 2016). Celecoxib can cause an increased risk of serious cardiovascular thrombotic events, including myocardial infarction and stroke, which can be fatal. This risk may occur early in the treatment and may increase with duration of use. Celecoxib capsules are contraindicated in clients who have recently received coronary artery bypass graft (CABG) surgery.
Client Teaching
Clients should take medication as directed and use the lowest effective dose for the shortest period of time. If signs of GI toxicity occur, these should be reported immediately to the healthcare provider.
Advise client to not take other NSAIDs while on celecoxib, as increased risk of GI effects.

Downloadable file (.docx): NSAID Medication Card – CH 6.5
Interactive Learning Activities
Clinical Reasoning and Decision Making Learning Activities 3
- A client who is a chronic alcoholic asks if it is okay to take ibuprofen for knee pain. What is the nurse’s best response?
- Ketorolac IV was administered to a client for severe pain (rated as “8”) due to a back injury. When should the effectiveness of the medication be evaluated?
- A client has been prescribed celecoxib for their arthritic pain. What client teaching does the nurse plan to provide?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the “Answer Key” sections at the end of the book.
References
Arrif, H. and Aggarwal, S. (2023). Salicylic Acid (Aspirin). National Library of Medicine. StatPearl [Internet]. Salicylic Acid (Aspirin) – StatPearls – NCBI Bookshelf
Antonucci, R., Zaffanello, M., Puxeddu, E., Porcella, A., Cuzzolin, L., Pilloni, M., & Fanos, V. (2012). Use of non-steroidal anti-inflammatory drugs in pregnancy: impact on the fetus and newborn. Current Drug Metabolism, 13(4):474-90. doi: 10.2174/138920012800166607.
Ershad, M., Naji, A., Patel, P. & Vearrier, D. (2024, February). N-Acetylcysteine. National Library of Medicine. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK537183/
Frandsen, G. & Pennington S. (2018). Abrams’ clinical drug: Rationales for nursing practice (11th ed.). (pg.305, 310, 952-953, 959-960) Wolters Kluwer. ↵
Garcia-Albeniz, X. and Chan, AT. (2012). Aspirin for the prevention of colorectal cancer. Best Practice Research in Clinical Gastroenterology, 25(0), 461-472. doi: 10.1016/j.bpg.2011.10.015 Aspirin for the prevention of colorectal cancer – PMC
Garriets, V., Anderson, J., Patel, P., Nappe, T. (2024, Jan). Acetaminophen. National Library of Medicine. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK482369/
Government of Canada (2020). Use of non-steroidal anti-inflammatory drugs beyond 20 weeks of pregnancy and risk of kidney damage in unborn babies, leading to low amniotic fluid. Recall and Safety Alert. Use of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) beyond 20 weeks of pregnancy and risk of kidney damage in unborn babies, leading to low amniotic fluid – Canada.ca
Government of Canada (2025, Sept 23). Acetaminophen is a recommended treatment for fever and pain during pregnancy. Public Advisory. https://recalls-rappels.canada.ca/en/alert-recall/acetaminophen-recommended-treatment-fever-and-pain-during-pregnancy
Health Canada. (2016). Summary Safety Review – Celecoxib – Assessing the Risk of Serious Heart and Stroke Side Effects at High Doses Relative to Other Non-Steroidal Anti-Inflammatory Drugs (NSAIDs). https://www.canada.ca/en/health-canada/services/drugs-health-products/medeffect-canada/safety-reviews/summary-safety-review-celebrex-generics-assessing-risk-serious-heart-stroke-high-doses.html ↵
Mahmoodi, A., Patel, P. & Kim, P. (2024). Ketorolac. National Library of Medicine. StatPearls.https://www.ncbi.nlm.nih.gov/books/NBK545172/
McCuiston, L., E., Vuljoin-DiMaggio, K., Winton, M., B., & Yeager, J. (2018) Pharmacology: A patient centered nursing process approach (pp. 268-270, 324, 332) Elsevier. ↵
Nemours KidsHealth (2023). Reye syndrome. Nemour KidsHealth. Reye Syndrome | Nemours KidsHealth
Ngo, V. & Bajaj, T. (2024). Ibuprofen. National Library of Medicine. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK542299/
Qureshi, O. & Dua, A. (2024, February). Cox Inhibitors. National Library of Medicine. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK549795/
RNPedia. (2021). Acetaminophen nursing considerations and management. https://www.rnpedia.com/nursing-notes/pharmacology-drug-study-notes/acetaminophen-n-acetyl-p-aminophenol/ ↵
Rosenjack Burchum, J., & Rosenthal, L. (2023). Chapter 21: Cyclooxygenase inhibitors. Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada.
Sun, M., Yu, J., Wan, J., Dou, X., Chen, X. Ye, F. (2025). Role of aspirin in cancer prevention. Cancer Treatment and Research Communications, 43, 100184. Role of aspirin in cancer prevention – ScienceDirect
Vallerand, A., & Sanoski, C. A. (2019). Davis’s Drug Guide for Nurses (16th ed.). F.A. Davis Company.

{kind=link}
{kind=link}