5.4 CNS Depressants
CNS depressants slow down brain activity, resulting in muscles to relax and an overall calming and soothing effect for that person. CNS depressants are used to treat anxiety, seizures, insomnia and panic attacks. Medications in this category include barbiturates, benzodiazepines, inhalants, and sleep aids. Even alcohol is considered a CNS depressant.
Depressants can be considered either an anxiolytic (anti-anxiety agents) or a hypnotic, but the difference is often only the dosage. As such depressants can also be called sedative-hypnotics. Anxiolytics are used to relieve anxiety and have a lower prescribed dosage. Conversely, hypnotics are used to promote sleep and have a higher dosage.
Along with benzodiazepines, there are a variety of sleep aids or hypnotics available. This unit will briefly discuss benzodiazepine-type medications (zolpidem, eszopiclone). Other hypnotics include antidepressants (trazadone or doxepin), antihistamines (diphenhydramine) and melatonin.
Other depressants not covered in this unit include inhalants. Nitrous oxide, an inhalant, is used for medical or dental procedures for its anxiolytic and analgesic effects. Nitric oxide (NO) is mixed with oxygen and delivered via face mask in controlled settings such as clinics or a hospital.
In this unit, we will cover barbiturates and benzodiazepines.
Barbiturates
Barbiturates have a long history, first developed in 1864 by Dr. von Baeyer, but it took until 1904 where it was used for psychiatric and neurological disorders. During the earlier half of the 20th century, it was used to induce sleep in psychotic patients, prescribed to treat insomnia and anxiety, and to reduce the number and intensity of seizures. By the 1960s and 1970s, barbiturate use declined due to serious adverse effects of dependence and risk of overdose, ultimately leading to more regulation with restricted prescriptions. At the same time, the development of benzodiazepines occurred and are now widely used (López-Muñoz, Ucha-Udabe, Alamo, 2005). Although the use is more limited, barbiturates are still used to treat seizure disorders, neonatal withdrawal, preoperative anxiety, anesthesia induction, and the induction of coma to address increased intracranial pressure (ICP) (Skibiski, Patel & Abdijadid. 2024).
Our prototype med will be Phenobarbital, which is primarily used as a sedative and to treat seizure disorders (raises the seizure threshold). In high doses, it can be used to induce anesthesia, and overdosage can cause death. Barbiturates are controlled substances under the Pharmacy Operations and Drug Scheduling Act. However, the misuse of barbiturates continues to occur with street use as a “downer” to counteract the effect of cocaine and methamphetamine.
Mechanism of Action
Normally, GABA inhibits activity in the brain leading to a calming effect. GABA is the primary inhibitory NT that reduces neuronal excitability, thereby it monitors and controls the amount of stimuli getting into the brain. If there is a disorder in GABA signaling, more impulses can lead to overstimulation, disordered thinking etc. and is the basis of some psychiatric conditions.
GABA’s role in the Brain: An analogy is a security guard at a night club. The security guard allows only so many people into the nightclub so it is more controlled and calmer. GABA has a similar effect on the brain. Not all stimuli or signals get through. A disorder in GABA signalling is basis of many psychiatric conditions.

Barbiturates bind to GABA receptor-chloride channel complex keeping the chloride channel open, resulting in both enhancing the inhibitory actions of GABA and also directly mimicking the action of GABA. They depress the whole CNS by potentiating the effects of GABA.
Barbiturates have a greater effect on the chloride channel than benzodiazepines as they work to open the chloride channel even in the absence of GABA. Along with the GABA effects, barbiturates also block AMPA and NMDA receptors, a subtype of glutamate receptor. Recall that glutamate is an excitatory neurotransmitter (DrugBank, 2026). When glutamate receptors are blocked, this further reduces CNS activity. Barbiturates not only enhance the inhibition of GABA but also block excitation, resulting in a strong overall effect compared to other sedative-hypnotic meds.
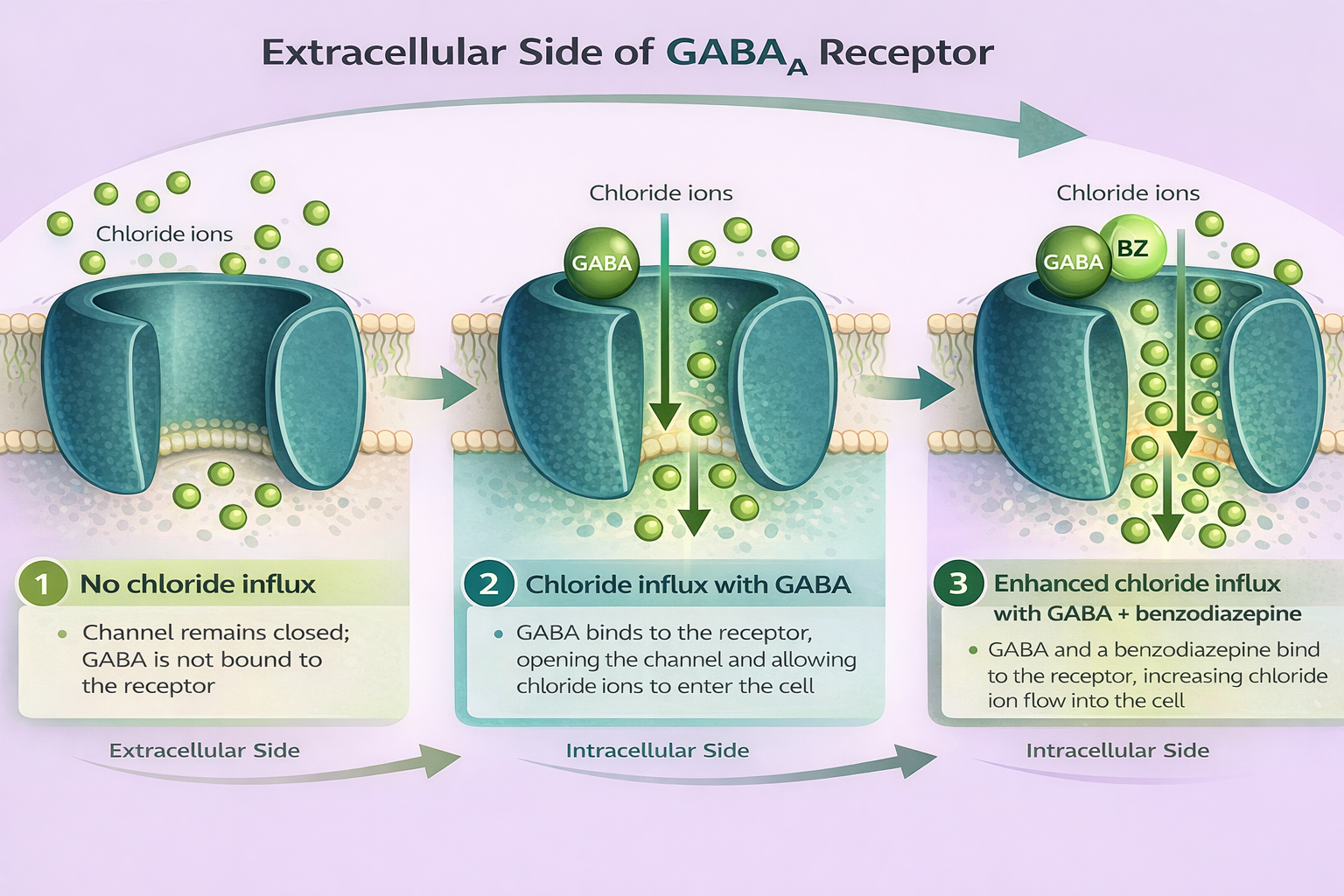
Figure 5.4a: Extracellular view of GABAa receptor (Sheila Odubote/ TRU Open Press)
The first image shows Chloride channel with GABA not bound to the receptor. The second image the chloride channel opening with the binding of GABA to the receptor and the influx of chloride cells. The third image shows the chloride channel opening with GABA and BZ binding to receptors, allowing a greater influx of chloride cells.
Indications for Use
There are three different groups of barbiturates which are based on the duration of action. We will focus our discussion on phenobarbital, but the other meds are used for comparison.
- Methohexital, thiopental: ultra short acting (30 seconds, duration 20 minutes). Used for anesthesia induction. Could also be used for procedural sedation, but less used for this purpose.
- Secobarbital: short-intermediate acting (onset 10 minutes with duration 3-4 hours). Used for insomnia or to induce sedation with medical assistance in dying (MAID).
- Phenobarbital: long acting (onset 30 minutes, duration up to 10-12 hours). Muscle relaxant, anticonvulsant. Can be used for alcohol withdrawal if other meds not effective.
The drug absorption depends on the lipid solubility of the drug and route of administration. The more lipid soluble, the faster onset and shorter the duration of action. It makes sense that methohexital is used for the induction of anesthesia, as it works very quickly and has a short duration of action. Whereas phenobarbital has a longer duration of action which would be beneficial in seizure management (Skibiski, Patel & Abdijadid. 2024; Vallerand & Sanoski, 2024).
Pharmacokinetics
Phenobarbital is rapidly absorbed orally or intravenously. It is distributed to all tissues including the brain, liver, skeletal muscles and kidneys. It crosses the blood brain barrier rapidly. It is metabolized by the liver through the P450 enzymes, and advanced age, chronic liver disease or drug interactions may decrease metabolism (Skibiski, Patel & Abdijadid. 2024). With repeated administration, tolerance develops due to the self-induced increase in barbiturate metabolism. Due to the high lipid solubility and subsequent distribution to fatty tissues, the sedative effects can take a long time as they are slowly released from the tissues.
Nursing Considerations
- Administered oral, IV, IM. If the oral dose is taken with food, absorption may be delayed. A loading dose may be given due to long t ½ to reach steady state.
- Nursing assessment: monitor vital signs (RR, oxygen sats, HR, BP) and respiratory status.
- For seizure management: assess location, duration and characteristics of seizure activity
- Assess level of consciousness, sedation levels and pain.
- Fall risk: supervise ambulation and use fall precautions.
- Pregnancy: readily crosses the placental barrier and can lead to fetal malformations. If methohexital is used for the induction prior to a caesarean delivery, the infant may have respiratory depressions (Skibiski, Patel & Abdijadid. 2024).
- Older Adult: avoid use with the older adult due to the likelihood of more pronounced depressive effects. Lower dosage and monitor closely for CNS changes, respiratory depression and fall risk.
- Contraindicated for use in clients with severe renal and hepatic disorders, severe respiratory depression, dyspnea or airway obstruction, and porphyria.
Drug Interactions:
Barbituates interact with many other drugs.
- Vitamin D: absorption interfered, so need to supplement to avoid osteomalacia.
- Vitamin K: enzyme induction leading to increased metabolism of vitamin K dependent clotting factors, resulting in an increased risk of bleeding.
- Barbiturates are enzyme inducers within the liver, so some drugs will be metabolized faster. Increased dosages and closer monitoring for meds such as warfarin, oral contraceptives, glucocorticoids.
- Synergistic effect with alcohol, antihistamines, opioids.
(Rosenjack Burchum & Rosenthal, 2019; Vallerand & Sanoski, 2024)
Side and Adverse Effects:
Side effects: similar to benzodiazepines and include:
- Drowsiness is common, especially with initiating therapy.
- Cognition: Mild impairment of concentration, judgment, memory may occur. Other: sleep disturbances, dizziness, headache, depression, poorly controlled pain, slowed reflexes, slurred speech.
- Paradoxical effects include euphoria, confusion, delirium, increased pain intensity
- GI upset (nausea, vomiting, diarrhea) and rashes, urticaria.
High Alert Med: Barbiturates is a high alert med, as there is no ceiling effect. Overdoses can cause unconsciousness, coma and death (Rosenjack Burchum & Rosenthal, 2019; Vallerand & Sanoski, 2024)
- CNS effects: drowsiness, CNS depression, coma
- CV effects: lowers heart rate, hypotension. If given in higher doses, can lead to depressed myocardium and vascular smooth muscle, resulting in shock.
- Resp effects: decrease in respiratory rate. It depresses the brain stem respiratory drive and depresses the chemoreceptors that control respirations, leading to respiratory depression.
Paradoxical responses can occur. In children, may see hyperactivity, behavioural and cognitive impairment. In the older adult, may see confusion, excitation or depression. Reduced dosages required.
There is no antidote, supportive measures only in overdose.
Client Teaching
- Take the prescribed medication as directed.
- Clients who undergo prolonged therapy should not discontinue treatment abruptly as this may cause the onset of seizure activity.
- These medications may cause drowsiness and should not be taken with alcohol or other CNS depressants.
- Female clients using oral contraceptives should also use non-hormonal-based contraceptives during therapy involving barbiturate use.
- Habit forming: High risk of tolerance and dependence. Overdose can cause respiratory depression and can be fatal.
- Overdose: the onset of symptoms following a toxic oral exposure to phenobarbital may not occur until several hours following ingestion. If an overdose occurs, consult with a Poison Information Center (1-800-567-8911).
Phenobarbital Medication Card
Now let’s take a closer look at the medication grid for phenobarbital in Table 8.5a (Rosenjack Burchum & Rosenthal, 2019; Vallerand & Sanoski, 2024). Medication cards like this are intended to assist students to learn key points about each medication. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.

Downloadable file (.docx): Phenobarbital Medication Card
Benzodiazepines
Benzodiazepines (BZD) were first produced in the 1950s and are still widely used today. They are the drug of first choice for anxiety and sedation, along with benzodiazepine-like medications. BZD are considered safer than many of the alternative CNS depressants.
Benzodiazepines are widely used for a variety of health conditions including anxiety disorders, panic disorders, seizures, procedural sedation and alcohol withdrawal.
Indications for Use
All beneficial effects of benzodiazepines are the result of depressant actions in the CNS. It is used for sedation, anti-anxiety, and anticonvulsant effects. Lorazepam injection is indicated for the treatment of status epilepticus. It may also be used in adult clients for pre-anesthetic medication to produce sedation (sleepiness or drowsiness), relieve anxiety, and decrease the ability to recall events related to the day of surgery. Lorazepam, either oral or IV, is used as a first line treatment for alcohol withdrawal.
Off label, BZD are also used for Tourette syndrome, delirium, sleep disorders and adverse movement effects (tics, tardive dyskinesia, tremors) caused by some meds (Bounds & Patel, 2024).
There are numerous benzodiazepines and they are used for slightly different purposes. Each medication differs in potency, onset of action and duration. Some of the conditions and type of BZD are listed below.
Anxiety disorders (anxiolytic)
- Alprazolam
- Diazepam
- Lorazepam
Insomnia
- Lorazepam
- Triazolam
Seizures (anticonvulsant)
- Diazepam
- Lorazepam
- Clonazepam
Alcohol Withdrawal
- Diazepam
- Lorazepam
Conscious sedation
- Midazolam
- Diazepam
Our prototype med will be lorazepam.
Mechanism of Action
Benzodiazepines bind to specific GABA receptors to potentiate the effects of GABA, an inhibitory neurotransmitter within the CNS. These receptors (GABA-A) are proteins that collectively shape a chloride channel in the centre. When BZD bind to and activate the BZD receptor, it increases the frequency of the GABA-A receptor chloride channel opening in the presence of GABA (allosteric effect), leading to neuron hyperpolarization and reducing nerve firing for the calming and sedative effects. If there is no GABA present, the Cl- channel would not open, and the sedative effects would not occur (Bounds & Patel, 2024; Rosenjack Burchum & Rosenthal, 2019).
Watch the short video to learn more about the MOA of benzodiazepines.
Neuroscientifically Challenged (n.d.). 2-Minute Neuroscience: Benzodiazepines. Youtube: 2-Minute Neuroscience: Benzodiazepines
Pharmacokinetics
Benzodiazepines are well absorbed after administration. They easily cross the blood brain barrier due to their high lipid solubility and are distributed rapidly. Most BZD undergo extensive metabolic alterations and are metabolized by hepatic enzymes CYP3A4 and CYP2C19. Although there are some differences between each BZD drug, most metabolites are pharmacologically active. This results in the BZD effects persisting much longer than the parent drugs half-life. For example, flurazepam whose plasma half life is 2-3 hours, its active metabolite half-life is 50 hours. Therefore, the effects of flurazepam lasts much longer. All are eliminated by the kidney (Bounds & Patel, 2024).
Nursing Considerations
Administration: mostly oral or IV routes, but can also be given IM, rectal or nasally.
- Should be prescribed for short periods only (e.g., 2 to 4 weeks). Treatment period should not be extended without re-evaluation of the need for continued therapy.
- Taper dosages to avoid withdrawal symptoms. May need to taper over weeks or months for long-term therapy.
- IV administration: risk of adverse effects is higher than with oral dosing, especially respiratory depression. In the event of respiratory depression, maintain a patent airway and ventilatory support as needed. The additive central nervous system effects of other drugs, such as phenothiazines, narcotic analgesics, barbiturates, antidepressants, scopolamine, and monoamine-oxidase inhibitors should be considered when these other drugs are used concomitantly with, or during the period of recovery from lorazepam injection.
Pregnancy: Benzodiazepines may cause fetal harm when administered to pregnant women. Children and the elderly are more likely to experience paradoxical reactions to benzodiazepines such as tremors, agitation, or visual hallucinations.
Elderly or debilitated clients may be more susceptible to the sedative and respiratory depressive effects of lorazepam. Therefore, these clients should be monitored frequently and have their dosage adjusted carefully according to the client’s response; the initial dosage should not exceed 2 mg.
Hepatic insufficiency: Dosage for clients with severe hepatic insufficiency should be adjusted carefully according to client response.
Adverse/Side Effects
Most benzodiazepines are relatively safe and well tolerated. The side effects are usually mild, and not noticed if the drug is used in low doses. Clients may experience drowsiness, dizziness, headache, nausea or vomiting, diarrhea and loss of balance.
Adverse effects are dose dependent and more likely with IV administration.
CNS:
- Low doses: drowsiness, sedation, dizziness, hang over effects, loss of balance
- High doses: confusion, disorientation, anterograde amnesia, hypotension
RESP: Low risk of respiratory depression. If given IV, can cause respiratory depression by inhibiting respiratory drive.
Adverse effects: visual disturbances such as diplopia, cyclic eyelid movement, loss of balance, and difficulty focusing eyes can occur.
High Alert Med: concomitant use of benzodiazepines and opioids may result in profound sedation, respiratory depression, coma, and death.
Paradoxical effects: when used for anxiety, can cause paradoxical effects such as insomnia, excitation, euphoria and heightened anxiety (Rosenjack Burchum & Rosenthal, 2019). This response is seen more often in children and older adults.
Benzodiazepines are on the Beer’s Criteria due to the higher risk of adverse effects and higher incidence of falls in the older population. It is recommended to avoid BZD in the older adult for insomnia or anxiety. It is acceptable to use BZD for alcohol withdrawal or severe generalized anxiety disorder unresponsive to other therapies (Canadian Geriatrics Society, 2025).
Physical and Psychological Dependence:
- Tolerance can develop if used for antiseizure, sedative or anxiolytic effects. Physical and psychological dependence may occur with long-term use. When discontinuing, may see mild withdrawal symptoms (anxiety, sweating, tremors, dizziness).
- Withdrawal from long term high-dose therapy or abrupt cessation can cause more significant symptoms such as panic, paranoia, hypertension, muscles twitches or convulsions.
Overdose
- Overdosage of benzodiazepines is usually manifested by varying degrees of central nervous system depression, ranging from drowsiness to coma.
- Treatment of overdose:
- It is mainly supportive until the drug is eliminated from the body.
- Vital signs and fluid balance should be carefully monitored in conjunction with close observation of the client.
- An adequate airway should be maintained and assisted respiration used as needed.
- Flumazenil, a benzodiazepine antagonist, may be used for hospitalized clients. There is a risk of seizure in association with flumazenil treatment, particularly in long-term benzodiazepine users (Bounds & Patel, 2024, Vallerand & Sanoski, 2024).
Antidote Flumazenil
Flumazenil is a competitive benzodiazepine receptor antagonist. It will reverse sedation but has variable effects on respiratory depression. It also carries a seizure risk. Administered IV, and given in incremental doses, repeated every minute, up to a total dose of 3 mg. duration of action is one hour, and may be repeated.
Client Teaching
- Clients who receive lorazepam should be cautioned that driving a motor vehicle, operating machinery, or engaging in hazardous or other activities requiring attention and coordination should be delayed for 24 to 48 hours following administration or until the effects of the drug, such as drowsiness, have subsided.
- Clients should be advised that if they get out of bed unassisted within 8 hours of receiving lorazepam, they risk falling and potentially sustaining injury.
- Alcoholic beverages should not be consumed for at least 24 to 48 hours after receiving lorazepam injectable due to the additive effects on central nervous system depression seen with benzodiazepines in general.
- Often prescribed for short term use, and if taking long term, do not abruptly stop taking the med.
- Elderly clients should be instructed that lorazepam injection may make them very sleepy for a period longer than 6 to 8 hours following surgery.
- Due to high risk of falls and injury, fall prevention strategies should be discussed.
Critical Thinking Out Loud
A 45-year-old client is being discharged home from the hospital following an appendectomy. They are usually independent and very active, with no health issues except insomnia. They tell the prescriber they would like a prescription to help them sleep at night. They are ordered: Lorazepam 0.5 – 1.0 mg oral before bedtime as needed. Other medications for discharge include an antibiotic and tramadol for pain control. The nurse reviews the order and considers this prescription for this client.
Lorazepam is an effective sedative, often used for insomnia. The dose that is ordered is low. The client is relatively young, has no mobility or cognitive concerns. He is on an analgesic that can also cause sedation and dizziness and these effects can be exacerbated with lorazepam. The nurse discusses with the client their insomnia and the use of other medications and interventions to promote sleep that have been tried in the past. They inform the client of the additive effect of taking both an analgesic and CNS depressant and the concern with being overly sedated and a risk for falls. The client understands that lorazepam should be used only if needed, right before bedtime and start with the lowest dose. They plan to try to not use lorazepam if they are also taking tramadol before bed. They understand the side effects and other considerations such as avoiding alcohol while taking lorazepam, not to drive after taking a dose, and if taking regularly, not to stop immediately.
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the “Answer Key” sections at the end of the book.
The Effects of Alcohol on GABA Receptors
Did you know that long term use of alcohol affects brain receptors, which undergo adaptive change in an attempt to maintain normal function. Alcohol enhances GABA activity acutely, with adaptive changes over time leading to decreased receptor sensitivity and decreased GABA levels. Therefore, a person needs more alcohol to get the same effect. GABA receptors become less responsive, leading to an imbalance of excitatory and inhibitory NTs. Alcohol also affects NMDA and dopamine receptors. For those with chronic alcohol consumption, if they stop drinking, leads to nervous system hyperactivity. Alcohol withdrawal protocols include benzodiazepines as part of the treatment to help reduce the neuron excitability.
Lorazepam Medication Card
Now let’s take a closer look at the medication card for lorazepam. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.

Downloadable file (.docx): Lorazepam Medication Card
Clinical Reasoning and Decision-Making Activity 5.4
- A client who has been experiencing panic attacks is prescribed lorazepam. Upon further discussion with the client, the nurse discovers that the client is planning to go on a cruise with her husband next week and plans to use a scopolamine patch to control nausea. The client states, “I can’t wait to relax on the cruise ship and have a margarita as we leave port!”
What important client education should the nurse provide to the client about the new prescription for lorazepam?
2. A client is brought in by ambulance to the ED and he are very drowsy and difficult to awaken. The client’s family say that he takes lorazepam for occasional anxiety and insomnia but lately he has been taking a higher amount to cope. This morning he was found unable to easily awaken. The family suspect he took too many lorazepam pills. Following an assessment, what medication will likely be given for this client? What will be interventions to support this clients suspected overdose?
3. A client is given phenobarbital for seizure activity in the hospital. What are important nursing interventions following administrering the med? Consider immediate actions and ongoing monitoring.
Note: Answers to the Critical Thinking activities can be found in the “Answer Key” sections at the end of the book.
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the “Answer Key” sections at the end of the book.
Benzodiazepine-like Drugs
Sometimes referred to as Z-Drugs or non-benzodiazepine drugs, this category of drugs are only used for treating insomnia. Examples are Zolpidem (trade name Ambien), Zaleplon (Sonata) and Eszopiclone (Lunesta).
They are all structurally different than benzodiazepines, and act as a GABA receptor agonist. They enhance the depressant effects of endogenous GABA. They do not have the anxiolytic or anticonvulsant effects that BZD have, and all have slightly different side effects and risk for tolerance. All are prescription medications and taken orally. Some comparisons between the meds:
Zolpidem: For short term use only, but long term use may cause tolerance and dependence. Respiratory depression may occur if used with other CNS depressants. Side effects include daytime drowsiness and dizziness.
Zaleplon: For short term use only for management of insomnia. Well tolerated with side effects including headache, nausea, drowsiness, myalgia and abdominal pain. It is less likely to cause anterograde amnesia (Bhandari & Sapra, 2023).
Eszopiclone: For short term use only (less than 4 weeks) for issues with sleep latency, sleep duration or nocturnal wakening. There is a risk of tolerance and dependence, leading to withdrawal and rebound insomnia if stopped suddenly. It is well-tolerated with minimal side effects which can include a bitter taste, headache, dizziness, and dry mouth. It can lead to psychological addiction. Adverse effect of sleep walking can occur.
(Drugs.com, 2026; Rosenjack Burchum & Rosenthal, 2019)
As with all CNS depressants, caution or avoidance for the older adult due to risk of falls and an exaggerated effect of CNS effects. They are contraindicated with severe hepatic disease, with dose reductions for those with mild-moderate hepatic disease.
To support your learning, you can access the Chapter 5 CNS Mood and Cogniton Medication Cards. This is a downloadable and editable document to allow you to update and add content.
Interactive Activities
References:
- Bhandari; P. & Sapra, A. (2023). Zaleplon. National Library of Medicine. Zaleplon – StatPearls – NCBI Bookshelf
- Bounds, C. & Patel, P. (2024). Benzodiazepines. National Library of Medicine. StatPearls [Internet].
- Canadian Geriatrics Society (2025). Twelve tests and treatments to question. Choosing Wisely Canada. Geriatrics Recommendations
- Drugs.com (2019, February 5). Barbiturates. https://www.drugs.com/drug-class/barbiturates.html ↵
- Drugs.com, 2026). Zopiclone. Zopiclone: Uses, Dosage, Side Effects, Warnings – Drugs.com
- DrugBank, 2026). Dihydroquinidine barbiturate: Uses, Interactions, Mechanism of Action | DrugBank
- López-Muñoz, F., Ucha-Udabe, R., Alamo, C. (2005).The history of barbiturates a century after their clinical introduction. Neuropsychiatric Disease and Treatment, Dec;1(4):329-43. PMID: 18568113; PMCID: PMC2424120.
- RNPedia. (2021). https://www.rnpedia.com
- Rosenjack Burchum, J., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
- Skibiski, J., Patel, P. & Abdijadid S. (2024). Barbiturates. National Library of Medicine. StatPearls [internet]. Barbiturates – StatPearls – NCBI Bookshelf
- Vallerand, A. & Sanoski, C. (2024). Davis’s Canadian drug guide for nurses (19th ed.). F.A. Davis Company: Canada
