7.10 Blood Coagulation Modifiers
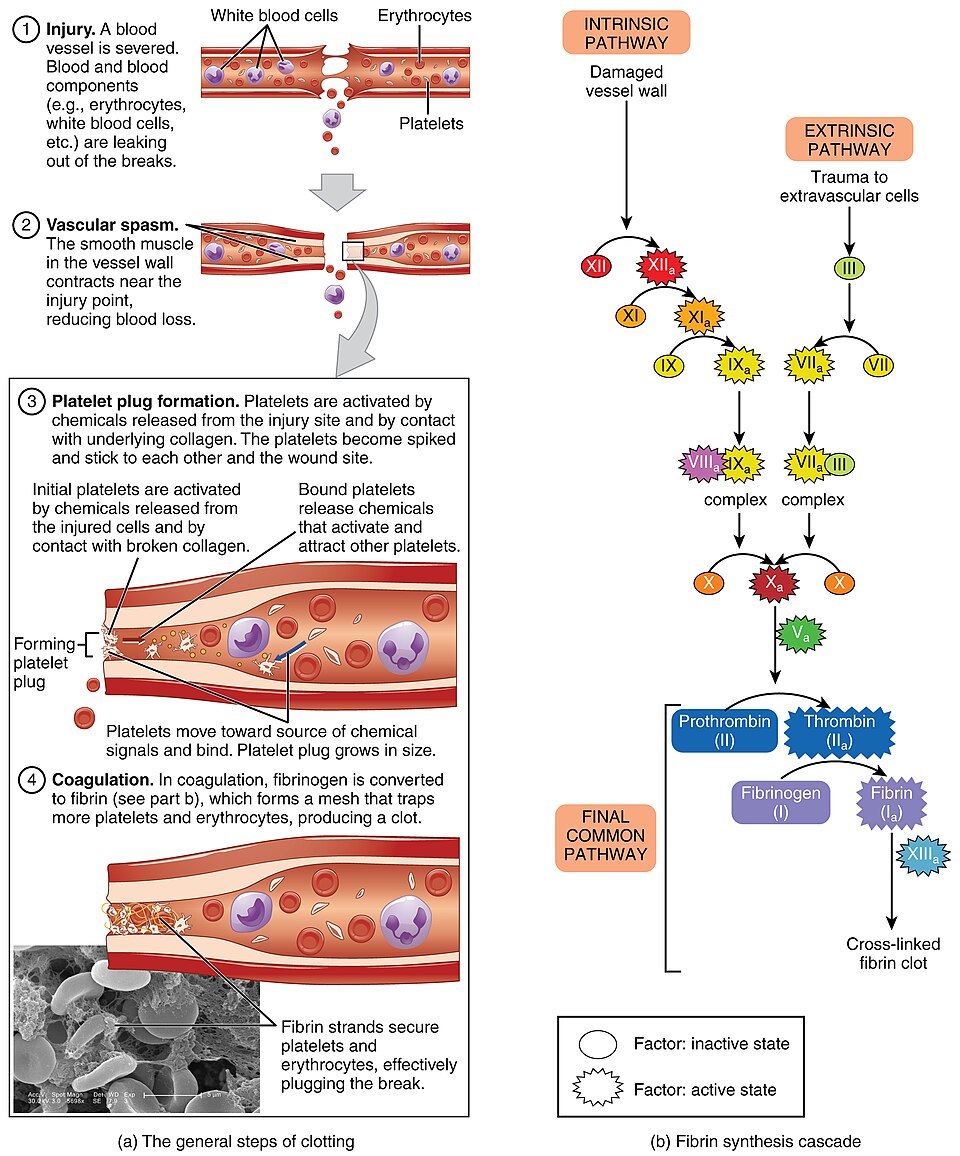
Coagulation normally serves a very healthy protective function by keeping us from excessive hemorrhaging. Hemostasis is a physiologic process by which bleeding is stopped following a blood vessel injury. It is a multistep process. The first is vascular spasm or constriction at the site of injury, followed by the formation of a platelet plug (primary hemostasis) and then, the reinforcement of the platelet plug by fibrin (coagulation phase). This seals the wound.
Watch the video to review the process of blood clotting.
Blood Clotting (Hemostasis) [4:37] by Dr. Matt and Dr. Mike (2020) on YouTube.
However, in conditions such as atrial fibrillation, deep vein thrombosis, pulmonary embolism, myocardial infarction and stroke (caused by emboli), where abnormal blood clotting has occurred, our clotting mechanisms can actually harm us. In these cases, pharmacological agents are used to alter the blood clotting mechanisms in order to preserve health and well-being.
Because blood clotting occurs via a few different pathways and processes, pharmacological agents are chosen depending on the severity of the condition and the desired anticoagulant effect. It is important to remember that there are varying levels of risk when anticoagulants are used. As such, nurses need to have knowledge to ensure safe administration and to educate clients on how to use these meds safely.
There are a number of drugs that modify coagulation. These include anticoagulants, antiplatelet drugs, thrombolytics (lyse thrombi), and antifibrinolytics.
- Antiplatelets: cyclooxygenase inhibitors (ASA, Clopidogrel/Ticagrelor), and glycoprotein IIb/IIIa inhibitor (tirofiban)
- These drugs inhibit platelet aggregation
- Used for arterial thrombus prevention
- Anticoagulants (Heparin, low molecular weight heparin, Warfarin, Rivaroxaban)
- These drugs disrupt the coagulation cascade and suppress the production of fibrin.
- Used for venous thrombus prevention
- Thrombolytics (Alteplase)
- Promote the lysis of fibrin, and lead to dissolution of the thrombi.
- Used to dissolve an ischemic stroke clot. Used only in critical care areas due to high risk and close monitoring required.
- Antifibrinolytic (tranexamic acid)
- Promote blood coagulation by stabilizing blood clots.
- Used for heavy menstrual bleeding. Taken orally, working within 24 hours.
- Note: desmopressin, an antidiuretic hormone medication, can also be used to control excessive bleeding, especially with hemophilia or von Willebrand’s disease.
Difference between arterial and venous thrombosis
Venous thrombosis develops at sites where blood flow is stagnant in a vein, usually deep veins. The stagnant blood initiates the clotting cascade, leading to fibrin production, and red blood cells and platelets adhering to form a thrombus (clot). Embolus are venous thrombi that have a long tail and can break off the become lodged elsewhere in the body such as the pulmonary circulation. Anticoagulants prevent thrombosis in veins.
Arterial thrombosis begins with the adhesion of platelets to the arterial wall, following damage to the wall or a rupture of plaque. Platelets aggregate and can occlude the artery. This is localized and can lead to decreased perfusion to the area. Antiplatelet drugs prevent thrombosis in arteries.
In this unit, we will focus on only three categories that affect coagulation:
- Antiplatelets: cyclooxygenase inhibitors (ASA, Clopidogrel/Ticagrelor)
- Anticoagulants (Heparin, low molecular weight heparin, Warfarin, Rivaroxaban, Dabigatran)
- Thrombolytics (Alteplase)
Antiplatelets
Antiplatelet therapy (APT) is the foundation of treatment and prevention of atherothrombotic events in patients with atherosclerotic cardiovascular disease (Canadian Journal of Cardiology, 2023). Although aspirin was the first antiplatelet medication, today there are a number of both oral and parenteral medications. Oral APT include aspirin, clopidogrel, ticagrelor, and dipyridamole. Parenteral meds are glycoprotein IIb/IIIa inhibitors such as tirofiban and eptifibatide, which are used in the acute phases of acute coronary syndrome (Iqba, Lopez & Hai, 2022).
Acetylsalicylic acid (aspirin) and clopidogrel (Plavix) will be the prototype medications.
To help understand the difference between the meds, we will look at the mechanism of action of ASA, Clopidogrel and Glycoprotein platelet inhibitors.
Mechanism of Action
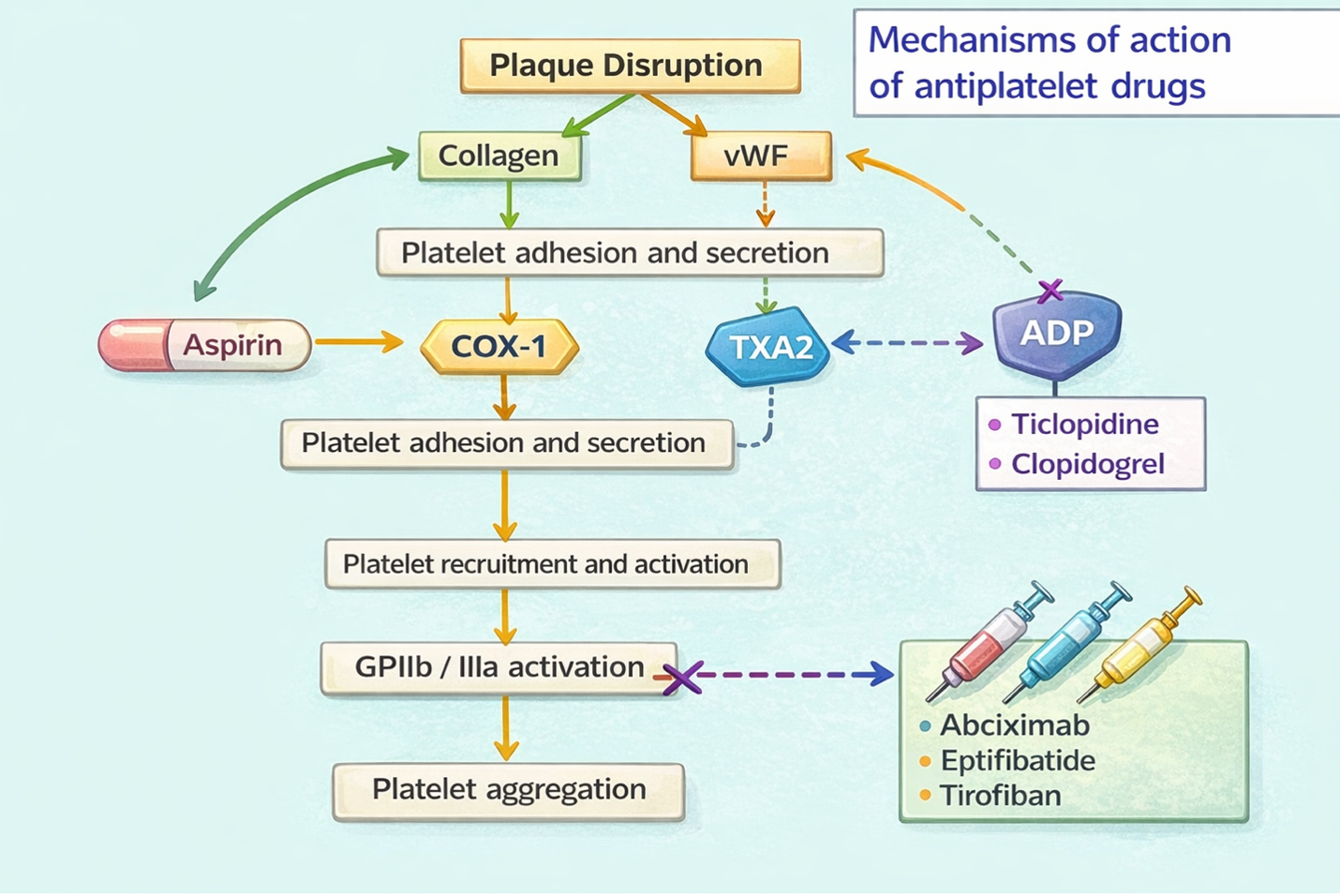
Antiplatelet drugs suppress platelet aggregation and prevent thrombosis in arteries. Antiplatelet drugs can be divided into categories based on their mechanism of action.
- Platelet aggregation inhibitors:
- Cyclooxygenase inhibitor: Acetylsalicylic acid (ASA)
- P2Y12 adenosine diphosphate (ADP) receptor blockers: Clopidogrel, ticagrelor.
- Glycoprotein platelet inhibitors: tirofiban
- Other APT meds that are not covered in this unit are protease-activated receptor-1 antagonists (vorapaxar) and nucleoside transport inhibitor and PDE3 inhibitor (cilostazol).
Acetylsalicylic acid (ASA)
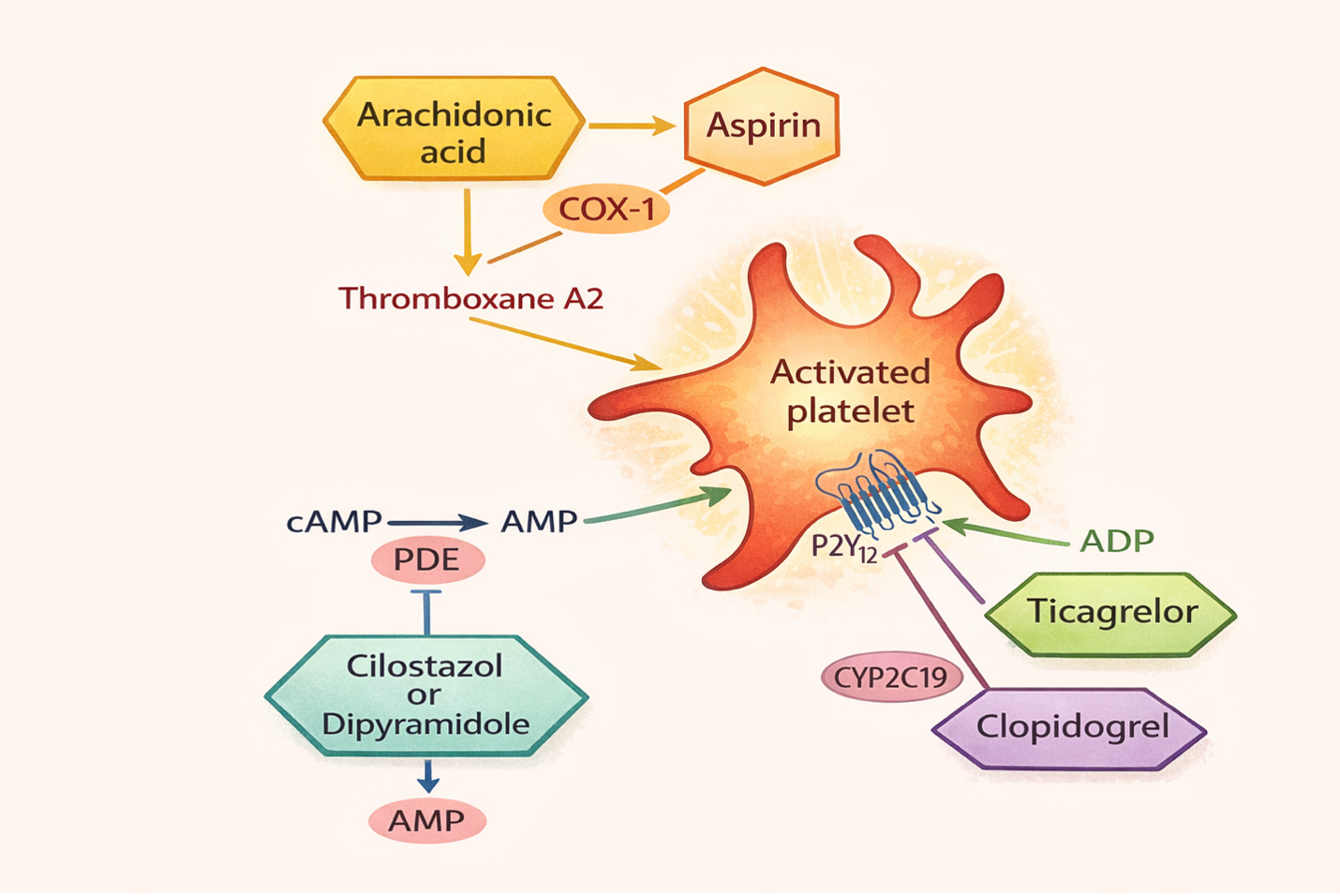
ASA irreversibly inhibits the cyclooxygenase enzyme (COX) activity in the prostaglandin synthesis pathway (PGH2). This contrasts with NSAIDs which reversibly binds to COX. Cyclooxygenase is needed for platelets to synthesize thromboxane A2 (TXA2) which is one of the factors to promote platelet aggregation and vasoconstriction on vascular smooth muscle. By inhibiting TXA2 mediated vasocontraction and platelet aggregation, the risk of arterial thrombosis is reduced. Low dose aspirin of 81 mg/day can result in near complete inhibition of COX-1. Low doses are often used, as higher doses can also inhibit COX-2 and lead to a higher risk of GI bleeding (Iqba, Lopez & Hai, 2022).
The irreversible inhibition is what sets ASA apart from other NSAIDs. Although it takes one hour post ingestion to block platelets, due to irreversible inhibition of COX, it is inhibited for the life of the platelet which is about eight days. This provides the sustained effect of inhibiting platelet aggregation after one dose. Other NSAIDs do not have this sustained effect and are not used for cardiac prevention.
P2Y12 Adenosine Diphosphate (ADP) Receptor Blockers: Clopidogrel
P2Y12 ADP receptor blockers work on platelet surface, irreversibly inhibiting the platelet P2Y12 receptor thereby preventing platelet aggregation. Clopidogrel causes irreversible receptor blockage while ticagrelor causes reversible blockage. Both have similar efficacy. Since P2Y12 inhibition with ticagrelor is reversible, the antiplatelet effect dissipates more rapidly than with clopidogrel, which are irreversible P2Y12 inhibitors. Therefore, there is less procedure-related bleeding and less time to withhold the drug prior to procedures (Wallentin et al, 2009).
Glycoprotein platelet inhibitors
Glycoprotein platelet inhibitors work by irreversibly inhibiting glycoprotein IIb/IIIa (GpIIb-IIIa) receptors on platelets, thus decreasing platelet aggregation. Their action is on the final step of platelet aggregation which limits all the platelet aggregation factors. They are the most effective antiplatelet drugs and are used short term to prevent ischemic events in ACS (Rosenjack Burchum & Rosenthal, 2019).
Indications for Use
Anti-platelet therapy are used for a wide variety of cardiovascular conditions. It is used for the prevention of acute coronary syndrome, for the maintenance of coronary artery stents, and peripheral artery disease.
Acetylsalicylic Acid
Acetylsalicylic Acid (aspirin) is a non-opioid analgesic and anti-pyretic. It is also used for its cardioprotective anti-platelet effects. In this unit, we will focus only on the cardioprotective effects. ASA is also in unit 6.5 with a focus on the analgesic and antipyretic effects.
Cardioprotective Effects of ASA: One of the beneficial effects of ASA is the thrombotic effects and is routinely recommended for clients at greater risk of myocardial infarction (MI) or stroke. This includes clients with ischemic stroke, transient ischemic attacks, acute MI (both ST elevation and non-ST segment elevation) and previous MI. It is also prescribed for higher risk clients as a primary prevention of MI (Rosenjack Burcham & Rosenthal, 2019). For anti-platelet effects, the dose of 81 mg once a day is sufficient, as higher doses will increase the risk of GI bleeding without more cardio protective effects.
Clopidogrel
Clopidogrel is used to prevent stenosis of coronary stents or secondary prevention following an MI or ischemic stroke.

Tirofiban
Tirofiban, the GP IIb/IIIa antagonist, is used short term to prevent ischemic events in clients with ACS or undergoing percutaneous coronary insertion. It is given intravenously.
Nursing Considerations for Anti-Platelet Medications
Administration:
- ASA can be given oral or rectal. It comes in tablet, liquid and enteric coated options. Different dosages are prescribed depending on the rationale for use:
- 81 mg po once a day – for cardioprotective effects. A larger dose is not needed to inhibit platelet aggregation.
- 325 mg po for acute cardiac events, such as suspected MI, to achieve effects quickly.
- 325-650 mg po q 4-6 hour (2600 mg/day) for pain and fever.
- 3000-4000mg per day for inflammatory conditions such as rheumatoid arthritis
- Clopidogrel, taken orally, and it is well tolerated. It is given with ASA in clients with ACS. It reaches steady state in 5-7 days.
- GPII-IIIa inhibitors are given intravenously and used for short term therapy during acute coronary syndrome.
ASA is rapidly absorbed in the small intestine after oral administration. ASA has a short life, converted to salicylic acid within 15-20 minutes. It is highly bound to albumin, and rapidly distributed to all body tissues. It is renally excreted (Rosenjack Burchum & Rosenthal, 2019).
Prior to surgery: ASA causes irreversible inhibition of platelet aggregation. This effect lasts the life time of a platelet which is 7-10 days. ASA is often withheld for several days prior to surgery or certain procedures to prevent excessive bleeding.
Children: ASA is contraindicated in children under the age of 14 due to the risk of Reye’s syndrome. Reye’s Syndrome can occur in children who have a viral or upper respiratory tract infection and are then given ASA to treat the fever. Children develop encephalopathy and liver damage secondary to mitochondrial injury. There is a high fatality rate of 30-45%. Children under 14 years should not be given ASA. If a child needs analgesic or pain relief, then acetaminophen or ibuprofen can be used safely.
Pregnancy and Breastfeeding:
ASA is not considered safe for pregnant women, especially after 20 weeks of pregnancy. It crosses the placenta, and can potentially cause low birth weight, still birth, and renal issues on the fetus. For the mother, it can suppress contractions, so need to avoid in the third trimester. It can also be found in breast milk and not recommended.
Older Adult:
Older adults are more susceptible to negative GI and CNS effects of anti-inflammatories. If the client has renal insufficiency, then ASA will not be readily excreted, prolonging the duration of action. There is also an increased risk of bleeding with concurrent use of Clopidogrel plus ASA.
Contraindications to using antiplatelet medications include large esophageal varices, recent stroke within 2 years, ESRD, severe hypertension with BP over 200/110.
Clients with an allergy to Ibuprofen should not take ASA due to cross sensitivity.
Increased risk of GI bleeding with clients with peptic ulcer disease or gastritis, clients on warfarin, or any bleeding disorders.
Drug Interactions for Clopidogrel
Clopidogrel is metabolized to its active metabolite by CYP2C19. Concomitant use of drugs that inhibit the activity of this enzyme results in reduced plasma concentrations of the active metabolite of Clopidogrel and a reduction in platelet inhibition. Drugs interactions can occur if used with proton pump inhibitors, opioids, NSAIDs, warfarin, and antidepressants (Iqba, Lopez, & Hai, 2022).
Adverse/Side Effects
ASA is typically well tolerated but may cause toxicity, intolerance or hypersensitivity.
The most common side effect is gastric irritation. This can range from mild gastritis to gastrointestinal bleeding. To avoid this effect, clients are recommended to take enteric coated ASA (Arif & Aggarwal, 2023).
Other side effects include heartburn and nausea. Bruising easily and bleeding gums are also common.
Adverse Effects:
Bleeding: GI bleeding is relatively common and the client may experience dark, tarry stools. Typically, the amount of bleeding is very minimal, but if on ASA for a long period of time, even at low doses, it may produce anemia. Also, there is a higher risk of gastric ulceration, perforation and bleeding. The chance for bleeding is higher if a client:
- takes a higher dose or takes it for a longer time than directed
- takes other drugs containing prescription or nonprescription NSAIDs (aspirin, ibuprofen, naproxen, or others)
- has had stomach ulcers or bleeding problems
- takes a blood-thinning (anticoagulant) or steroid drug
- is age 60 or older
- smokes cigarettes
- has 3 or more alcoholic drinks every day while using this product
To minimize the risk of gastric ulcers, clients can take a proton pump inhibitor to reduce the hydrochloric acid in the stomach. Other meds such as histamine receptor antagonists or misoprostol are beneficial.
Hypersensitivity reactions
Hypersensitivity reactions are less common but are more likely with clients with a history of asthma, rhinitis and nasal polyps (Rosenjack Burchum & Rosenthal, 2019). This NSAID-induced respiratory disease begins within one hour of ingestion. Symptoms begin with diffuse watery rhinorrhea and can eventually lead to urticaria, bronchospasm and shock. This is not the same as an allergic reaction but due to the inhibition of COX-1 which triggers the production of leukotrienes. Clients who are allergic to any NSAID should not take aspirin as there is cross-reactivity.
Salicylate Toxicity
If ASA levels climb above therapeutic levels, salicylism can occur. Cues can include tinnitus (ringing in the ears), sweating, headache, nausea and dizziness. If a mild case, then withhold ASA, and once symptoms reside, then ASA can resume but with smaller doses.
If severe, the client can experience hyperthermia, tachypnea, metabolic acidosis, hypokalemia, seizures and cerebral edema. If these cases, salicylate toxicity is treated based on salicylate concentration, acid-base and electrolyte status. Treatment is activated charcoal, treating acidosis, and supportive measures (Arrif & Aggarwal, 2023).
Contraindications
ASA is contraindicated if the client has a bleeding disorder such as hemophilia, vitamin K deficiency, or a recent history of bleeding in the stomach or intestine. High doses of ASA should be held prior to surgery for one week. It does not need to be held for minor procedures such as dental procedures (Rosenjack Burchum & Rosenthal, 2019).
Renal Impairment
Extra caution should be advised for clients at higher risk of impaired renal function from ASA use. ASA can cause irreversible renal impairment resulting in salt and water retention and edema. Clients most at risk are advanced age, history of renal insufficiency or liver impairment or heart failure.
Client Teaching
Clients should be made aware of the potential risks to avoid gastric distress, GI bleeding and other adverse effects.
- Take with a full glass of water and remain upright for 30 minutes
- Use only the recommended dosage depending on the reason for use.
- Monitor for side effects such as nausea, gastric irritation, and occasional blood in stools. Report persistent symptoms such as ongoing bleeding or fever longer than 3 days.
- Monitor for adverse effects such as tinnitus and hold ASA until seen by their prescriber.
- If the client has asthma or rhinitis, be aware of hypersensitivity reaction cues such as diffuse watery rhinorrhea, itching and bronchospasm.
- Do not give ASA to children.
- If going for surgery, discuss with health care provider for the need to hold ASA one week prior to surgery.
- Avoid consuming alcohol greater than 3 drinks a day while on ASA
- Do not take ASA while pregnant. If taking ASA for inflammatory conditions, and under the supervision on their prescriber, ASA may be taken up to the third trimester.
(Vallerand & Sanoski, 2024).
Acetylsalicylic Acid Medication Card
Now let’s take a closer look at the medication card for antiplatelet meds. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.
Downloadable file (.docx): Acetylsalicylic Acid Medication Card
Anticoagulants
Recall that anticoagulants are used to prevent venous clot formation. Clients who are more at risk for clots such as deep vein thrombosis (DVT) are those with blood flow stasis (advanced age, obesity, atrial fibrillation, bedrest), endothelial damage (major surgery or trauma) and hypercoagulable states (increased estrogen from pregnancy or oral contraceptive use) (Kushner et al, 2024).
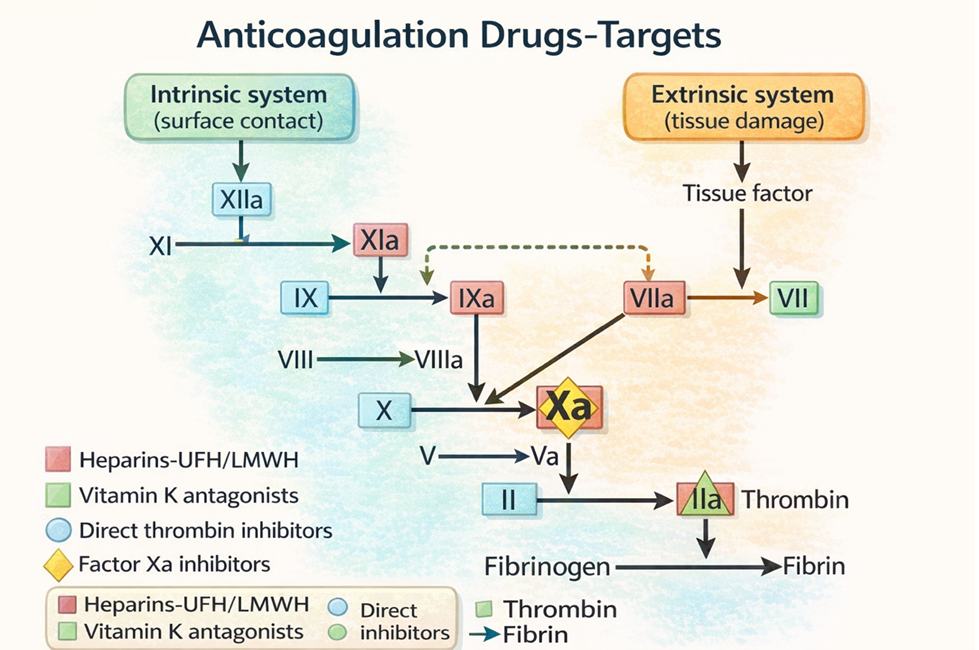
Anticoagulants prevent the formation of a clot by greatly enhancing the activity of antithrombin, which inactivates thrombin and factor Xa, which results in reducing the formation of fibrin and the ability of the blood to clot. They are used to:
- Prevent the formation of thrombi with high-risk clients
- Prevent and treat thromboembolic events (DVT, PE)
- Prevent excess coagulation from surgery or dialysis
Anticoagulants include the following drug classes:
- heparins or unfractionated heparin and low molecular weight heparin (LMWH),
- warfarin (Coumadin),
- selective factor Xa inhibitors (Rivaroxaban), and
- direct thrombin inhibitors (dabigatran).
In this unit, we will review heparins, warfarin and selective factor Xa inhibitors.
Diagnosis for venous clot formation:
For all clients who are high risk for a DVT or pulmonary embolus (PE), nurses must assess for:
- DVT: unilateral calf pain, swelling and warmth in the calf.
- Pulmonary embolus: SOB, chest pain, fatigue, tachycardia, hypoxia
Note: clients will not present with all these symptoms or they will be very subtle. Pay attention to subtle cues and report any unusual finding.
For any client suspected of a clot, PE or DVT diagnostics may include:
- Positive D-dimer (elevated levels indicate a clot somewhere in the body, not very specific so not used for definitive diagnosis)
- Chest XR to rule out other causes
- Duplex ultrasound if DVT suspected
- CT scan chest
- VQ scan
Medication Safety with Blood Coagulation
Anticoagulants are a high alert med due to the risk of bleeding. Heparin and warfarin are both on the top 10 list of drugs most frequently reported causing harm due to a drug error (Institute for Safe Medication Practices in Canada (ISMP), 2020). In hospital settings, errors are related to administration issues including incorrect dosage calculations and infusion rates (Anderson & Townsend, 2015). ISMP (2006) found that the underuse of anticoagulants in high-risk clients that resulted in venous thromboembolism is one of the most serious complications. In the community, anticoagulants can be used incorrectly by clients and carry the risk of serious bleeding. To reduce harm, the Health Research and Educational Trust recommend that facilities:
- Educate staff based on evidence and best practices.
- Use standardized order sets and protocols. For example, standardized order sets for heparin and warfarin.
- Perform medication reconciliation at all transitions.
(Anderson & Townsend, 2015).
Heparin Sodium
Heparin sodium is an anticoagulant that is commonly used in the hospital setting to either prevent or treat thrombosis. Heparin unfractionated (IV infusion) is given in high doses to treat a DVT or PE. In lower doses, it is given SQ to prevent post-op thrombosis.
Heparin is a high alert medication due to the different concentrations and high risk of bleeding. To avoid risk, hospitals use several processes for storing and labelling to help prevent errors. As nurses, we must ensure safety by following the appropriate steps when choosing which vial to draw up the medication and follow hospital protocols during administration such as independent double checks.
We will review unfractionated heparin and also Low Molecular Weight heparin (enoxaparin)

Safety alert for heparin
Heparin comes in many different concentrations, depending on the rationale for prescribing heparin.
Dosages include: 1000 units/mL, 5000 units/mL, 10,000 units/mL
Take precautions to avoid a med error by following safe med practices.
Mechanism of Action
Unfractionated Heparin
Unfractionated heparin potentiates the inhibitory effect of antithrombin on factor Xa and thrombin. In the absence of both of these clotting factors, the production of fibrin is reduced and clotting is suppressed (Rosenjack Burchum & Rosenthal, 2019). Recall that fibrin forms the framework for thrombi in veins.
Heparin does not have fibrinolytic activity; therefore, it will not break down existing clots, only prevent venous thrombosis.
Heparin is highly polar, and as such does not readily cross membranes especially the GI tract, so it is only given parenterally. Heparin works quickly, within minutes by IV route. It has a peak effect of 5-10 minutes. It has a short half-life of 1-2 hours, which is longer in clients with renal or hepatic insufficiency, obesity or infections (Vallerand & Sanoski, 2024). For SQ route, the is 20-60 minutes.
Low Molecular Weight Heparin (dalteparin, enoxaparin)
Low Molecular Weight Heparin (LMWH) also potentiates the inhibitory effect of antithrombin. But their molecular chains are shorter than with unfractionated heparin, so they preferentially inactivate factor Xa and less able to inactivate thrombin. Heparin has a faster onset of anticoagulant action as it will inhibit Xa and thrombin, while LMWH acts only through Xa inhibition.
LMWH are equally effective at venous thrombi prevention. It has a higher bioavailability and a prolonged half-life than unfractionated heparin, resulting in more predictability. As such, they are given in a fixed dose, once a day and do not require PTT monitoring (Patel & Varacallo, 2025).
Indications for Use
Unfractionated Heparin
Depending on the purpose, the dose and concentration of heparin are different. It is only given IV or SQ, as the heparin molecule is too large to cross membranes in the GI tract.
- IV heparin (continuous infusion) is commonly indicated for the treatment of deep venous thromboembolism (DVT) or pulmonary embolism. It is also indicated for use during acute myocardial infarction.
- Subcutaneous heparin is commonly indicated to prevent DVT or embolization caused by atrial fibrillation.
- Heparin IV flushes (“Hep-Locks”) are used to maintain the patency of central IV lines. These concentrations are very low, with between 10-100 units/mL.
Low Molecular Weight Heparin (dalteparin, enoxaparin)
Used for:
- prophylaxis of venous thromboembolic disease (VTE) on acute or elective admission to the hospital,
- treatment of deep vein thromboses (DVT) and pulmonary embolism (PE).
- DVT treatment in pregnant women.
Unlike heparin, they can also be used by clients at home. For example, high risk post-op clients that need short term anticoagulation.
Nursing Considerations
Administration:
Unfractionated heparin IV for DVT and PE treatment:
- Continuous IV infusion in peripheral or central line. IV bags are pre-mixed in pharmacy with 25,000 units heparin /D5W 500 mL for a concentration of 50 units/mL.
- Heparin Nomogram is used that includes lab work, initial heparin therapy and continuous therapy. Initial dosing is based on client weight.
- It requires close monitoring of frequent partial thromboplastin time (PTT) results to ensure dosage is in therapeutic range and to reduce the risk of overdose with associated bleeding. Dosage is considered adequate when the activated partial thromboplastin time (APTT) is 1.5 to 2 times the normal or when the whole blood clotting time is elevated approximately 2.5 to 3 times the control value. Follow institutional therapeutic monitoring for current practice guidelines and client context.
- Labs: baseline PTT, CBC and INR before therapy, then PTT every 6 hours until within therapeutic range. Monitor platelet count q 2-3 days.
Unfractionated heparin SQ for DVT prophylaxis:
- SQ syringes with 10,000 units/mL for dose of 5000 units SQ.
- BID dosing. Risk of bruising at site.
- No PTT monitoring
Heparin molecules are too large to cross membranes so only given IV or SQ. It is also too large to cross the placental barrier, so there is no risk to the fetus. It is also too large to be excreted in breastmilk.
LMWH: enoxaparin is administered SQ, usually once a day. Often prescribed for 7-10 days post-op for clients recovering from hip or knee surgeries or abdominal surgeries.
Hepatic and renal impairment: heparin is metabolized by the liver and excreted by the kidney. The half-life is two hours so if renal or hepatic impairment, duration of action will be longer.
Do not give IV heparin with antiplatelet medications.
Older adult: A higher incidence of bleeding has been reported in clients over 60 years of age, especially women.
Reversal agent: protamine sulfate. If bleeding requires quick reversal of anticoagulation, protamine is given by slow infusion to neutralize heparin sodium and reverse the heparin action. Protamine forms a bond with the heparin molecule and neutralizes it immediately. Administer 20 mg/min. Protamine 1 mg will neutralize 100 units of heparin. It lasts about 2 hours and then dose may need to be repeated.
Contraindicated in clients with a history of Heparin-Induced Thrombocytopenia (HIT) and Heparin-Induced Thrombocytopenia and Thrombosis (HITT). HIT is a condition where platelets drop 30% or more below a client’s baseline after heparin is administered and can lead to HITT where thrombi are formed.
Use with caution with medications that affect the coagulation cascade due to additive effects that increase the risk of bleeding. When a client is receiving IV heparin therapy to treat a blood clot, it may be overlapped with oral warfarin to establish anticoagulation therapy after discharge. See more information about this process under the “Warfarin” section.
Adverse/Side Effects
High Alert Med: Fatal hemorrhages have occurred due to medication errors. Carefully examine all heparin products to confirm the correct dose prior to the administration of the drug. Independent double check for infusions. Notify prescribing provider immediately of new signs of bleeding or bruising, or sudden changes in vital signs that indicate internal bleeding, such as decreasing blood pressure with an associated increase in heart rate.
Heparin-Induced Thrombocytopenia (HIT): Some clients may develop Heparin-Induced Thrombocytopenia (HIT) or Heparin-Induced Thrombocytopenia and Thrombosis (HITT). It is a potentially fatal immune-mediated disorder that is characterized by extremely low platelet count and an increase in thrombotic events despite adequate anticoagulation. Monitor platelet count. If this develops, heparin should be discontinued immediately.
Cues of internal bleeding
The risk of internal hemorrhage is 10%. Assess for symptoms such as hypotension, tachycardia, petechiae, red or black stools, hematuria, pelvic pain and headache. Notify the MD immediately if hemorrhage is suspected. Protamine sulfate IV is the reversal agent.

Client Teaching
- Clients should notify health care staff immediately of new signs of bleeding or bruising,
- and remind physicians and dentists that they are receiving heparin before any surgery or invasive procedure is scheduled.
- Clients should avoid medications containing aspirin or NSAIDS.
- Clients should avoid IM injections, and use a soft toothbrush and electric razor, as precautions against causing bleeding (Vallerand & Sanoski, 2024).
Low Molecular Weight Heparin (LMWH)
Enoxaparin is a low molecular weight heparin (LMWH) is often prescribed instead of heparin for DVT prevention. It is very effective but with the additional benefit of not requiring aPTT monitoring.

Mechanism of Action
Enoxaparin is a low molecular weight heparin, which has antithrombotic properties with a higher ratio of anti-Factor Xa to anti-Factor IIa activity compared to heparin. It is metabolized slowly from the liver. It has a longer bioavailability and is more predictable than heparin. For this reason there is a fixed dose and no need for monitoring coagulation.
Indications for Use
It is indicated for the prevention and treatment of deep vein thrombosis (DVT), which may lead to pulmonary embolism (PE). It is also used in combination with aspirin for the treatment of acute myocardial infarction or a STEMI. It is often prescribed post op for clients who are high risk of a DVT such as orthopedic surgeries.
Nursing Considerations
Administration: SQ and preferably in the abdomen for best absorption. Given once a day or BID. It is supplied in a prefilled syringe.
Safety and effectiveness have not been established in pediatric clients.
Older adult: The risk of bleeding increases with age, especially if used concurrently with antiplatelet medications.
Renal Impairment: Use with caution in clients with renal impairment; risk of bleeding is increased. A dosage adjustment is recommended for clients with severe renal impairment.
Overdoses can be neutralized with a slow IV infusion of protamine sulfate. Not as effective as with heparin.
Adverse/Side Effects
Less bleeding risk but still monitor for bleeding. Higher risk following percutaneous coronary revascularization procedures or with concurrent medication conditions such as recent GI ulcer. It may cause Heparin-Induced Thrombocytopenia (HIT) or Heparin-Induced Thrombocytopenia with Thrombosis (HITT).
High Alert Med: Epidural or spinal hematomas may occur in clients who are anticoagulated with low molecular weight heparins (LMWH) and are receiving neuraxial anesthesia or undergoing spinal puncture. These hematomas may result in long-term or permanent paralysis.
Client Teaching
- Notify health care staff immediately of new signs of bleeding or bruising.
- Remind physicians and dentists that they are receiving heparin before any surgery or invasive procedure is scheduled.
- Clients should avoid medications containing aspirin or NSAIDS (Vallerand & Sanoski, 2024).
Warfarin
Since 1954, warfarin has been a standard but hazardous treatment for preventing blood clots. It is a vitamin K antagonist. Warfarin requires close laboratory monitoring and individual dose adjustments based on PT and INR lab results. When the pharmaceutical industry began marketing modern replacements for warfarin, including dabigatran, rivaroxaban, and apixaban, they designed them to be easier to use than warfarin because no laboratory monitoring was required, but they were not necessarily safer. It is vital for nurses to provide thorough client and caregiver education for clients prescribed anticoagulants at home. Suggested client education topics are included for each type of medication below.
Mechanism of Action
Warfarin inhibits an enzyme that is required for the action of vitamin K. Without vitamin K, the production of clotting factors II, VII, IX and X as well as coagulation regulator proteins C and S, is diminished. These clotting factors circulate in the blood so it takes a few days for plasma levels to fall. Warfarin is also highly bound to protein, so the actual available amount of warfarin is unavailable to produce its effect. This explains why there is a delay in achieving therapeutic effect (Patel et al, 2024).
Indications for Use
Warfarin is typically given for long term prophylaxis against thrombosis. It is indicated for:
- Prophylaxis and treatment of venous thrombosis and its extension, pulmonary embolism (PE).
- Prophylaxis and treatment of thromboembolic complications associated with atrial fibrillation (AF) and/or cardiac valve replacement.
- Reduction in the risk of death, recurrent myocardial infarction (MI), and thromboembolic events such as stroke or systemic embolization after myocardial infarction.
Pharmacokinetics
Warfarin is easily absorbed following oral administration. It can take up to 72 hours to take effect, with the duration of action between 2 and 5 days. It is highly protein bound at 99%. Free or unbound warfarin readily crosses cell membranes. It crosses the placental barrier. It is metabolized in the liver and excreted by the kidney and feces (Patel et al, 2024).
Nursing Considerations
Administration: oral, formulated in various strengths in different colors to help prevent errors when clients self-administer different dosages at home (See figure 7.10h) Close International normalized ratio (INR) monitoring is required.
Monitoring:
- Baseline INR prior to therapy.
- Warfarin initiated at 5 mg/day but may be lower in at-risk clients (see below).
- INR every 2-4 days, then weekly, and once stable q 2 weeks, then eventually q 4 weeks. The objective is for the INR to be raised to an appropriate level.
Normal INR 0.8-1.2
Target 2-3 (target for mechanical valve 3-4.5)
(Ministry of Health, 2023).
At the initiation of therapy:
- INR will rise without concomitant therapeutic anticoagulant effect during the first 5-7 days of treatment. During the maintenance phase, a dose change may not be reflected in INR for 4-5 days and so dose changes more than twice a week are not recommended.
- As therapeutic effect will not occur for the first 5 days, LMWH or unfractionated heparin SQ may be prescribed during that time.
Dosages: typical starting dose is 5 mg/day. Lower doses of 1-2 mg/day may be ordered for clients who are frail, over 70 years of age, hypoalbuminemia (i.e. malnourished, liver disorders, post- operative), heart failure, recent use of some antibiotics that would impact gut flora.
In hospitalized clients receiving heparin therapy, there is often a period of overlap where the client is prescribed both IV heparin and warfarin until the INR reaches therapeutic range. At that point, the IV heparin is discontinued.
Cultural differences: clients of Asian descent tend to require lower doses. Clients of African American descent tend to need higher doses because of the differences in genetic polymorphisms between these populations.
Contraindications:
Absolute contraindications include liver disease with baseline INR greater than 1.3, non-adherence to taking the med or with accessing INT testing, or hemorrhagic tendencies or blood dyscrasias. Also, recent surgery of the central nervous system or eye, or traumatic surgery resulting in large open surfaces.
Bleeding tendencies include conditions such as active ulceration in the GI tract, overt bleeding in the GU or respiratory systems, cerebral aneurysms, dissecting aorta, pericarditis, or bacterial endocarditis.
Pregnancy: contraindicated during pregnancy due to risk to fetus such as teratogenicity and spontaneous abortion. LMWH is safe to use. Women with mechanical valves who may need warfarin, then avoid first trimester and within 2-4 weeks of delivery.
Dietary restrictions:
Although there are no absolute dietary restrictions for patients taking warfarin, they do need to maintain a consistent and regular diet. Their vitamin K intake should be consistent amount each day or it can influence INR levels. Vitamin K rich foods include leafy greens, cabbage, fish, liver, tomatoes. Avoidance of certain herbs such as garlic, ginger, gingko bilboa, and St John’s Wort, may be recommended.
(Ministry of Health, 2023; Patel et al, 2024).
Drug Interactions
Warfarin has significant interactions with many medications; either they interact to reduce the coagulant effects (sub therapeutic) or the coagulation can be increased to the point of hemorrhage. For example, there is a higher risk of bleeding (higher INR) with many medications including anticonvulsants (phenytoin sodium), analgesics (acetaminophen, aspirin, tramadol). antibiotics (amoxicillin, macrolides, tetracycline and many others), antidepressants (SSRIs, citalopram) and anti-arrythmics (amiodarone, propafenone).
INR levels are decreased with St John’s Wort, antibiotic (rifampin), antithyroid agents, trazadone and smoking. Read drug label information before administering. Consult with the prescriber or the pharmacist.
BC Guidelines.ca (2015)
Reversal Agent: Vitamin K1
Vitamin K antagonizes warfarin’s actions and can reverse the inhibition of clotting factor synthesis. It is used if INR is greater than 5.
Dosage: oral or IV. For IV, dilute and infuse slowly to avoid flushing, chest pain, dyspnea and hypotension.
i.e. 2.5 mg po or 0.5- 1.0 mg IV. Only give enough vitamin K to get INR back into range. If severe bleeding, can give fresh frozen plasma or whole blood. If too much vitamin K is given, it is difficult to anticoagulate afterwards.
(Ministry of Health, 2023; Patel et al, 2024)

Adverse/Side Effects
High Alert Med: Warfarin can cause major or fatal bleeding. Perform regular monitoring of INR in all treated clients. Drugs, dietary changes, and other factors affect INR levels achieved with warfarin therapy. Instruct clients about prevention measures to minimize risk of bleeding and to report signs and symptoms of bleeding. Warfarin can cause acute kidney injury and bleeding risks are increased in clients with liver disease.
Signs of bleeding can include: hypotension, tachycardia, bruises, petechiae, hematomas, red or black stools, pelvic pain, headache.
Client Teaching
Clients or their caregivers must be able to adhere to the treatment plan. Ensure they understand the treatment goals and need for strict monitoring and strategies to avoid risk. Advise clients to:
- Avoid alcohol, cranberries, and grapefruit as they increase the effect of warfarin and the risk of bleeding.
- Strictly adhere to the prescribed dosage schedule.
- Follow INR monitoring guidelines as provided by the prescriber.
- Avoid any activity or sport that may result in traumatic injury and risk of bleeding.
- Tell their provider if they experience frequent falls, since warfarin can increase their risk for bleeding in the brain.
- Eat a normal, balanced diet, including green, leafy vegetables, to maintain a consistent intake of vitamin K.
- Tell all health care professionals and dentists that they are taking warfarin, especially before surgery or dental procedures.
- Use electric razors instead of straight razors.
- Carry identification stating that they are taking warfarin.
- Do not take any medications, herbal supplements or OTC meds without consulting with their prescriber.
- Notify their provider immediately if any unusual bleeding or symptoms occur, such as pain, swelling or discomfort, prolonged bleeding from cuts, increased menstrual flow or vaginal bleeding, nosebleeds, bleeding of gums from brushing, unusual bleeding or bruising, red or dark brown urine, red or tar black stools, headache, dizziness, or weakness (DailyMed, 2025).
Example in practice:
A 72-year-old client, Jas, has experienced a syncopal episode and was brought to ED. He is diagnosed with atrial fibrillation. Following the initial treatment to lower his heart rate and improve his cardiac output, he is now stable. He is ordered the beta blocker bisoprolol to maintain his heart rate. Jas is also ordered warfarin for long term prevention of a stroke. The nurse checks his recent blood work. The INR is 2.2. Jas weighs 62 kg. The nurse checks the Warfarin nomogram in the physician’s orders. Based on the client’s latest INR and his weight, the nurse will give him warfarin 5 mg po. Jas will be taking 5 mg each morning for the next two days, at which time his INR will be rechecked and the dose adjusted to keep his INR between 2-3.
Warfarin Medication Card
Now let’s take a closer look at the medication card for warfarin. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.
Downloadable file (.docx): Warfarin Medication Card
Clinical Reasoning and Decision-Making Activity 1
A client who was treated in the hospital for DVT in his left leg has been prescribed warfarin.
- The client asks, “Will the warfarin dissolve the clot in my leg?” What is the nurse’s best response?
The nurse plans to assess the client’s lab work before administering the warfarin.
- What blood test(s) are important to monitor for clients taking warfarin, and what is the therapeutic range?
The nurse knows that the client will need to monitor his diet when taking warfarin.
- What dietary instructions should be provided to the client?
The nurse plans to provide client education regarding this newly prescribed medication.
- Outline the topics to cover with this high-risk medication.
- What is the reversal agent for warfarin?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 7: Cardiovascular Medications Answer key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
Direct Factor Xa Inhibitor: Rivaroxaban
Rivaroxaban (Xarelto) is a selective Xa inhibitor. Rivaroxaban is a relatively newer class of anticoagulant and has some advantages over warfarin. It works quickly, has a fixed dosage, lower bleeding risk and no need for monitoring. Another med in this class is apixaban.
Mechanism of Action
Rivaroxaban is a selective inhibitor of factor Xa and indirectly inhibits platelet aggregation induced by thrombin. It binds directly with factor Xa resulting in the inhibition of thrombin.it binds to both free and clot bound factor Xa which is different than heparin.
High bioavailability following oral administration. Highly protein bound, excreted in the urine and in the liver.
Indications for Use
Rivaroxaban is indicated for prevention or treatment of DVT and PE. It is used to prevent the risk of stroke with atrial fibrillation. In combination with aspirin, it is indicated to reduce the risk of major cardiovascular events such as cardiovascular (CV) death, myocardial infarction (MI) and stroke, and in clients with chronic coronary artery disease (CAD) or peripheral artery disease (PAD).
Nursing Considerations
Administration: oral form, take with or without food. Take with water and ensure adequate hydration.
Avoid with end stage renal disease or advanced liver disease
Overdose: in the case of an overdose, treat with activated charcoal to avoid further absorption. Andexanet can be given as an antidote.
Drug Interactions: rivaroxaban levels can be altered by any drug that inhibit or induce CYP3A4 and P-glycoprotein. For example, phenytoin and St John’s Wort can reduce rivaroxaban’s effects. Check monographs and consult with the pharmacist.
Pregnancy: not safe with pregnancy
Food interactions: Grapefruit interferes with the metabolism of rivaroxaban, resulting in higher dosages. The furanocoumarins in grapefruit inhibit the enzyme CYP3A4, which reduces the metabolism of rivaroxaban. Avoid eating grapefruit or drinking grapefruit juice, or limit to 1-2 glasses a week. It is safe to drink or eat other fruits, such as orange juice.
Adverse/Side Effects
As with all anticoagulants, there is a risk of bleeding. Compared to warfarin, the risk of bleeding is low.
High Alert Med: Epidural or spinal hematomas may occur in clients who are anticoagulated with rivaroxaban and are receiving neuraxial anesthesia or undergoing spinal puncture. These hematomas may result in long-term or permanent paralysis.
Client Teaching
- Clients should report any signs of unusual bleeding or bruising to the healthcare provider.
- Inform the prescriber of all prescriptions, OTC medications, vitamins, and herbal products.
- Consult with the prescriber if planning on taking any new medications or supplements.
- Advise client about avoiding grapefruit or limiting to only only 1-2 glasses per week.
Direct Thrombin Inhibitors: Dabigatran
Dabigatran (Pradaxa) is a direct-acting thrombin inhibitor. It has many advantages over warfarin, such as no need for monitoring, less risk of bleeding, and predictable effects so less restrictions based on the client’s age.
Mechanism of Action
Dabigatran is a competitive, direct thrombin inhibitor. Because thrombin enables the conversion of fibrinogen into fibrin during the coagulation cascade, its inhibition prevents the development of a thrombus.
It is well absorbed in the GI tract with low protein binding. It is not metabolized by the liver. Renal excretion.
Indications for Use
This drug is used to prevent or treat deep vein thromboses (DVT) or pulmonary emboli (PE). It is also used for prevention of stroke and systemic embolism with nonvalvular atrial fibrillation.
Nursing Considerations
Administration: oral form, give with or without food.
Overdose: Idarucizumab, a specific reversal agent, is available for urgent care or emergency operation client care.
Pediatrics: Safety and effectiveness have not been established.
Drug Interactions: there are fewer drug interactions than with warfarin, but caution with P-glycoprotein modulators.
Adverse/Side Effects
High Alert Med: Epidural or spinal hematomas may occur in clients who are anticoagulated with dabigatran and are receiving neuraxial anesthesia or undergoing spinal puncture. These hematomas may result in long-term or permanent paralysis.
Risk of bleeding can be fatal (DailyMed, 2025).
Client Teaching
- Clients should report any signs of unusual bleeding or bruising to the healthcare provider.
- Dispose of dabigatran bottles four months after opening.
- inform their health care provider of all prescriptions, OTC medications, vitamins, and herbal products.
Thrombolytic: Alteplase (tPA)
Alteplase (tPA) is a thrombolytic used to break up clots. It is also known as tissue plasminogen activator and it is one of three drugs that can be used to remove a clot. It has a very short half-life of 5 minutes so it can open a clogged artery rapidly. It is often given with heparin to prevent re-occlusion of the affected blood vessel.
It can also be used to unplug central lines, but at much smaller dosages (McCuistion et al, 2018).
Mechanism of Action
Alteplase binds to fibrin in a thrombus and converts the entrapped plasminogen to plasmin, which is an enzyme that digests the fibrin meshwork of clots. Plasmin also degrades fibrinogen and other clotting factors, resulting in the breakdown of the clot.
Indications for Use
Alteplase is indicated for the acute treatment of myocardial infarction (MI), stroke, or massive pulmonary embolism (PE). It is also used to clear central lines such as a peripherally inserted central line catheter (PICC).
It is important to understand that Alteplase is considered a “clot buster” whereas previous anti-platelet drugs do not clot-bust but rather make the platelets less sticky. This makes Alteplase a high risk medication. Since it cannot differentiate between what clot you want to dissolve, it basically floats through the blood destroying all clots.
Nursing Considerations
Administration: given IV, dosage is based on weight. Bolus dose of 15 mg, then 50 mg infused over 30 minutes, hen 35 mg infused over 60 minutes (Rosenjack Burchum & Rosenthal, 2019).
Alteplase should be given as soon as possible for the best outcome. The best results are within 2-4 hours of symptom onset or sooner.
Monitor:
- Vital signs before and during treatment, then at least q 4 hour.
- Assess for bleeding q 15 minutes during first hour of therapy, then every 15-30 minutes for the next 8 hours and then every 4 hours for the duration of therapy. Frank bleeding can occur from IV sites, body orifices, melena stool, joint pain and coffee ground emesis. If uncontrolled bleeding occurs, stop therapy and report immediately.
- Labs: prior to and during therapy, labs may include CBC, fibrin/fibrin degradation product, PT, thrombin time, aPTT, cross match
Occluded venous access device: 2 mg/2 mL into occluded catheter. May repeat once in 2 hours if still occluded (Vallerand & Sanoski, 2024).
The drug is contraindicated in situations in which the risk of significant bleeding is greater than the potential benefit such as:
- Active internal or intracranial bleeding
- History of recent stroke
- Recent (within 3 months) intracranial or intraspinal surgery or serious head trauma
- Presence of intracranial conditions that may increase the risk of bleeding (e.g., some neoplasms, arteriovenous malformations, or aneurysms)
- Current severe uncontrolled hypertension
- Recent major surgery
Significant post-administration monitoring is performed due to the risk of life-threatening bleeding.
Adverse/Side Effects
High Alert Med: This drug can cause significant, sometimes fatal, internal or external bleeding, especially at arterial and venous puncture sites.
Avoid intramuscular injections for at least 24 hours and perform venipunctures carefully and only as required.
It can increase the risk of thrombo-embolic events in clients with high likelihood of left heart thrombus, such as clients with atrial fibrillation.
Client Teaching
For treating an embolus: client should be on bedrest and avoid unnecessary procedures such as shaving or vigorous tooth brushing.
Explain the purpose of the therapy and the need for close monitoring.
Inform client to report any potential signs of bleeding, such as bruising, black stools or joint or abdominal pain.
(Vallerand & Sanoski, 2024)
Comparing Medications for Blood Coagulation
To support your learning, you can access the Chapter 7 Blood Coagulation Modifiers medication table medication table. This is a downloadable and editable document to allow you to update and add content. In clinical practice, ensure to access current drug manuals and agency policy prior to administration.
Critical Thinking and Decision-Making Activity 2
Complete the following questions. Refer to the answer key for the correct answers.
Joseph, 59 years old, has sudden onset of 4/10 substernal chest pain.
- His partner gives him two low-dose aspirins to chew while waiting for the ambulance. Is this good advice?
- Joseph arrives at the hospital. An ECG and troponin levels are done. He is diagnosed with a non-ST-elevation MI. He is ordered nitroglycerin spray to help relief his chest pain. The nurse prepares to give the nitrospray. The nurse recalls the correct administration technique:
- “Shake the canister, hold it upside down, and spray onto the client’s throat.”
- “Spray the medication under their tongue and do not swallow immediately.”
- “Inhale deeply while spraying the medication into your mouth.”
- “Apply the spray to the skin of your chest, covering an area 2 inches wide.”
- Which side effect should the nurse anticipate with a client taking nitroglycerin?
- Severe hypotension
- A persistent, severe cough
- Headache
- Increased heart rate (bradycardia)
- Joseph’s chest pain is resolved with two sprays of nitroglycerin. Later that day, he has had an angiogram of his heart and a stent was inserted into one of his coronary arteries. Upon returning to the ward, he is ordered Clopidogrel 300mg po, followed by 75 mg po daily. What is the purpose of this type of dosing? What does clopidogrel do?
- After a few days, Joseph is going home. He is prescribed:
- Nitroglycerin spray for chest pain, one spray at a time up to 3 sprays. Wait 5 minutes between sprays.
- Aspirin 81 mg po once a day
- Clopidogrel 75 mg once a day
What might be important for teaching him about his antiplatelet therapy?
- Joseph is wondering why his friend takes warfarin for his heart issues. He asks if he should also be on warfarin as well. What will the nurse tell him?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 7: Cardiovascular Medications Answer key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
References
Anderson, P., & Townsend, T. (2015). Preventing high-alert medication errors in hospital patients. American Nurse Today, 10(5). https://www.americannursetoday.com/wp-content/uploads/2015/05/ant5-CE-421.pdf
Arif, H., & Aggarwal, S. (2023). Salicylic acid (aspirin). In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK519032/
BC Guidelines. (2015). Warfarin therapy management: Appendix A. https://www.healthlinkbc.ca
Blausen.com staff (2014). “Medical gallery of Blausen Medical 2014”. WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436
DailyMed. (2025a). Rivaroxaban. U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/
DailyMed. (2025b). Warfarin. U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/
Dr Matt & Dr Mike. (2020, May 12). Blood clotting (hemostasis) [Video]. YouTube. https://www.youtube.com/watch?v=ZcoEajlESiI
Institute for Safe Medication Practices Canada (ISMP Canada). (2006). Appropriate anticoagulant use: A patient safety priority. ISMP Canada Safety Bulletin, 6(10). https://ismpcanada.ca/wp-content/uploads/ISMPCSB2006-10Anticoagulant.pdf
Institute for Safe Medication Practices Canada (ISMP Canada). (2020). Medications most frequently reported in harm incidents over the past 5 years (2015–2020). ISMP Canada Safety Bulletin, 20(11). https://ismpcanada.ca/wp-content/uploads/ISMPCSB2020-i11-Medications-Reported-Harm.pdf
Iqbal, A., Lopez, R., & Hai, O. (2022). Antiplatelet medications. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK537062/
Kushner, A., West, W. P., Suheb, M. Z., & Pillarisetty, L. S. (2024). Virchow triad. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/
McCuistion, L. E., Vuljoin-DiMaggio, K., Winton, M. B., & Yeager, J. J. (2018). Pharmacology: A patient-centered nursing process approach. Elsevier.
Ministry of Health. (2023). Warfarin. BC Guidelines. https://www2.gov.bc.ca
Patel, S., Singh, R., Preuss, C. V., & Patel, N. (2024). Warfarin. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/
Patel, P., & Varacallo, M. (2025). Low-molecular-weight heparin (LMWH). In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/
Rosenjack Burchum, J., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier.
Vallerand, A. H., & Sanoski, C. A. (2024). Davis’s Canadian drug guide for nurses (19th ed.). F. A. Davis.
Wallentin, L., Becker, R. C., Budaj, A., Cannon, C. P., Emanuelsson, H., Held, C., Horrow, J., et al. (2009). Ticagrelor versus clopidogrel in patients with acute coronary syndromes. The New England Journal of Medicine, 361(11), 1045–1057. https://doi.org/10.1056/NEJMoa0904327
Media Attributions
- 7.10a File:1909 Blood Clotting.jpg by OpenStax College/Anatomy and Physiology CNX at Wikimedia Commons; used under a CC BY 3.0 license.
- 7.10b “Bayer Aspirin Low Dose” by Mike Mozart on Flickr is licensed under CC BY 2.0 license.
- 7.10c Mechanism of action of anti-platelet medications is created by Sheila Odubote, TRU Open Press; subject to the CC BY-NC-SA license.
- 7.10d An activated platelet and the mechanism of action of coagulation modifiers, ticagrelor, clopidogrel and aspirin is created by Sheila Odubote, TRU Open Press; subject to the CC BY-NC-SA license.
- 7.10e Blausen 0034 Angioplasty Stent 01 – Percutaneous coronary intervention. by BruceBlaus Wikimedia Commons is used under a
- 7.10f: left: “Heparin Sodium sample.jpg” by LHcheM at Wikimedia Commons is licensed under CC BY-SA 3.0 and right: “Heparin in Dextrose Injection” is from DailyMed/NIH, retrieved from Chippewa Valley Technical College and used under a CC BY 4.0 is licensed under CC BY 4.0 license.
- 7.10g Coagulation Cascade is created by Sheila Odubote, TRU Open Press; subject to the CC BY-NC-SA license.
- 7.10h Petechia on the back of a client by James Heilman, MD at Wikimedia Commons is used under a CC BY-SA 4.0 license.
- 7.10i syringe-disposable-syringe-blister-103059 by stux at Pixabay is used under the Pixabay Content License.
- 7.10j”Warfarintablets5-3-1.jpg” by Gonegonegone at Wikimedia Commons is licensed under CC BY-SA 3.0 ↵

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}