7.8 Anti-hypertensives V2
Hypertension occurs when an individual’s blood pressure is above normal limits for a sustained period of time. The current hypertension guidelines by Hypertension Canada is a BP over 130/80. Hypertension can be either primary (essential) due to genetic and environmental factors or secondary due to other diseases such as renal disease, preeclampsia or thyroid disease. It can occur at any age, including children, although we mostly see hypertension in the middle age adult and older, or with clients with risk factors. For clients at higher risk, such as those with diabetes mellitus, cardiovascular disease, dyslipidemia, or renal disease, the target BP may be lower. Pharmacological treatment will begin when the BP is over 140/90, or if cardiovascular disease then treat if BP over 130/90 (Goupil et al, 2025).
There are over 14 different classes of drugs to treat hypertension. To understand why there is so many classes of meds, we go back to the physiological changes that contribute to high blood pressure. The mechanisms that regulate blood pressure are:
- Neural: sympathetic NS receives messages from baroreceptors and chemoreceptors to change vessel diameter in response to low BP. If BP is too low, the brainstem stimulates:
- heart (activates B1 receptors in the heart)
- blood vessels (activates alpha-1 receptors in the endothelial cells that line blood vessels, leading to vasoconstriction. BP can also be high due to structural remodelling that can lead to the hardening of the arteries.
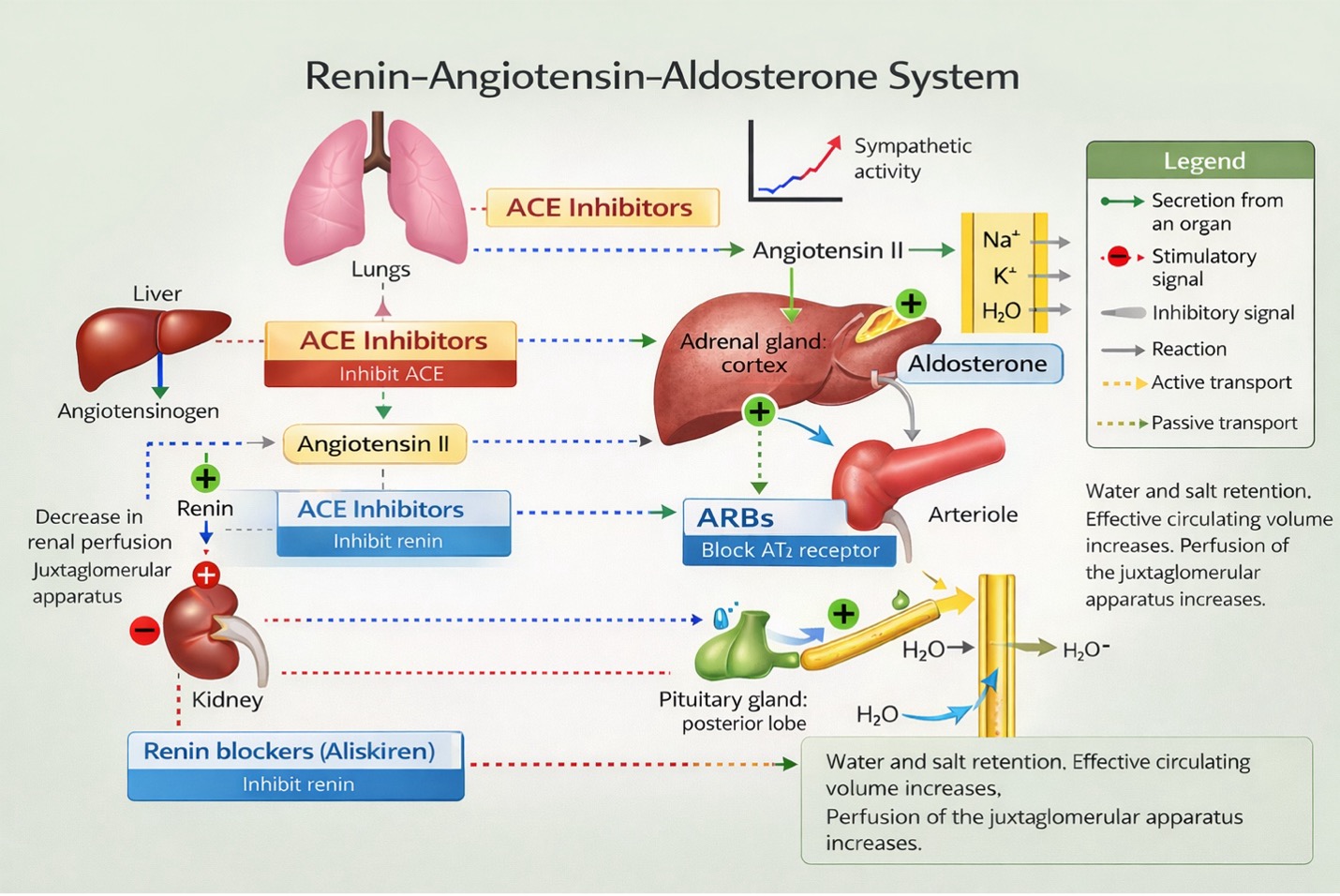
- Hormonal: RAAS (renin angiotensin aldosterone system) is activated in response to low blood volume. Review the RAAS as an important determinant of blood pressure and fluid volume.
- Renal: the kidney has a central role in BP regulation. When BP falls, the GFR also lowers, promoting the retention of Na, Chl and water. This increase in blood volume, results in an increase in venous return to the heart, increased CO, and increased BP.
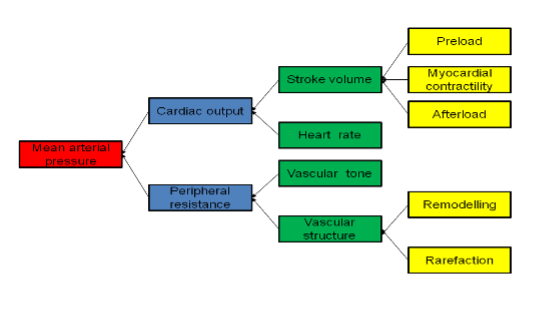
To lower blood pressure, medications are chosen to reduce heart rate, myocardial contractility, blood volume, venous return and lessen the tone of the arteriolar smooth muscle. Recall that blood pressure can be defined as:
Arterial blood pressure (BP) = cardiac output (CO) x peripheral resistance.
An increase in either CO or peripheral resistance, will increase BP. To take it a step further, the diagram 7.8a shows the other factors that will impact CO or peripheral resistance, and ultimately BP.
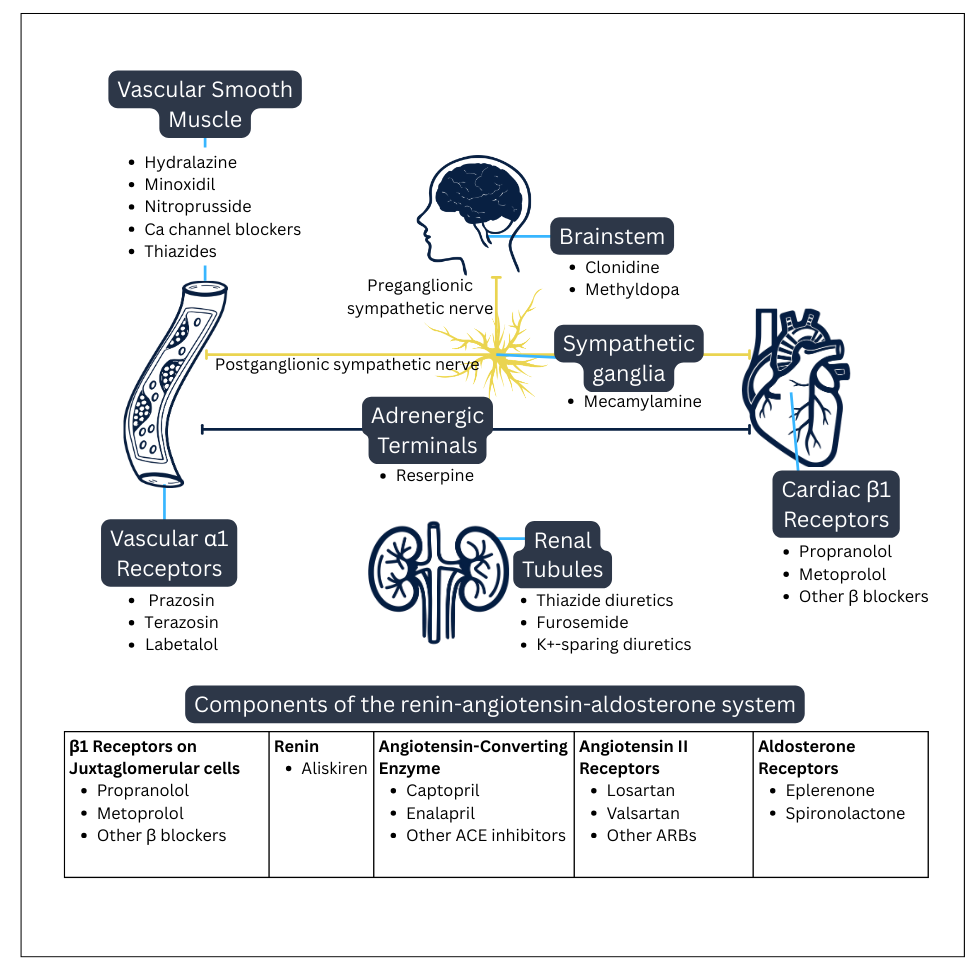
As mentioned above, there are 14 different classes of meds to lower blood pressure. Refer to the diagram below for all the sites of action of antihypertensives and the medications.
Refer to the chart at the end of this unit for an overview of antihypertensives and sites of action.
Depending on their blood pressure and other factors such as other health issues (i.e. renal, cardiac health issues) and cost considerations, clients may be started on one antihypertensive but the current guideline is for triple therapy with three different classes of anti-hypertensives. The benefit is the dosages will be lower and less potential side effects and they all working synergistically to manage blood pressure.
Clients need to be also implementing lifestyle changes such as diet, exercise and cessation of smoking. Client resources on lowering blood pressure are available through HealthLinkBC – Lifestyle Steps to Lower Your Blood Pressure (www.healthlinkbc.ca).
First line treatment of blood pressure:
- Thiazide-type diuretics: hydrochlorothiazide. This med will be covered in the diuretic unit
- Calcium channel blockers: Dihydropyridines (amlodipine)
- Angiotensin-converting enzyme (ACE) inhibitors: ramipril and angiotensin II receptor blockers (ARBs): losartan
(BC Guidelines.ca, 2020)
Other medication classes that are also commonly used, but not first line, are beta blockers (Bisoprolol, Metoprolol), alpha-2 agonist (clonidine), direct-acting vasodilators (hydralazine) and thiazide-like diuretics (indapamide).
This unit will cover only a few common medications. Some of the classes of meds have been covered in other units.
In chapter 4: Autonomic Nervous System:
- Unit 4.12 beta blockers (metoprolol, propranolol),
- Unit 4.10 alpha-2 agonist (clonidine)
This unit will cover:
- Meds that alter RAAS:
- Angiotensin Converting Enzyme Inhibitors
- Angiotensin Receptor Blocker (ARB)
- Direct-acting vasodilators: hydralazine
- Calcium channel blocker: amlodipine
Drugs that suppress RAAS: ACE inhibitors, Angiotensin receptor blockers
ACE Inhibitor (Angiotensin Converting Enzyme)
ACE inhibitors are a widely used for as antihypertensives. There are a number of medications in this class including ramipril, captopril, enalapril, among others. They have slightly different formulations from each other, but all work similarly. ACE inhibitors have a good safety profile.
In this unit, our prototype med will be Captopril. Note that all ACE inhibitors end in ‘pril’
Mechanism of Action
This medication blocks the conversion of Angiotensin I to Angiotensin II in the renin-angiotensin-aldosterone system. This action prevents vasoconstriction and aldosterone-mediated volume expansion, resulting in vasodilation and sodium and water excretion by blocking aldosterone.
Captopril improves cardiac output and reduces blood pressure by:
- Decreasing peripheral vascular resistance
- Reducing preload by causing vasodilation and natriuresis
- Reduces afterload by inhibiting the formation of angiotensin II
The second effect of ACE inhibitors is they also inhibit the breakdown of bradykinin. This results in vasodilation and also bronchoconstriction from bradykinin lodging in the bronchioles. Symptoms include a cough and in rare cases, angioedema.
What is bradykinin and why is asking about a cough important?
Bradykinin is a substance involved in the inflammatory process and has a role to play in sensitizing somatosensory fibers causing hyperalgesia, and it also has a role in mediating pro-inflammatory peptides and the local release of histamine.
Bradykinin is normally broken down by an enzyme called kininase. Kininase and ACE are the same enzyme. When ACE inhibitors are taken, they inhibit the breakdown of bradykinin, thereby increasing bradykinin levels. Typically, this is of no concern, but in some clients, they develop a dry cough which is due to higher levels of bradykinin. The elevated bradykinin may result in angioedema. As such, if someone is on an ACE inhibitor and develops a cough, they are switched to an ARB which does not have any effect on bradykinin.
See more information about the renin-angiotensin-aldosterone system in the “Review of Basic Concepts” section of this chapter.
Indications for Use
Cardioprotective effects: ACE inhibitors are an antihypertensive of choice for patients with hypertension, heart failure, post-MI ventricular dysfunction or diabetic neuropathy (Marte et al, 2024). It prevents remodeling of the left ventricle and also cardiac and vascular hypertrophy. They are effective at reducing mortality with these effects.
They are indicated as first-line treatment for patients with chronic kidney disease with evidence of proteinuria.
ACE inhibitors are used for clients with a cardiac history such as heart failure, recurrent stroke prevention and post-MI.
ACE inhibitors are also used for diabetic nephropathy, which is the leading cause of end-stage kidney disease (ESKD). This condition is due to microvascular complications of diabetes in both type 1 and type 2 diabetes. Captopril decreases the rate of progression of renal insufficiency by controlling blood pressure (Marte et al, 2024).
Nursing Considerations
Administration: oral BID or TID. Take one hour before meals as food decreases bioavailability. Enalapril can be given both oral and IV.
Monitor:
- Obtain baseline electrolytes and renal panel. Repeat these labs yearly.
- Blood pressure prior to therapy and then the following two weeks. Once stabilized, q 4 months.
Renal impairment: as it is excreted by the kidney, reduced dosage is required.
Liver impairment: avoid in clients with severe liver disease such as cirrhosis and ascites.
Pregnancy: do not give if pregnant or plan to become pregnant. Captopril will cause fetal birth defects such as skull hypoplasia, impaired renal function, hypotension, and fetal death.
Use with caution with clients who have diabetes.
Use with caution or avoid with Black people due to a slightly higher risk of angioedema. ACE inhibitors are also less effective in lowering blood pressure in this population (Nkunu et al, 2026).
Can cause hyperkalemia, monitor for ECG changes or symptoms such as nausea, palpitations, muscle pain or paresthesia (Marte et al, 2024). Clients with renal impairment, diabetes or who are on potassium supplements are more at risk.
Drug Interactions:
- Avoid use with other medications that increase potassium (i.e. potassium sparing diuretics).
- May increase risk of lithium toxicity.
Adverse/Side Effects
Side Effects include:
- Frist dose hypotension: profound hypotension after taking the first dose. Assess BP prior to dose and then 2 hours post. Ensure client safety to prevent falls.
- Orthostatic hypotension, dizziness, syncope
- Metallic taste
- Cough: dry, non-productive. Occurs in 20% of people. Can start within one week to 6 months after initiating therapy. If it develops, switch to an ARB.
Adverse Effects:
- Hyperkalemia aldosterone production is decreased which normally promotes K excretion in the kidney. Monitor serum potassium levels.
- Increased BUN and Creatine, decreased GFR: anticipate slight decrease. Caution with renal insufficiency
- Angioedema: rare. May experience increased facial swelling or difficulty swallowing or breathing should seek emergency medical attention. Report a persistent cough or angioedema to the health care provider (DailyMed, n.d.)
- Neutropenia
Client Teaching
- Medications should be taken as directed. Take one hour before meals on an empty stomach.
- Clients taking ACE inhibitors should be cautioned to avoid salt substitutes or foods high in potassium.
- May alter sense of taste, but this generally resolves within 2-3 months of medication therapy.
- If persistent dry cough develops, see prescriber. Will be switched to an ARB or other antihypertensive.
- Inform prescriber if plan to get pregnant or are pregnant.
- If weight gain and swelling of feet or ankles, see prescriber.
- Seek immediate medical assistance if swelling of the throat, lips or tongue.
- Change positions slowly, may become dizzy or lightheaded

Downloadable file (.docx): Captopril Medication Card
Angiotensin II Receptor Blocker (ARB)
ARBs are similar to ACE inhibitors in that they act on the renin-angiotensin-aldosterone system (RAAS). They are well tolerated, and often prescribed to clients unable to take ACE inhibitors due to the drug-induced cough. Both ARBs and ACE inhibitors have similar efficacy and indicated for similar conditions such as hypertension and diabetic neuropathy (Khalil & Zeltser, 2024). Losartan is an example of an Angiotensin II receptor blocker.
Mechanism of Action
ARBs act similarly to ACE inhibitors to lower blood pressure. ARBs prevent the angiotensin II mediated vasoconstriction and release of aldosterone, but do so by blocking the action of angiotensin II (ACE inhibitors block the formation of angiotensin II). The result is vasodilation and decreased peripheral resistance. It also has renoprotective effects in type 2 diabetes. It can also reduce the risk of stroke with clients with hypertension with left ventricular hypertrophy (Mulla, Patel & Siddiqui, 2024).
Indications for Use
ARBs are used to treat hypertension and to prevent nephropathy in diabetic clients. It is also beneficial for clients with hypertension and left ventricular hypertrophy to help prevent ventricular remodelling.
Nursing Considerations
Administration: well absorbed orally, with onset of action in 6 hours and duration of action 24 hours. Take the med at the same time each day. If taken with food, absorption will be slowed down.
Monitor serum potassium levels at initiation of therapy and regularly.
Do not administer to clients who are pregnant due to risk of fetal harm. It is not recommended for children under 6.
Hepatic impairment: Anticipate dosage adjustment with hepatic impairment.
May cause renal failure in clients with renovascular disease, volume depletion or taking NSAIDs.
Risk of hyperkalemia: risk increases if concurrent renal impairment, diabetes or use of potassium supplements.
Adverse/Side Effects
Side effects: hyperkalemia, fatigue, diarrhea, dizziness, nausea
Adverse effects:
- Renal insufficiency. Assess for proteinuria periodically
- Upper respiratory tract infection
- Hypotension
- Gastritis
- Urinary tract infection
- Angioedema: facial swelling or difficulty breathing, seek medical help
(BC Guidelines.ca, 2020; Mulla, Patel & Siddiqui, 2024)
Client Teaching
- Medications should be taken as directed, at the same time each day.
- Clients should not discontinue therapy unless directed to do so by their healthcare provider.
- Patients should be careful to avoid salt substitutes and foods with high levels of potassium. Do not take potassium supplements unless directed by your prescriber.
- ARBs may cause orthostatic changes and patients should be cautioned to change positions slowly.
Direct-Acting Vasodilators
Hydralazine and minoxidil are examples of direct vasodilators. They are an effective antihypertensive, but do have a number of side effects that prevents them from being a first line therapy.
Nitroprusside is another direct acting vasodilator but is reserved for life threatening hypertension. It is administered IV and works within a few minutes. This med would be given in critical care areas.
Hydralazine will be our prototype medication.
Mechanism of Action
Hydralazine’s direct mechanism of action is unknown, but it causes vasodilation via direct relaxation of vascular smooth muscle. It works on the dilation of arterioles without much effect on the dilation of veins. Peripheral vasodilation results in a reduction of blood pressure and decreased vascular resistance. It also leads to a compensatory baroreceptor-medicated release of epinephrine and norepinephrine which increases venous return and cardiac output. As the sympathetic nervous system is stimulated, this leads to tachyphylaxis and tachycardia (Herman, Bruss & Tivakaran, 2023).
Indications for Use
Hydralazine is used to treat essential hypertension not responsive to other medications. It can be used for hypertensive emergencies and acute onset hypertension during pregnancy, along with labetalol.
Nursing Considerations
Administration: oral or IV.
- For oral, it is given up to QID, with doses tapered up depending on effect.
- For IV dosages during hypertensive emergencies, effects occur within 5 to 30 minutes with a total duration of 2 to 6 hours (Herman, Bruss & Tivakaran, 2023).
Monitor:
- heart rate, blood pressure and ECG before therapy and regularly
- Risk of orthostatic hypotension. Ambulate clients slowly and take BP lying, sitting, and standing or as per orders.
Do not abruptly discontinue medication.
If reflex tachycardia occurs, may be treated with a beta-adrenergic med.
Use with caution in clients with coronary artery disease, mitral valve rheumatic heart disease, and cerebral vascular accidents.
This medication should only be used in pregnancy if the benefits outweigh the risks, due to lack of safety studies.
Adverse/Side Effects
Reflex tachycardia, monitor ECG or assess heart rate and blood pressure closely. Clients may feel palpitations.
Other: tremors, numbness, tingling, disorientation, nasal congestion, headache, nausea, vomiting, and diarrhea are effects associated with hydralazine (Medline, n.d.).
Adverse effects:
Systemic lupus erythematosus (SLE): a chronic disease that causes inflammation in the connective tissue. It affects many organs including skin, joints, kidneys, lungs, central nervous system, and blood-forming (hematopoietic) system. Although rare, this adverse effect places hydralazine in a third line therapy. Although lupus symptoms can vary, monitor for a characteristic sign of SLE, a flat, red rash across the cheeks and bridge of the nose. This rash is called a “butterfly rash” because of its shape (Medline, n.d.).
Client Teaching
- Clients should remain compliant with the therapeutic dosing regimen, even if symptoms resolve. The client should be cautious not to double up on medication doses. Additionally, the client should consult the healthcare provider for follow-up instruction if two or more doses of medication are missed.
- Clients should be instructed to monitor their weight and assess for fluid retention in the feet and ankles.
- Risk of orthostatic hypotension, advise client to mobilize slowly.
- Instruct client to report any rashes and fatigue.
- Instruct client to report any angina, faintness, dizziness, or numbness and cool extremities.
- Client or caregiver should take clients blood pressure as directed.
Calcium-Channel Blockers
There are two types of Calcium channel blockers (CCB). Non-dihydropyridines (verapamil, diltiazem) and dihydropyridines (amlodipine, nifedipine). Although both types cause dilation of arterioles, non-dihydropyridines also have effects on the heart by decreasing cardiac conduction and contractility (Rosenjack Burchum & Rosenthal, 2019).
This section will focus on dihydropyridines that have a greater affinity for peripheral smooth muscle and ultimately decrease blood pressure.
Our prototype drug will be amlodipine.
Mechanism of Action:
CCBs bind to receptors on L-type voltage-gated calcium channel. This results in the calcium channel being blocked and the inhibition of calcium influx into cardiac (myocytes, SA and AV nodes) and vascular smooth muscle cells. In the heart, this leads to a decrease in conduction and a decrease in the workload of the heart. In the blood vessels, this leads to vasodilation. Amlodipine has a greater affinity for vascular smooth muscle leading to dilation of peripheral arteries, decreased vascular resistance (afterload) and decreased blood pressure (Bulsara, Patel, & Cassagnol, 2024).
CCB also have an effect on the pancreatic islet cells. It inhibits the release of insulin. In an overdose situation, this would lead to hyperglycemia.
Indication of Use
Amlodipine is used for hypertension. It is also prescribed for stable and variant angina. With variant angina, it relaxes the coronary artery spasm. Off label, it can also be used for Raynaud’s phenomena, left ventricular hypertrophy and diabetic neuropathy.
Nursing Considerations
Administration: oral, once a day dosing. It can be taken with or without food. Peak concentration is 6-8 hours, with a long half life with terminal elimination of 30-50 hours. It is extensively metabolized by P450 enzymes in the liver.
Dosage adjustment with liver impairment. No lower dosage with renal impairment.
Pregnancy: can be used safely during pregnancy.
Drug Interactions:
- NSAID use can decrease the effects of CCB
- Grapefruit can increase the effects of CCB (flavonoid and nonflavonoid components of grapefruit interferes with CYP3A4 activity)
- Clarithromycin or erythromycin can decrease metabolism of CCB, leading to hypotension.
- If taken with high doses of statins, there is an increased risk for myopathy and rhabdomyolysis (Bulsara, Patel, & Cassagnol, 2024). Figure 7.8d Brown coloured urine that is characteristic of rhabdomyolysis.

Monitoring:
- Labs: renal (creatinine and BUN) and hepatic panel
- Assess BP and HR prior to initiating therapy and regularly. If SBP <100 hold med, or as ordered.
- Take BP lying, sitting and standing to assess for orthostatic hypotension.
- Assess for adverse effects such as headache, constipation, lightheaded, flushing, peripheral edema.
Amlodipine is contraindicated in patients with heart failure, severe aortic stenosis, unstable angina, severe hypotension, chronic constipation, and hepatic impairment (BC Guidelines.ca, 2020; Bulsara, Patel, & Cassagnol, 2024).
Adverse/Side Effects
Side effects: headache, constipation
- Other: side effects related to vasodilation: pedal edema, flushing, headache, palpitations
Adverse Effects:
- Angina, heart failure, pulmonary edema, tachycardia, bradycardia, skin rashes
Client teaching:
- Clients should remain compliant with the therapeutic dosing regimen, even if blood pressure improves. Take med once a day. The client should be cautious not to double up on medication doses.
- Clients should be instructed to monitor blood pressure regularly during therapy.
- Assess for fluid retention in feet and ankles.
- Risk of orthostatic hypotension, advise client to mobilize slowly.
- Avoid grapefruit juice
- Can cause constipation, increase fluids and fiber.
The following tables provide an overview of Anti-hypertensive Medications effects on the body. Table 1 provides an overview of the different sites in the body and the drug effects. Table 2 provides the sites of drug action within the RAAS.
Anti-hypertensive Medication Cards
The following medication cards are to assist in your learning of the content and to use in the practice setting. They are editable med cards and are intended for you to change or add content. The med cards are not intended to replace referring to a current drug guide to ensure correct use of the medications. Chapter 7 Cardiovascular Anyhypertensive Med Cards
Overview of Sites of Drug Action and their Effects
| Site of Drug Action* | Representative Drug | Drug Effects |
| Brainstem | Clonidine | Suppression of sympathetic outflow decreases sympathetic stimulation of the heart and blood vessels. |
| Sympathetic ganglia | Mecamylamine | Ganglionic blockade reduces sympathetic stimulation of the heart and blood vessels. |
| Adrenergic nerve terminals | Reserpine | Reduced norepinephrine release decreases sympathetic stimulation of the heart and blood vessels. |
| Cardiac beta1 receptors | Metoprolol | Beta1 blockade decreases heart rate and myocardial contractility. |
| Vascular alpha1 receptors | Prazosin | Alpha1 blockade causes vasodilation. |
| Vascular smooth muscle | Hydralazine | Relaxation of vascular smooth muscle causes vasodilation. |
| Renal tubules | Hydrochlorothiazide | Promotion of diuresis decreases blood volume. |
Overview of Sites of Drug Action and the Renin-Angiotensin-Aldosterone System
| Site of Drug Action* | Representative Drug | Drug Effects |
| Beta1 receptors on juxtaglomerular cells | Metoprolol | Beta1 blockade suppresses renin release, resulting in (1) vasodilation secondary to reduced production of angiotensin II and (2) prevention of aldosterone-mediated volume expansion. |
| Renin | Aliskiren | Inhibition of renin suppresses formation of angiotensin I, which in turn decreases formation of angiotensin II and thereby reduces (1) vasoconstriction and (2) aldosterone-mediated volume expansion. |
| Angiotensin-converting enzyme (ACE) | Captopril | Inhibition of ACE decreases formation of angiotensin II and thereby prevents (1) vasoconstriction and (2) aldosterone-mediated volume expansion. |
| Angiotensin II receptors | Losartan | Blockade of angiotensin II receptors prevents angiotensin-mediated vasoconstriction and aldosterone-mediated volume expansion. |
| Aldosterone receptors | Eplerenone | Blockade of aldosterone receptors in the kidney promotes excretion of sodium and water and thereby reduces blood volume. |
Retrieved from: Rosenthal & Rosenjack Burchum. (2025). Drugs for Hypertension – Clinical GateClinical Gate
Clinical Reasoning and Decision-Making Activity 1
A male 65-year-old client has the following medications ordered: metoprolol 100 mg daily, lisinopril 5 mg daily, verapamil ER 100 mg daily, and hydrochlorothiazide 25 mg daily. He has a history of hyperlipidemia, hypertension, and coronary artery disease. The client asks the nurse, “Why do I have to take so many medications?”
- What is the class and mechanism of action of each of these medications?
- What is the nurse’s best response to the client’s question?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 7: Cardiovascular Medications Answer key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
Clinical Reasoning and Decision-Making Activity 2
A client has hypertension and is started on the ACE inhibitor, enalapril. After six months, their prescriber ordered blood work, and discovered the client’s serum potassium level of 5.5 meq/mL.
- What is the rationale for the higher potassium level? Is there a concern?
- To lower the potassium levels, what would the nurse want to include in a teaching session?
- The clients blood pressure is still high despite starting on enalapril. The prescriber has now started amlodipine (CCB). What health teaching should the client be aware of with amlodipine?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 7: Cardiovascular Medications Answer key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
References
Adams, M., Urban, C., El-Hussein, M., Osuji, J. & King, S. (2018). Pharmacology for Nurses. A pathophysiological approach (2nd Canadian ed.). Pearson Canada Inc: Ontario.
BC Guidelines.ca (2020). Hypertension: diagnosis and management. Appendix D. htn-full-guideline.pdf
DailyMed (n.d.). Captopril. National Library of Medicine. DailyMed – CAPTOPRIL- captopril tablet CAPTOPRIL tablet
Herman, L., Bruss, Z. & Tivakaran, V. (2023). Hydralazine. National Library of Medicine. Hydralazine – StatPearls – NCBI Bookshelf
Kishen G. Bulsara; K., Patel, P. & Cassagnol, M. (2024). Amlodipine. National Library of Medicine. StatPearls [Internet]. Amlodipine – StatPearls – NCBI Bookshelf
Marte, F., Sankar, P., Patel, P., & Cassagnol, M. (2024). Captopril. National Library of Medicine. Captopril – StatPearls – NCBI Bookshelf
Mulla, A., Patel, P. & Siddiqui (2024). Losartan. National Library of Medicine. StatPearls [Internet]. Losartan – StatPearls – NCBI Bookshelf
Nkunu, V., Campbell, L., Tsuyuki, R., Bello, A., & Ringrose, J. (2026). Are angiotensin converting enzyme inhibitors effective in the treatment of hypertension in Black patients? Canadian Journal of Cardiology Open. https://doi.org/10.1016/j.cjco.2026.01.011
Rosenjack Burchum, J., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
Rosenthal, L. & Rosenjack Burchum, J. (2025). Lehne’s Pharmacotherapeutics for Advanced Practice Providers. Elsevier Canada. Drugs for Hypertension – Clinical GateClinical Gate
Media Attributions
- 7.8a File:Mean arterial pressure.png by Adh30 at Wikimedia Commons is used under a CC BY-SA 4.0 license.
- 7.8b Sites of action of antihypertensive drugs. Drugs for Hypertension was recreated/ adapted by TRU Open Press using Canva from Clinical Gate, 2017 (Figure 39.2); subject to the CC BY-NC-SA 4.0 license.
- 7.8c The effects of antihypertensive medications on RAAS is by Sheila Odubote, TRU Open Press; subject to the CC BY-NC-SA 4.0 license.
- 7.8d File:RhabdoUrine.JPG is by James Heilman, MD at Wikimedia Commons, used under the CC BY-SA 3.0 license.

{kind=link}
{kind=link}