7.11 Diuretics V2
Diuretics are a category of medications that are used extensively for a variety of edematous and non-edematous conditions that result in fluid-buildup in the body. Most diuretics act by targeting ion transport receptors on the luminal surface of the renal tubules. Conditions we will commonly see diuretic therapy include acute or chronic renal disease, with the goal to help the kidney work more effectively. Diuretics are used when there is a fluid or volume overload issue, often due to heart failure, which might be evident in pulmonary edema or peripheral edema. With end-stage liver disease, the client often experiences ascites, and diuretics will also be used. We also see diuretics prescribed for essential hypertension, with the goal to decrease blood volume and therefore blood pressure. Lastly, diuretics are sometimes used to eliminate toxic substances from the body through diuresis (Arumugham, & Shahin, 2023).
To understand how diuretics work, you need to have a good understanding of the renal system and Renin Angiotensin Aldosterone System. Take time now to review the components of the kidney and RAAS.
Watch: Kidney function and anatomy | Renal system physiology | NCLEX-RN | Khan Academy
To monitor how well the kidney is functioning, a client will be ordered lab tests. Often referred to as a renal panel, it will include BUN, eGFR, and electrolytes:
Blood urea nitrogen (BUN):
- Measures how much nitrogen is in the blood.
- Urea, or BUN, is a nitrogen-containing waste product of protein and amino acid metabolism. The liver releases urea into blood and it is filtered by the kidneys into urine.
- ↑’d levels of urea due to dehydration, kidney disease, ↑ protein intake or ↑ protein breakdown from muscle damage or GI bleeds.
Estimated glomerular filtration rate (eGFR):
- Measures the filtration rates according to your protein levels, age, sex, height and weight.
- This is the best indicator of glomerular function. GFR normally decreases with age.
Serum creatinine:
- This test looks for creatinine buildup. Creatinine is a waste product that comes from the digestion of dietary protein and the normal breakdown of muscle tissue.
- Numerous factors can affect creatinine levels including diet; muscle (weight of your muscles); malnutrition; and other chronic illnesses.
Serum Potassium:
- Therapeutic serum potassium level is 3.5-5 mEq/L.
- Potassium is often excreted with diuretic therapy, and must be closely monitored to ensure within therapeutic limits.
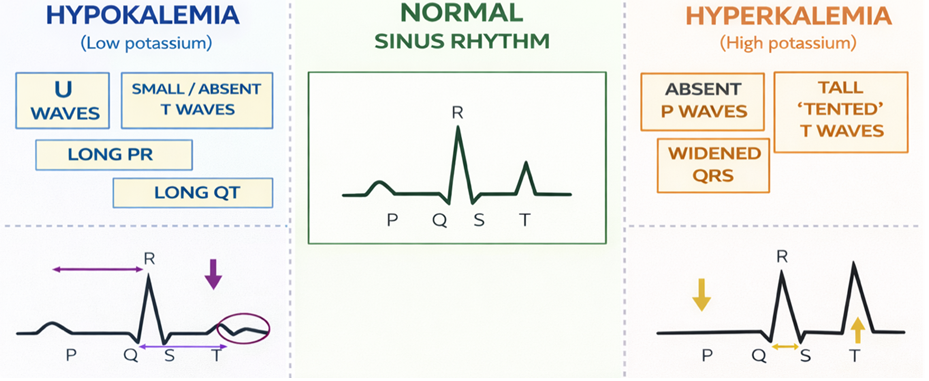
- Mild hypokalemia can present as mild muscle weakness. As potassium levels drop, dysrhythmias are common, with flattened T waves and depressed ST depression. Potassium levels below 2.5 mEq/L, serious and even lethal dysrhythmias, along with muscle cramps and weakness.
Serum Sodium:
- Therapeutic serum sodium level is 136–145 mEq/L.
- Mild hyponatremia can cause nausea and fatigue, with lower sodium levels resulting in headache, lethargy and seizures.
Refer to the National Kidney Foundation website for information on monitoring lab values: How to Read Your Kidney Health Lab Results | National Kidney Foundation
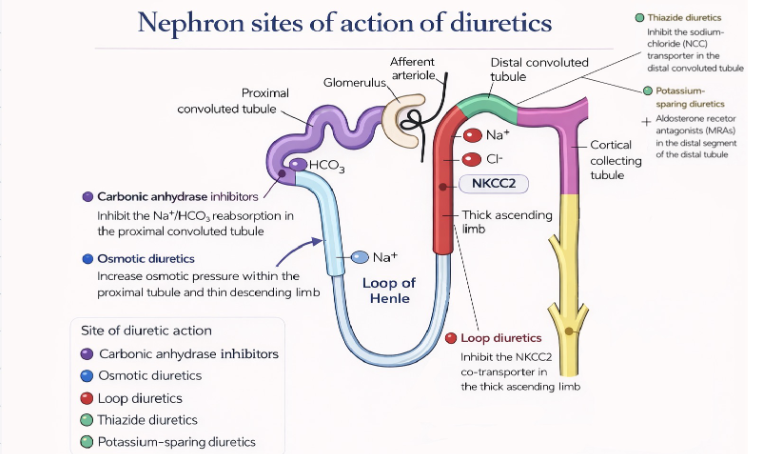
Most diuretics all have similar mechanism of action in that they block sodium and chloride reabsorption, which creates an osmotic pressure within the nephron that prevents the passive reabsorption of water. This results in water and solutes retained within the nephron, and then excreted out in the urine. But, each diuretic works on a different part of the renal tubules, so their overall effects will differ with the amount of diuresis and the degree that solutes that are reabsorbed.
General Overview of Diuretics:
- all work in a particular area of the nephron. Those that act earlier in the nephron (where there is a higher solute concentration) has the greater diuretic effect.
- all diuretics cause diuresis but some have a greater effect. The choice of diuretic depends on kidney and other health issues.
- all have the potential to lower BP by lowering vascular volume
- most can cause hypovolemia due to excess fluid loss
- all have the potential to cause electrolyte and acid base imbalances
There are five categories of diuretics, these are loop, thiazide and thiazide-like, osmotic, carbonic anhydrase inhibitors, and potassium sparing. The choice of diuretic will depend on the health issue, lab work and the client’s clinical presentation. Many clients with advanced disease will have complex medication profiles and may be on more than one diuretic.
Example in Practice 1:
A client has heart failure secondary to an incompetent aortic valve. The client is experiencing shortness of breath from pleural effusions and pulmonary edema. This client is prescribed a loop diuretic to help rid the body of the extra fluid. Depending on the client’s potassium levels, they may be prescribed a second diuretic, such as a potassium-sparing diuretic or a carbonic anhydrase inhibitor.
Example in Practice 2:
Client B has essential hypertension. The client is on anti-hypertensive medications, but the prescriber feels a decrease in preload may also be helpful. To eliminate some intravascular fluid that is contributing to a higher preload, a thiazide diuretic may be ordered. Thiazides work on the distal convoluted tubule so they are not as powerful but will still decrease preload and decrease systemic vascular resistance due to their direct vasodilatory effects (Arumugham & Shahin, 2023).
Example in Practice 3:
Client C has acute kidney injury from sepsis. The acute kidney injury has caused decreased urine output. The client is ordered a loop diuretic to help with the fluid overload and reduce pulmonary edema. Loop diuretics will not help resolve the kidney injury or prevent dialysis, they will help rid the body of excess fluid (Hegde, 2020).
In this unit we will review the following three classes of meds:
- loop (furosemide)
- thiazide (hydrochlorothiazide)
- potassium sparing (spironolactone)
As we will not cover osmotic diuretics or carbonic anhydrase inhibitors in detail in this unit, so the following brief overview is provided.
Osmotic diuretics
Osmotic diuretics (Mannitol) work by increasing the osmolarity of the tubular fluid in the proximal tubule and the loop of Henle. It is given IV, and exerts its effect by creating a strong osmotic force that inhibits passive reabsorption of water, which then leads to increased urination.
Mannitol is used for elevated intracranial pressure (ICP) and cerebral edema (head injured patients) and to prevent renal failure in urgent situations of severe hypotension, shock, and oliguric acute kidney injury. For all uses, it is mostly given in higher acuity or critical care areas due to close assessment and monitoring that is required due to the powerful nature of the med and the instability of the client’s state.
Carbonic anhydrase inhibitors
Carbonic anhydrase inhibitors, Acetazolamide, is also sometimes used as an adjunct diuretic for heart disease. It is also prescribed for many non-cardiac conditions such as glaucoma, epilepsy and for altitude sickness.
Carbonic anhydrase is found in the proximal tubule and red blood cells. Acetazolamide prevents the breakdown of carbonic anhydrase, leading to sodium, bicarbonate, and chloride being excreted along with water. By causing a loss of HCO3+ in the urine, this leads to metabolic acidosis. The body then compensates for this loss of bicarbonate by decreasing CO2 levels and ultimately higher partial pressures of O2 in the blood. For clients with altitude sickness, this effect will decrease the incidence of tissue hypoxia (Arumugham & Shahin, 2023).
Loop Diuretics
Loop diuretics are the most effective diuretic to produce the most loss of fluid and electrolytes. They are used extensively for many conditions that cause fluid overload. Within this class, Torsemide, bumetanide and furosemide are loop diuretics; with furosemide the most common med ordered in this class.
Furosemide will be our prototype med.
Mechanism of Action
Loop diuretics action is in the thick ascending loop of Henle. It inhibits the absorption of sodium and chloride by inhibiting the Na-Cl cotransporter system. By blocking the reabsorption of sodium and chloride, passive reabsorption of water occurs, with subsequent excretion of water. Along with free water excretion, potassium is unable to be reabsorbed back into the lumen, leading to a loss of potassium. And, to a lesser extent, the loss of calcium and magnesium (Huxel, Raja & Ollivierre-Lawrence, 2023).
Indications for Use
Loop diuretics are very potent diuretics and are used when a client has an exacerbation of fluid overload. Furosemide is used to treat clients with edema, hypertension, pulmonary edema, peripheral edema and congestive heart failure. IV furosemide is used to urgently treat pulmonary edema.
Nursing Considerations
Administration: oral, IM or IV. For acute fluid overload, such a pulmonary edema, intravenous route would be given. Prolonged effects can occur if the client has any hepatic or renal dysfunction.
- IV: The usual initial dose is 20-40 mg, repeated in 1-2 hours depending on effect. Onset of action within 5 minutes, with duration of action 2 hours. Administer by slow IV push. For high dose therapy, furosemide continuous infusions with a rate of 4mg/min may be ordered.
- Oral: the usual initial dosage is 20 mg, up to 80 mg. Onset of action within 60 minutes. The peak effect occurs within the first or second hour. The duration of diuretic effect is 6 to 8 hours.
When possible, loop diuretics should be administered in the morning, and evening doses should be avoided (unless urgent) so that sleep is not disturbed.
Monitoring:
- Before therapy, assess intake and output, signs of fluid overload, blood pressure and heart rate and lung sounds.
- During therapy, monitor for dehydration, hypotension and electrolyte imbalances that can occur with excessive diuresis:
- Dehydration: assess for dryness of mouth, thirst, weakness, lethargy, drowsiness,
- Electrolyte disturbances, particularly hypokalemia: confusion, nausea, headache, muscle pains or cramps, muscular fatigue, tachycardia, arrhythmias,
- Anticipate potassium loss and the likelihood of potassium supplements. Potassium sparing diuretics such as spironolactone is often ordered to counterbalance the potassium losses from loop diuretics.
Laboratory Tests: Monitor serum electrolytes, (particularly potassium), creatinine and BUN should be done frequently during the first few months of furosemide therapy and periodically thereafter.
Risk of ototoxicity: assess for tinnitus and hearing loss. Hearing loss is more common with rapid or high dose administration or with renal dysfunction. Hearing loss may be reversible.
Older adult: Use cautiously for clients with decreased renal function. Kidney function should be monitored closely for all clients because this is a potent medication that works within the kidney tubules.
(Huxel, Raja & Ollivierre-Lawrence, 2023; Vallerand & Sanoski, 2024)
Drug Interactions
- Digoxin: Monitor the client closely for hypokalemia if furosemide is used concomitantly with digoxin. Hypokalemia may increase the risk of digoxin toxicity and subsequent risk of dysrhythmias.
- Lithium: furosemide will lower sodium levels, which can result in lithium accumulating to toxic levels. Close monitoring of lithium levels with reduction of lithium dosage may be required.
- Sulfa allergy: slight risk of allergic reaction if taking furosemide and the client has a sulfa allergy.
Contraindicated in anuria, severe cases of electrolyte depletion, and hepatic coma.
Pregnancy: Treatment during pregnancy requires monitoring of fetal growth. There are no human studies available, so use furosemide only if absolutely needed.
Tolerance: Tolerance can develop and can cause a ‘breaking’ phenomena where there is a rebound retention of Na+ due to increased absorption from the distal tubules. The result is a progressive decrease in urinary output after repeated doses of furosemide. This can occur with chronic diuretic therapy. Diuretic resistance can also occur when the maximum dose of furosemide does not produce the anticipated diuresis. This can be due to hypertrophy of the distal tubule which increases sodium reabsorption. Close intake and output are required when furosemide is first administered or in acute situations of fluid overload in order to assess for the diuretic effect. With long term therapy, clients should be taught to monitor fluid changes such as edema, weight gain or respiratory changes that indicate fluid overload.
Huxel, Raja & Ollivierre-Lawrence, 2023
Adverse/Side Effects
Adverse effects include dehydration, hypotension, and electrolyte imbalances.
Excess loss of sodium, chloride, magnesium and potassium. Hypokalemia, with a serum potassium of less than 3.5 mEq/L, can lead to serious dysrhythmias.
- Close monitoring of serum electrolytes is essential during therapy. Hypokalemia can first present with muscle weakness and cramping, tingling or numbness, fatigue and heart palpitations. As the level drops lower, if not corrected, it can lead to paralysis, difficulty breathing and an irregular heart beat. The ECG complex will display a prolonged PR interval, long QT, small or absent t waves (Cleveland Clinic, 2022). See figure 7.11b
- Potassium supplements many be added as a scheduled medication to decrease risk of hypokalemia.
Dehydration can occur due to fluid loss. Monitor for signs of dehydration such as dry mouth, thirst, weakness, lethargy, oliguria.
Hypotension can occur due to excess fluid loss and the relaxation of venous smooth muscle. Monitor for signs such as light-headedness and dizziness.
The risk of ototoxicity increases with concurrent use of other drugs such as aminoglycosides and renal impairment (DailyMed, 2025).
Hyperglycemia risk is rare, and due to the inhibition of insulin release. For diabetic clients or prediabetes, this may require closer monitoring and anti-diabetic medication adjustments.
Client Teaching
- Take medication as prescribed. Do not double up doses if a dose is missed
- Monitor blood pressure and pulse
- Report any rashes, muscle weakness, muscle cramps, nausea, dizziness, tingling of extremities
- Inform prescriber if planning on becoming pregnant or if pregnant.
- Advise clients to change position slowly, as they may experience orthostatic changes.
- Clients should also report weight gain of more than three pounds in a day or five pounds in a week to their healthcare provider.
- Clients should also be encouraged to enjoy potassium-rich foods during loop diuretic drug therapy. Avoid high sodium foods.
Furosemide Medication Card
Now let’s take a closer look at the medication card for furosemide. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.

Downloadable file (.docx): Furosemide Medication Card
Clinical Reasoning and Decision Making Learning Activity 1
Mrs. Smith is a 79-year-old widow who has lived alone for the past 5 years. Three years ago she was hospitalized for a myocardial infarction, which resulted in heart failure. She is compliant with her medications, which include digoxin (Lanoxin) 0.125 mg daily, furosemide (Lasix) 40 mg daily, and potassium (K-Dur) 20 mEq daily.
Recently Mrs. Smith ran out of her potassium and thought that because it was “just a supplement,” it would be OK to go without it until the next time she went to town to fill the prescription. She has not taken her potassium for a week.
Today she is at the clinic with generalized weakness, fatigue, nausea, and diarrhea. Her BP is 104/62, pulse 98 bpm and slightly irregular, RR 20, and temp 36 C. Blood is drawn and shows serum sodium level of 150 mEq/L (normal 135-145 mEq/L), digoxin level of 2.6ng/ml (normal 0.6-1.2 nmol/L) and potassium level of 3.0 mEq/L (normal 3.5-5.0 mEq/L).
- What assessments should a nurse do before and after administering a diuretic?
- What are the signs and symptoms of digoxin toxicity? What can happen to a client who has toxic levels of digoxin?
- Furosemide can cause dehydration. What might be some symptoms of dehydration?
- What electrolyte imbalance(s) can occur in clients taking furosemide (Lasix)?
- What relationship exists between this client’s furosemide, digoxin, and potassium levels?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 7: Cardiovascular Medications Answer key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
Thiazide and Thiazide-like Diuretics
Thiazide diuretics are considered first line diuretic for hypertension. It has similar effects as loop diuretics as it increases the excretion of sodium, potassium and chloride as well as water. The amount of diuresis is much lower than loop diuretics making it a safer medication.
Our prototype med will be hydrochlorothiazide (HCTZ)
Mechanism of Action
Thiazide diuretics, also known as benzothiadiazides, work in the early segment of the distal convoluted tubule to directly inhibit the sodium chloride cotransporter, thereby preventing sodium reabsorption and inducing both natriuresis and diuretic effects (Akbari & Khorasani-Zadeh, 2023). In this part of the nephron, only 10% of filtered sodium and chloride is normally reabsorbed, so the diuretic effect is much lower than loop diuretics. They are not effective for immediate diuresis.
Thiazide-like diuretics, lack the benzothiadiazide backbone in the chemical properties, and is considered better at managing hypertension and less effect of electrolyte disturbances. Two meds in this category are metolazone and indapamide (Akbari & Khorasani-Zadeh, 2023).
Indications for Use
Hydrochlorothiazide diuretics are used to manage hypertension and adjunct therapy for peripheral edema with heart failure, hepatic cirrhosis, corticosteroids and estrogen therapy. HCTZ can also be used to manage edema from renal dysfunction, such as nephrotic syndrome.
What is Nephrotic Syndrome?
Nephrotic syndrome is proteinuria with a low serum albumin level and edema. It is characterized by a loss of protein in the urine of greater than 3 grams a day or the presence of 2 grams of protein per gram of urine creatinine. It can be due to a number of kidney diseases and from systemic diseases such as diabetes and lupus erythematosus (Sinnakirouchenan & Batuman, 2025).
Nursing Considerations
Administration: oral form only. Take in the morning with food. Taper dosages depending on effect.
- Onset of action within 2 hours, peaks in 4 hours, and lasts 6-12 hours.
Monitoring:
Thiazides will cause the same loss of electrolytes and water, but to a much lesser extent.
- Electrolyte imbalances including hyponatremia, hypokalemia, and hypochloremia.
- Assess labs before and periodically during therapy.
- Hypokalemia can occur so if lower than 3.5 mEq/L, potassium supplements may be needed. Encourage potassium rich diet.
- Fluid loss and dehydration is a moderate risk. Assess for signs of dehydration, weakness, hypotension, and light-headedness.
- Monitor blood pressure and heart rate before dose and periodically afterwards.
- Monitor urine output
Contraindicated with clients with anuria or sulfa hypersensitivity. Use with caution with clients with renal disease.
Avoid NSAIDs as this may blunt the effect of diuretics.
Adverse/Side Effects
Adverse effects are similar to loop diuretics, with the exception that it does not cause ototoxicity.
- Electrolyte imbalances including hyponatremia, hypokalemia, and hypochloremia.
- Metabolic alkalosis
- Hyperglycemia due to a decrease in insulin secretion.
- Hyperuricemia due to increased urate reabsorption in the proximal tubule. May precipitate gout in clients with this disorder.
- Hyperlipidemia although MOA is unclear. Monitor LDLs, total cholesterol, cholesterol and triglycerides.
Risk of acute pancreatitis: Although rare, thiazides have a toxic effect on the pancreas and can lead to increased pancreatic secretions and ischemia.
Hypersensitivity reactions can occur so monitor for reactions that include rash, hives, angioedema, wheezing, and anaphylaxis.
(Akbari & Khorasani-Zadeh, 2023; Rosenjack Burchum & Rosenthal, 2019).
Client Teaching
- Clients should be instructed to take these medications at the same time each day and do not double up doses if a dose is missed.
- Notify their healthcare provider if they experience significant change in weight, such as 5-pound weight gain in one week.
- May cause orthostatic changes so individuals should change positions slowly. Monitor blood pressure periodically.
- Some clients may note increased photosensitivity, so protective measures such as sunscreen and covering up in the sun.
- Incorporate non-pharmacological measures to lower blood pressure, such as low sodium diet and exercise.
Potassium Sparing Diuretic
Potassium-sparing diuretics are used to treat or prevent hypokalemia associated with the use of loop diuretics and thiazide diuretics. It has a very mild diuretic effect, therefore it is rarely used alone as a diuretic. It can also be used with hepatic disease for those with ascites. There are two categories of potassium-sparing diuretics: aldosterone antagonists and non-aldosterone antagonists.
Spironolactone is an aldosterone antagonist and will be our prototype medication.
Mechanism of Action
Spironolactone acts primarily through competitive binding of receptors at the aldosterone-dependent sodium-potassium exchange site in the distal convoluted renal tubule. Spironolactone causes increased amounts of sodium and water to be excreted, while potassium is retained. The amount of diuresis is minimal, as much of sodium has already been absorbed by the time the filtrate reaches the distal nephron.
Indications for Use
Spironolactone is used primarily to treat resistant hypertension and edema in clients with heart failure and liver disease. It also has a cardioprotective effect in clients with heart failure due to the aldosterone blockade in the heart and blood vessels. It can also be used for hyperaldosteronism and polycystic ovary syndrome. Also used to counterattack potassium loss caused by other diuretics such as thiazides and loop.
Nursing Considerations
Administration: oral form only. Peak effect is 2-3 days with a duration of action of 2-3 days. Administer in the morning to avoid nocturia.
Monitoring:
- Blood pressure and heart rate prior to therapy and regularly, especially if given as an adjunct to antihypertensive therapy.
- Urine output and report if less than 30 ml/hour.
- Assess for hyperkalemia such as fatigue, muscle weakness, paresthesia, confusion, dyspnea, and cardiac arrythmias.
- Labs: electrolytes, BUN, creatinine, serum magnesium
Renal impairment: Use cautiously with clients who have renal impairment due to increased risk for hyperkalemia.
Use with caution with diabetic clients as it can cause hyperglycemia.
Drug interactions:
- Risk of hypotension if used with antihypertensive drugs
- NSAIDs may decrease spironolactone’s effects
- May increase the risk of lithium toxicity. Monitor sodium and lithium levels.
Adverse/Side Effects
- Electrolyte imbalances may occur including hyperkalemia, hyperglycemia, and hyperuricemia.
- Dehydration and hypotension: monitor blood pressure and signs of light-headedness or dizziness.
- Hypersensitivity reaction may occur, monitor for rash and discontinue if it develops due to risk of Steven Johnson syndrome.
- Endocrine effects such as erectile dysfunction, menstrual irregularities and gynecomastia may occur due to med being structurally similar to steroid hormones.
Client Teaching
- Clients should be instructed to take these medications at the same time each day. Take in the morning to avoid nocturia
- Notify their healthcare provider if they experience significant changes in weight.
- Diuretics may cause orthostatic changes, so individuals should change positions slowly. Avoid activities such as driving if feeling dizzy.
- Clients should be advised to avoid salt substitutes and foods that contain high levels of potassium.
- Monitor blood pressure regularly
- Inform male clients of potential for erectile dysfunction or gynecomastia. A lower dose may be required. Inform female clients of the potential for irregular menses.
Arumughan & Shahin (2023); Rosenjack Burchum & Rosenthal (2019); Vallerand & Sanoski, (2024)
Comparing Diuretic Medications
To support your learning, you can access the Chapter 7 Comparing Diuretic Medications table tables. This is a downloadable and editable document to allow you to update and add content. For clinical practice, ensure to consult current drug manuals and agency policy prior to administration.
Clinical Reasoning and Decision-Making Learning Activities 2
- A client is prescribed a thiazide (hydrochlorothiazide) for hypertension. The nurse notices they have a number of other health issues. Which health issue does this medication may cause concern?
- epilepsy
- heart failure
- gout
- COPD
- A client will be started on spironolactone for liver cirrhosis and ascites, as an additional diuretic. The nurse should monitor for which common side effect?
- tachycardia
- hypoglycemia
- hypertension
- gynecomastia
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 7: Cardiovascular Medications Answer key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
References
Akbari, R. & Khorasani-Zadeh, A. (2023). Thiazide diuretics. National Library of Medicine. StatPearls [Internet]. Treasure Island (Fl). StatPearls Publishing.
Arumugham & Shahin, 2023). Therapeutic uses of diuretic agents. National Library of Medicine. StatPearls [Internet]. Therapeutic Uses of Diuretic Agents – StatPearls – NCBI Bookshelf
Cleveland Clinic (2022). Hypokalemia. https://my.clevelandclinic.org/health/diseases/17740-low-potassium-levels-in-your-blood-hypokalemia
Daily Med (2025). Furosemide injection. U.S. National Library of Medicine. DailyMed – FUROSEMIDE injection, solution
Hegde, A. (2020). Diuretics in acute kidney injury. Indian Journal of Critical Care Medicine, 24(Suppl 3):S98-S99. doi: 10.5005/jp-journals-10071-23406. PMID: 32704212; PMCID: PMC7347069.
Huxel, C., Raja, A. & Ollivierre-Lawrence, M. (2023). Loop diuretics. National Library of Medicine StatPearls [Internet]. Loop Diuretics – StatPearls – NCBI Bookshelf
Rosenjack Burchum, J., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
Sinnakirouchenan, R. & Batuman, V. (2025). Nephrotic syndrome. Med Scape. https://emedicine.medscape.com/article/244631-overview?form=fpf
Media Attributions
- 7.11a Diuretics and sites of action on nephron is created by TRU Open Press; subject to the CC BY-NC-SA license.
- 7.11b The effects of hypokalemia and hyperkalemia on the ECG complex is created by Sheila Odubote, TRU Open Press; subject to the CC BY-NC-SA license.
