6.7 Adjuvant Analgesics V2
Learning Outcomes
- Describe the purpose of adjuvant medications in treating pain.
- Articulate the common adjuvant medications and how they promote pain relief.
- Understand the mechanism of action, indications for use, adverse effects and nursing considerations for muscle relaxants.
- Understand the mechanism of action, indications for use, adverse effects and nursing considerations for NMDA antagonist ketamine.
There are numerous adjunct medications and all have a place in providing pain relief for certain health issues. Medications used as adjuvant analgesics were developed for other purposes but were later found to be effective to treat pain. They are used to enhance analgesia and need to be used properly to provide effective pain management.
Many drug classifications have been found to be effective for pain management. Some classifications are:
- Antidepressants
- Antiepileptics
- Alpha 2-adrenergic agonists
- Botox
- Corticosteroids (dexamethasone, prednisone)
- Local anesthetics (lidocaine, bupivacaine)
- Muscle relaxants
- NMDA antagonists (Ketamine)
- Cannabinoids
The prescribing of adjuvant medications is often for clients with complex or chronic pain situations. For example, pain from cancer, fibromyalgia, multiple sclerosis, palliative or chronic pain post-injury that is not easily managed with typical analgesics or when avoiding or minimizing the use of opiates is desired. Often these pain syndromes are a result of a mixture of pain mechanisms, and therefore there is no simple formula available to manage the chronic complex pain state.
Before adjuvant medications are prescribed, the health care team completes a detailed health history including learning about the client’s other health issues, a thorough medication profile, the goal of care and the stage of disease.
Example in Practice
A client has breast cancer with metastases and is experiencing significant bony pain. They have been initially prescribed non-opioid and opioid pain medications with suboptimal results. After a detailed assessment, this client will continue with a opioid: Duragesic fentanyl patch, hydromorphone oral for breakthrough pain, and also be prescribed an adjuvant medication for persistent cancer pain syndrome. There are many options that can be used effectively and an individualized plan will be needed. Options could include the corticosteroid dexamethasone, bisphosphonates or an antidepressant (Mitra & Jones, 2011).
In this unit, we will start with a brief overview of some of the common adjuvant medications. A more detailed discussion of muscle relaxants and NMDA antagonists will be provided.
Antidepressants
Although antidepressants (AD) have been used as an adjunct to treat pain caused by arthritis, migraines, neuropathic pain and fibromyalgia, the research on the efficacy is not consistent. A meta-analysis has shown inconclusive evidence of the efficacy of AD to treat pain (Ferriera et al, 2023). Of the antidepressants, tricyclics have been reported to show moderate efficacy in treating cancer and neuropathic pain (Birkinshaw et al, 2023). Marks, Choi and Turpen (2024) prescribe serotonin and norepinephrine reuptake inhibitors (SNRIs): duloxetine for chronic pain with moderate effect across all outcomes measured. For clients with difficult to manage chronic pain or palliative clients, AD may provide some relief and worth trying.
Antiepileptics (anticonvulsants)
Antiepileptic drugs have shown some efficacy in treating neuropathic pain. Neuropathic pain is a result of damaged nerve fibers, so pain from causes such as post-op, would not be effective. Chronic nerve pain from diabetic neuropathy, postherpetic neuralgia, or central neuropathic pain post-stroke are some conditions that antiepileptics may be beneficial. Gabapentin and pregabalin are two meds that provide some relief. Gabapentin may also be prescribed for migraine headaches (Sealock & Seneviratne, 2021: Wiffen et al, 2013).
Local anesthetics
Local anesthetics work by blocking nerve impulses and provide effect pain relief to a localized area, often for a brief period of time. They can be applied topically prior to doing a painful procedure. They can be given via SQ injection to the injured area, for example prior to inserting stitches. Or can be injected directly into the tissues for a nerve block to a joint or extremity. Local anesthetics will be reviewed in unit 6.8.
Corticosteroids
Dexamethasone is the main corticosteroid that is often prescribed for chronic pain issues, especially related to cancer or palliative pain control. Corticosteroids reduce inflammation through inhibiting prostaglandin synthesis and reduce vascular permeability that results in tissue edema. They also reduce neuropathic pain through reducing spontaneous discharges in damaged nerve cells (Vyvey, 2010). Corticosteroids will be reviewed in chapter 9, endocrine unit.
Bisphosphonates
This class of drugs is used to treat osteoporosis and can slow down bone breakdown and reduce inflammation. Alendronate, one med in this classification, is also used for pain from bone metastases although the actual mechanism is uncertain. It would be a secondary medication for pain relief.
Medical Cannabis
Cannabis has been used for its psychoactive effects for a long time in Canada, and it was not until 1999 that it was approved for medicinal purposes. In Canada, 17.7% of those over the age of 15 used cannabis for medical reasons (Health Canada 2013b). In the last few decades, there has been considerable research exploring the beneficial effects of cannabis. ∆9-tetrahydrocannabinol (THC) is well-known for its psychotropic effects (feelings of euphoria, mood altering). Cannabinoids (CBD) does not have this mood altering effect and has been used to treat many health issues, such as nausea, appetite stimulation, pain relief and seizure prevention (Kallant & Porath-Waller, 2016).
With the more recent research and interest in the medicinal use of cannabis, as well as prompted by the unreliability of effects from smoking or ingesting cannabis, synthetic versions have been developed. Nabilone, Dronabinol, and Sativex are a few synthetic products available. For pain control, medicinal cannabis is approved for neuropathic pain, relief from muscle spasticity and for treating cancer pain. Adverse effects can include impaired cognitive functioning such as memory, coordination and judgment issues, and chronic bronchitis (Kallant & Porath-Waller, 2016; Schrot & Hubbard, 2016).
The cultivation of cannabis started in Neolithic China more than 6000 years ago. Research of the medical use of cannabis started in 1838 by Sir William B. O’Shaughnessy, who treated individuals in India with muscle spasms and convulsions. Medical use of cannabis mostly subsided after that time, due to the unpredictability of effects and variable potency found with ingesting or smoking cannabis (Kallant & Porath-Waller, 2016). In the 1960’s research increased again, and cannabidiol (CBD) and the most psychoactive cannabinoid delta-9-tetrahydrocannabinol (THC) were identified. Since then, more than 100 different cannabinoids have been discovered. Current studies are uncovering how cannabis has a role in modulating inflammatory and neuroprotective properties as well as other effects such as mood and daily functioning. The discovery of the endocannabinoid system (ECS) has also shown promise in understanding its central role in the regulation of many key functions to maintain homeostasis (Lanz et al, 2016).
Muscle Relaxants
Movement disorders are difficult to treat as the underlying cause of the pain or movement limitations can be due to skeletal, muscular, endocrine or nervous systems. A comprehensive assessment is ideal to best determine a treatment plan that may include drug therapy with antispasmodics, antispastics or benzodiazepines (covered in chapter 8). The utilization of muscle relaxants varies for treatment of acute and chronic pain. Choosing which drug to prescribe can be difficult as some of the drug’s mechanism of action are poorly understood as well as determining the underlying reason for pain (Chang, 2020).
Skeletal muscle relaxants can be divided into two categories:
Centrally acting skeletal muscle relaxants:
- Baclofen – used for spasticity
- Cyclobenzaprine – used for spasms (localized muscle spasm)
Direct-acting muscle relaxants:
- Dantrolene – used for spasticity
Defining the Terms: Spasticity and Spasms
Spasticity originates in the central nervous system. Spasticity disorders are characterized by increased muscle tone, spasm or loss of dexterity. Ie. Cerebral palsy, multiple sclerosis or stroke are examples. These conditions are treated with physical therapy and a combination of drugs.
Muscle Spasms are an involuntary contraction of a muscle or muscle group. The muscle becomes tightened, leading to a decreased ability to function. Causes can include localized muscle injury, acute or chronic pain syndromes and epilepsy. These conditions are treated with a combination of NSAIDs and centrally acting muscle relaxants, along with physiotherapy and non-pharmacological interventions (ie. massage, acupuncture, rest).
Anti-spastic medications are used for conditions such as cerebral palsy and multiple sclerosis. For ex., baclofen, dantrolene, tizanidine and diazepam (Benzodiazepine).
Anti-spasmodic medications are used for musculoskeletal conditions include cyclobenzaprine metaxalone, and methocarbamol (Robaxin).
In this section, we will review baclofen and cyclobenzaprine.
Baclofen
Indications for Use
Baclofen is used to treat muscle spasticity caused by multiple sclerosis, spinal cord injuries, or other spinal cord disorders. It helps reduce the frequency and severity of painful spasms in quadriplegic or paraplegic clients. Off label, Baclofen has also been used to treat clients with alcoholic liver disease, and reduce alcohol cravings and anxiety. It is also sometimes used for irretractable hiccups.
Mechanism of Action
Baclofen is a centrally-acting skeletal muscle relaxant. It acts within the spinal cord to suppress hyperactive reflexes involved in the regulation of muscle movements. It also is structurally similar to gamma-aminobutyric acid (GABA), aninhibitory neurotransmitter, leading to an inhibitory action of neuronal activity in the brain and spinal cord (Adams, 2019). By reducing the release of excitatory neurotransmitters in the presynaptic neurons and stimulating the inhibitory neuronal signals in the postsynaptic neurons, this results in spasticity relief (Ghanavatian & Derian, 2024).
Nursing Considerations
Administration:
- Baclofen is taken orally, with peak effect one-hour post-administration. The t1/2 is 4-5 hours, requiring multiple dosing throughout the day.
- Dose: 15-20 mg TID or QID. Maximum dosing 80mg/day.
- Doses are titrated up every 3 days.
- Take with or without food.
Intrathecal administration: may be injected into the lumbar region to reduce generalized spastic hypertonia post-stroke, or other cerebral or spinal spasticity.
Metabolism and Excretion: baclofen is metabolized in the liver, and 70% is eliminated in an unchanged form through the kidneys, with a small amount excreted in the feces. Doses are reduced for clients with renal insufficiency of a GFR 30-60 mL/min/1.73 m².
Baclofen is safe for clients 12 years and older. It is not advised for pregnancy due to risk of birth defects, so benefit vs risk needs to be considered. Very small amount of baclofen is found in breast milk, with the only caution is sedation in the infant.
Adverse/Side Effects
Baclofen is well tolerated, safe medication with rare adverse effects. It has a wide safety margin. Most adverse effects are on the CNS or GI systems.
- As a CNS depressant, drowsiness, dizziness, vertigo or light-headedness are common. These effects subside with continued use and they are minimized with titrated doses.
- GI effects can include nausea, vomiting and constipation.
- Urinary retention risk especially if the client has benign prostrate hypertrophy or is taking anti-cholinergic meds.
- Muscle weakness
Other adverse effects have been reported but rare, and include hypotension, peripheral edema, hypoventilation, insomnia, depression and impotence.
Abrupt Drug Withdrawal
Hallucinations, paranoid ideation and seizures have occurred on abrupt withdrawal of oral baclofen. Therefore, except for serious adverse reactions, the dose should be reduced slowly over 1 to 2 weeks when the drug is discontinued. Abrupt withdrawal of intrathecal baclofen can result in hyperpyrexia, altered mental state, rebound spasticity and muscle rigidity. Slow titration and close monitoring of the pump is required.
Overdose
Signs and symptoms of overdose include vomiting, muscular hypotonia, drowsiness, accommodation disorders of the eye, coma, respiratory depression, and seizures. There is no antidote, so supportive measures only.
Client Teaching
- Advise clients of the potential adverse effects. They should not drive if they experience confusion or drowsiness until those symptoms subside.
- Clients should be advised to change positions slowly because of the potential orthostatic changes that may occur.
- They should avoid concurrent use with alcohol or other CNS depressants as they will potentiate sedation and dizziness.
- Do not abruptly stop taking baclofen and see their prescriber for instructions to taper their dosages.
Ghanavatian & Derian, 2024; Rosenjack Burchaum & Rosenthal, 2019.
Baclofen Medication Card
Now let’s take a closer look at the medication card for baclofen. Medication cards like this are intended to assist students to learn key points about each medication. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.

Downloadable file (.docx): Baclofen Medication Table
Clinical Reasoning and Decision-Making Learning Activity 1
A client just started taking baclofen for muscle spasticity due to multiple sclerosis.
What teaching should the nurse provide?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 6: Pain and Mobility Medications Answer Key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
Cyclobenzaprine
Indications for Use
For clients with acute muscle spasm, treatment can include non-pharmacological measures, non-steroidal anti-inflammatories, and the use of a centrally acting muscle relaxant. Cyclobenzaprine is used to treat acute muscle spasms. It relieves muscle spasm locally, without interfering with the overall muscle function. It is a drug of first choice for acute muscle spasm.
Mechanism of Action
Cyclobenzaprine reduces tonic somatic muscle activity (depresses motor activity) at the level of the brainstem. It is structurally similar to tricyclic antidepressants.
Nursing Considerations
Administration: oral formula, well-absorbed from the GI tract.
- Immediate release: Onset of action: one hour, with peak in 4 hours.
- Also available in extended release.
- T1/2 is 1-3 days, with maximum effect may take 1-2 weeks.
Caution with hepatic impairment as the drug undergoes considerable enterohepatic recirculation. Lower dosages are required with liver disease.
Contraindicated or used with caution if taking antidepressants while on this med due to risk of serotonin syndrome.
Lifespan considerations:
- Children: safe for clients 15 years and older.
- Older adult: Use cautiously with older adults, as the frequency and severity of adverse events are increased, especially if also taking concomitant medications. Dosing for the older adult should begin with 5 mg dose and titrated slowly upward.
- Pregnancy and Breastfeeding: avoid with pregnancy as safety has not been established. Should not be used by breastfeeding women.
Adverse/Side Effects
Cyclobenzaprine is well tolerated. Most adverse effects are on the CNS and CV system and anticholinergic effects.
CNS: drowsiness, dizziness and fatigue.
CV: similar to tricyclic anti-depressants, it can cause sinus tachycardia and conduction delays. Caution with clients with a cardiac history.
Anti-cholinergic effects: dry mouth, blurred vision, photophobia, urinary retention and constipation. Use with caution with clients with benign prostrate hypertrophy, narrow-angle glaucoma and increased intra-ocular pressure.
Serotonin Syndrome:
The development of a potentially life-threatening serotonin syndrome has been reported with cyclobenzaprine hydrochloride when used in combination with other drugs, such as selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), tramadol, bupropion, meperidine, verapamil, or MAO inhibitors (MAOIs). The concomitant use of cyclobenzaprine hydrochloride with MAO inhibitors is contraindicated.
Serotonin Syndrome (Serotonin Toxicity)
Serotonin is a neurotransmitter that regulates mood, behaviour and other physiological functions. Serotonin syndrome occurs from an excessive serotonergic activity throughout the central nervous system that can be potentially life-threatening. Excess serotonin can be caused by therapeutic medication use (taking a large dose of a prescribed med), accidental medication interactions (taking more than one med that increases serotonin levels), using recreational drugs or an intentional overdose.
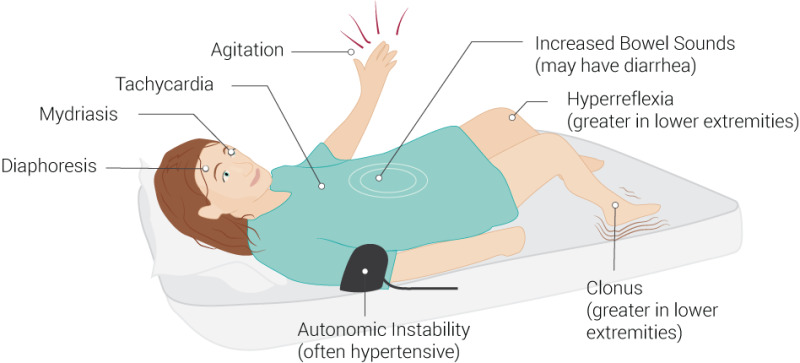
Serotonin syndrome symptoms may include:
- mental status changes (e.g., confusion, agitation, hallucinations),
- autonomic instability (e.g., diaphoresis, tachycardia, labile blood pressure, hyperthermia),
- neuromuscular abnormalities (e.g., tremor, ataxia, hyperreflexia, clonus, muscle rigidity),
- and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea).
The client typically feels unwell and seek help before life-threatening symptoms appear.
Treatment includes discontinuing any concomitant serotonergic agents if the above reactions occur, and supportive symptomatic treatment should be initiated. If concomitant treatment with cyclobenzaprine hydrochloride and other serotonergic drugs is clinically warranted, careful observation is advised, particularly during treatment initiation or dose increases.
Client Teaching
- Take as directed and inform prescriber of any change or additions of other medications including herbal supplements or recreational substances.
- Advise client of potential adverse effects of the medication.
- Change positions slowly because of the potential orthostatic changes that may occur.
- If taking more than one serotonergic medication, report any symptoms of toxicity.
- Avoid concurrent use with alcohol or other CNS depressants.
- Caution with driving as risk of sedation and dizziness
- Report any change in heart rate or rhythm.
- May cause constipation; increase fluids and fiber intake.
Cyclobenzaprine Medication Card
Now let’s take a closer look at the medication card for cyclobenzaprine (Opentextbc, n.d.)

Downloadable file (.docx): Cyclobenzaprine Medication Card
Clinical Reasoning and Decision-Making Learning Activity 2
A client asks if they can drive their car while taking cyclobenzaprine.
What is the nurse’s best response?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 6: Pain and Mobility Medications Answer Key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
References
Adams, M., Urban, C., El-Hussein, M., Osuji, J. & King, S. (2018). Pharmacology for Nurses. A pathophysiological approach (2nd Canadian ed.). Pearson Canada Inc: Ontario.
Birkinshaw, H., Fridrich, C., Cole, P., Eccleston, C., Serfaty, M., Stewart, G. … (2023). Antidepressants for pain management in adults with chronic pain: a network meta-analysis. Cochrane Database Systematic Review, 5(5), CD014682. PMCID: PMC10169288 DOI: 10.1002/14651858.CD014682.pub2
Ferreira, G., Adel-Shaheed, C., Underwood, M., Finnerup, N. O’Day, R…. (2023). Efficacy, safety, and tolerability of antidepressants for pain in adults: overview of systematic reviews. British Medical Journal, 380: e072415. doi: 0.1002/14651858.CD014682.pub2. PMID: 37160297
Ghanavatian, S. & Derian, A. (2024). Baclofen. National Library of Medicine. Baclofen – StatPearls – NCBI Bookshelf
Health Canada. (2013b). Canadian Alcohol and Drug Use Monitoring Survey (CADUMS). Ottawa, Ont.: Author. Retrieved from www.hc-sc.gc.ca/hc-ps/drugs-drogues/ stat/_2011/summary-sommaire-eng.php
Kallant, H. & Porath-Waller, A. (2016). Clearing the smoke on cannabis. Medical Use of Cannabis and Cannabinoids– An Update. Canadian Centre on Substance Abuse. ISBN 978-1-77178-363-7
Lanz C, Mattsson J, Soydaner U, Brenneisen R (2016) Medicinal Cannabis: In Vitro Validation of Vaporizers for the Smoke-Free Inhalation of Cannabis. PLoS ONE 11(1): e0147286. https://doi.org/10.1371/journal.pone.0147286
Marks, S., Choi, K., and Turpen, J. (2024). Tricyclic Antidepressants for pain. Palliative Care Network of Wisconsin.https://www.mypcnow.org/fast-fact/tricyclic-antidepressants-for-pain/
Muscle Cramps Image: https://www.istockphoto.com/en/photo/a-young-woman-got-severe-cramps-in-her-calf-at-night-while-sleeping-gm1467944141-499607613
Rosenjack Burchum, J., & Rosenthal, L. (2023). Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
Schrot, R. & Hubbard, J. (2016). Cannabinoids: Medical implications. Anesthesia Medicine, 48(3), 128-41. PMID: 26912385 DOI: 10.3109/07853890.2016.1145794
Sealock, K. & Seneviratne, C. (2021). Lilley’s Pharmacology for Canadian Health Care Practice (4th ed.). Elsevier: Canada
Vyvey, M. (2010). Steroids as pain relief adjuvants. Canadian Family Physician, 56(12), 1295-1297. https://pmc.ncbi.nlm.nih.gov/articles/PMC3001922/
Wiffen, P., Derry, S., Moore, R.A., Aldington, D., Cole, P., et al (2013). Antiepileptic drugs for neuropathic pain and fibromyalgia ‐ an overview of Cochrane reviews. Cochrane Database Systematic Review, 11, CD010567. doi: 10.1002/14651858.CD010567.pub2
Media Attributions
- 6.7a SerotoninSyndrome.jpg by Beckie Palmer on Wikimedia Commons is used under a CC BY 4.0 license.

{kind=link}