6.6 Opioid Analgesics and Antagonists V2
Learning Outcomes
- Describe the mechanism of action of opioid agonist and opioid antagonist medications.
- Discuss the primary effects, indications and nursing considerations for the different opioid medications, including, morphine, fentanyl, hydromorphone, codeine, and methadone.
- Understand how tramadol’s mechanism of action differs from opioid medications and articulate uses and important nursing considerations.
- Discuss the mechanisms of action, indications and nursing considerations for opioid antagonists, Naloxone and Suboxone.
- Apply this understanding when considering the nursing care of clients receiving these medications through critical thinking and application questions.
In this unit, we will look generally at opioid analgesics as they all have very similar effects.
Opioid Analgesics
There are several types of opioid analgesics, most are used to treat moderate-severe pain. They are used for many types of pain, often for acute (post-operative, post-injury), chronic pain conditions, chemotherapy and palliative pain. The type and dose of opioids that are ordered will differ depending on the use. All have the potential of addictive properties and misuse, and as such are a controlled drug and require a prescription. In Canada, they are placed in drug schedule 1A (prescription only, controlled substance). Clients who are on opioids for palliative purposes rarely leads to drug abuse or addiction (Fraser Health, 2006).
Most opioids that are prescribed are used along with non-opioid or adjunctive medications to improve pain control and lower the amount of opioids used.
Assessment of Pain
Prior to any administration of analgesics, a thorough assessment is required to best meet the needs of the client. Included in the assessment:
- Physical and psychosocial assessment
- Medication profile of all medications; prescribed, OTC and herbal supplements.
- Assessment of the pain including PQRST questioning
- Impact of pain on quality of life, ability to complete ADLs (activities of daily living) and functionality.
Mechanism of Action
Opioid receptors are located throughout central nervous system and in other locations in the body. Opioid receptors are proteins that respond to both natural opioids (enkephalins, endorphins) and opioid drugs. There are 3 types of opioid receptors: µ [mu], κ [kappa] and δ [delta]. Of these, two are primary receptors for pain: mu (morphine), kappa (butorphanol). Each receptor-drug complex results in pain relief, although some pairings have more sedative or euphoria effects than others.
The primary effect, pain relief, is achieved when opioids bind to receptors on neuronal cell membranes –> slows or stops the pain message to the brain.
Opioid receptors are located throughout the body. In the brain, they are located in the cerebral cortex, brain stem, and thalamus. In the respiratory system, they are located in the mechanoreceptors in the lungs and airways. They are located throughout the autonomic nervous system, and as such have an effect in the gastrointestinal tract and the urinary system. So, when opioid receptors are occupied by an opioid med, they occupy receptors in many parts of the body, not just the CNS to decrease pain. This helps explain the many adverse effects.
The following table provides a general overview:
| Receptor | Other effects | Pain relief effects |
| Mu (µ) | Respiratory depression | All have a role in pain relief |
| Kappa (κ) | Dysphoria, sedation | All have a role in pain relief |
| Delta (δ) | Mood | All have a role in pain relief |
Full agonists
Most opioid medications have agonist effects on opioid receptors. (refer to chapter 1 for an overview of agonist actions LINK PLEASE). Examples of agonist opioids including morphine, codeine, fentanyl, oxycodone, hydromorphone, and methadone.
Partial agonists
A few opioid analgesics have a partial agonist response. For example, Buprenorphine is a partial agonist that is considered a safe alternative to opioid use disorder and with managing severe pain not responsive to other alternative treatments. It is a partial agonist on the mu-opiate receptor, along with weak kappa receptor antagonist and delta receptor agonist. It is unique as it has a ceiling effect at higher doses, where it would then transition into an antagonist mode. This action decreases the respiratory depression risk (Kumar, Viswanath & Saadabadi, 2024).
Indications for use
For mild pain, non-opioid medications are effective. For more moderate to severe pain, opioid analgesics are prescribed and in conjunction with non-opioid options. In the hospital setting for acute pain, opioids that are frequently prescribed are morphine sulfate, fentanyl, or hydromorphone and all three can be given IV or oral. For pain control with more of a sustained effect or if the client can swallow, then oral formulas of morphine (MS Contin) or hydromorphone (oral, rectal formulas) can be ordered.
Unique Pain Situations
Palliative or long-term chronic pain: some clients will be prescribed a transdermal patch of fentanyl (Duragesic) along with possibly an oral opioid for breakthrough pain. Another alternative is to use adjunct medications, which can include non-opioid (NSAIDs, muscle relaxants, cannabinoids) options. Refer to the unit 6.7 for more information on adjunct med pain meds.
Break through dose (BTD)
Some clients are on a regular dose of analgesic but need extra pain relief for painful dressing changes, repositioning or other painful situations. In these cases, the physician will prescribe a PRN med to use along with the regularly scheduled analgesic. There are a few ways that are used to calculate BTD. One option is to start with a breakthrough dose 50% of the every 4-hour dose and then reassess daily. If the background dose is increased, then the breakthrough dose is also increased (Doulton, 2014). For example, the order reads:
Morphine 2 – 5 mg IV q 4 hours
Morphine 1 – 2.5 mg IV q 4 hours prn for breakthrough pain
Often, the background dose and breakthrough dose are the same opioid. Sometimes they are different. For example, if the client is on a fentanyl transdermal patch, the BTD will be an alternate med such as a short-acting morphine, oxycodone, or hydromorphone (Doulton, 2014).
Managing Pain in acute care settings: Patient-controlled analgesia
To provide more effective pain control in clients who are cognitively capable to follow the instructions, patient-controlled analgesia (PCA) is a good option. Opioids are commonly used in PCA include morphine, hydromorphone and fentanyl. To receive the opioid using a PCA device, the client pushes a button, which releases a specific dose but also has a lockout mechanism to prevent an overdose (McCuistion et al, 2018).
Read more about opioid usage in Canada at this Health Canada website.

Treatment with Opioids: general principles
- Opioids are a drug of choice for moderate to severe pain.
- Long lasting or continuous pain should be treated with sustained release opioids
- Use the oral route when able; there is no perfect route so the plan should be individualized for each client.
- Think about the 3 B’s when reviewing the physician’s orders: bowels, barfing and breakthrough. Is there a med or treatment plan for each?
- Ceiling effect: most opiates do not have a ceiling effect (Tramadol and Codeine are exceptions). Therefore, if the client is experiencing more pain (end of life, cancer pain, severe pain), then a higher dose of opiate can be given without achieving a maximum concentration.
- Allergies: most ‘allergies’ to opioids are not true allergies, but an adverse effect. Pruritis is a common adverse effect, and is sometimes mistaken for an allergy. If a true allergy exists for morphine or codeine, they might not be allergic to a different classification, such as synthetic fentanyl or semi-synthetic hydromorphone.
(Fraser Health, 2008; Adams et al, 2019)
Classification of Opioid medications
- Natural opiates are morphine and codeine, as they are derived from the unripe seeds of the poppy plant.
- Synthetic opioid meds are fentanyl, methadone
- Semi-synthetic opioid meds are oxycodone, hydromorphone
Why it matters? Pruritis occurs more with natural opiates instead of synthetic opioids. If a client has a true allergic reaction in one drug classification, they might be fine in a different classification.
Morphine
Is a natural opioid, derived from the unripe seeds of the poppy plant. Morphine is typically used as the standard which other opioids are measured against.
Fentanyl
Fentanyl is a semi-synthetic opioid. It is 80-100 times more potent than morphine. It is highly lipophilic. It is used for moderate to severe pain from intra-op, post op pain, chronic pain, breakthrough pain, and emergency pain control. It is highly lipophilic, with a rapid onset of action when given IV (one minute) and a short duration of action (one hour) making it ideal for procedural or emergency pain relief. For ongoing severe pain, transdermal patches are often prescribed.
Hydromorphone
Hydromorphone is a semi-synthetic opioid used for moderate to severe pain. It is 5-8 times more potent than morphine. Ie. Morphine 10 mg IV = Hydromorphone 2 mg IV. For clients with renal insufficiency, it is a good option over morphine. It has a faster onset than morphine, so faster analgesic effect. It can be given in many routes, and often seen used for palliative clients using the SQ butterfly administration.
Codeine
Codeine is a natural opioid that is used for moderate pain relief. It is often used in combination with acetaminophen or ibuprofen to provide a convenient non-opioid/opioid option. Besides pain relief, it has a unique use as a cough suppressant (anti-tussive) and the only opioid with this effect. It is not used with children less than 12 years due to the risk of respiratory depression and minimal cough suppression abilities. Codeine does have a ceiling effect which is different than the other opioid choices.
Methadone
Methadone is a synthetic opioid that is used for chronic pain management, opioid maintenance therapy or for neuropathic pain. The opioid dependent treatment is for maintenance or for detoxification. The principal goal is to relieve cravings, suppress abstinence syndrome and block the euphoric effects associated with opioids. it is given orally once a day by a clinic or pharmacy, and has a long duration of action of 24-36 hours. For clients with a cardiac history, there is a possible adverse effect of prolonging the QT interval and leading to torsade de pointe if left untreated. Clients that are a good candidate for methadone therapy and have a cardiac risk, a baseline ECG prior to starting methadone and then one month after is recommended. Methadone is for long term management and some clients are on methadone for months to years.
Tramadol
Tramadol is a dual mechanism of action analgesic. It has a weak agonist effect on the mu receptor, and also inhibits norepinephrine and serotonin reuptake in the pre-synaptic neurons. It is used for a wide variety of pain situations including neuropathic pain, post-operative pain, lower back pain, as well as pain associated with labour, osteoarthritis, fibromyalgia, and cancer. It is also used off-label for premature ejaculation and restless leg syndrome that are refractory to other medications. It is a relatively safe analgesic, with 1/10th the potency of morphine. Ie. Morphine 1 mg oral = Tramadol 10 mg oral. Benefits to tramadol include a low incidence of constipation, nausea and dizziness compared to other opioids as well as no hypotension or respiratory depression. It should be used with caution with clients with epilepsy or head trauma as it may cause seizures. Other cautions include avoid using with other CNS depressants, especially antidepressants with serotonin inhibition such as SSRIs or TCA’s. Tramadol does have a ceiling effect due to the risk of seizures at higher doses (Fraser Health, 2008).
Dosing and Routes of Administration
Depending on the opioid, it can be available in many formulations including oral, PR, IM, SQ, IV and transdermal.
Oral routes: it can also be available in immediate release (IR), sustained release (SR) or controlled release (CR). It is important for nurses to be alert for oral meds that are SR or CR, as the dose, frequency and duration of action will be different.
Example:
- Immediate release: t1/2 is 2-4 hours with duration of action 4-5 hours.
- Sustained release: duration of action is 8-12 hours.
Differences between immediate release, controlled release and sustained release:
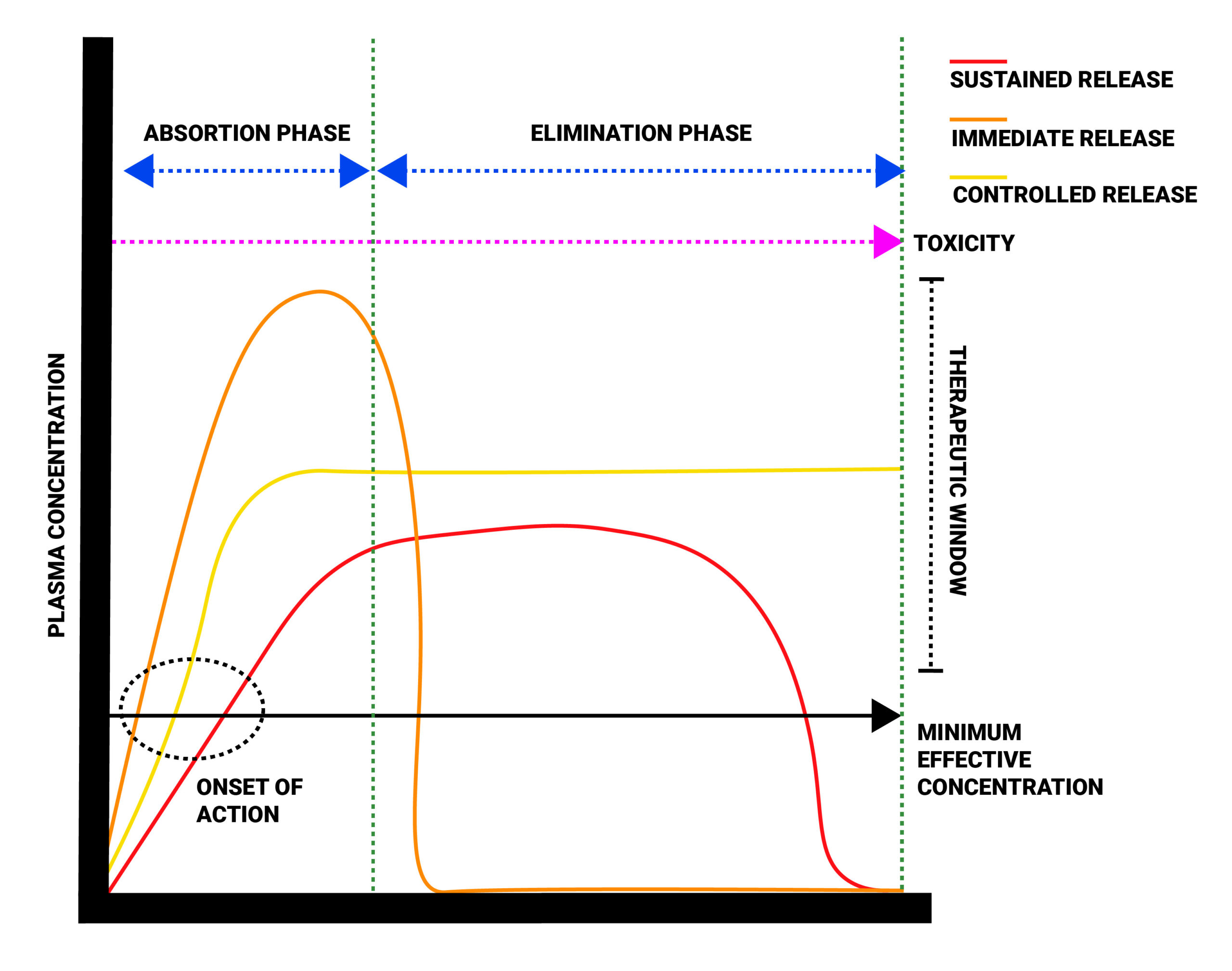
A client with complex or chronic pain issues will often be prescribed a SR or CR formula so they have consistent pain control.
| Generic/trade name | Route | Adult Dosage Formulation |
| morphine
MS Contin, Statex, M.O.S. |
PO & Rectal
SQ, IM, & IV
Immed. release, extended release, sustained release |
Oral: 5, 10, 30 mg IR tab
12 hr and 24 hr SR formulations
Rectal: 5-30 mg PR IV: 2mg/ml – 50 mg/ml Relative potency: 10 mg IV = 30 mg po |
| fentanyl
Duragesic, abstral |
Transdermal
IM IV |
Oral: 100-800 mcg tabs
12 mcg-100mcg patch IV: 50 mcq/ml
Relative potency: 100x more potent than Morphine |
| hydromorphone
Dilaudid |
PO
Rectal SQ, IM & IV |
Oral: 1-8 mg
SR: 12 and 24 hr formulations PR: 3 mg IV/SQ/IM: 2- 50 mg/ml |
| oxycodone
Oxycontin Percocet |
PO | Oral: 5 mg-20 mg IR
5-80 mg SR No IV or supp Percocet: 5 mg/325 mg |
Combination Formulations: opioids are often combined with a non-opioid medication such as acetaminophen or ibuprofen. This gives the added benefit addressing the pain utilizing different pain pathways and using less opioids that can cause dependency and more adverse effects.
Tylenol #3: Acetaminophen 325-650 mg + codeine phosphate 30 mg + caffeine 15 mg
Drug manufacturers also make Tylenol #2 (acetaminophen 300 mg, codeine phosphate 15 mg, caffeine 15 mg) as an option for those clients needing less pain control such as for dental procedures or from minor injuries.
Did you know… the purpose of caffeine is to improve the absorption of codeine and acetaminophen.
Safety Considerations with Opioids: potency matters
It is important to consider that the type of opioid and their route have different effects on the client. How potent the opioid is will have an effect on the dose we give. For instance, hydromorphone is five times more potent than morphine. Fentanyl is 80-100 times more potent than morphine (UptoDate, 2021). What does this mean in practice? Nurses need to pay attention to the dose to avoid under or over medicating a client.
- Morphine is given in milligrams(mg). The typical dose would be 2-5 mg IV.
- Fentanyl is given in micrograms (mcg). The typical dose would be 50-100 mcg IV. In comparison to morphine, it is 100x more potent.
- Hydromorphone is also given in mg. A dose may be 1.5 mg IV. In comparison to morphine, it is 5 times more potent.
Side/Adverse Effects
Most clients will experience some side effects from taking an opioid. Mild effects can include dizziness, sedation, nausea, and constipation. The most serious effect is respiration depression. Nurses play an important tole in minimizing these effects. To begin, nurses need to anticipate that adverse effects will occur, completing a thorough assessment before and after administration, close monitoring, and being proactive with interventions.
Adverse effects of Opioids
Many unwanted effects of opioid meds are due to the activation of receptors in other parts of the body. The following table lists adverse effects, physiological causes and nursing considerations.
| Adverse effects: | Cause | Nursing considerations |
| Pruritis | Due to histamine release.
More with epidurally administered opioids |
Give Antihistamine prn
(mostly with non-synthetic opioids, morphine or codeine) |
| Constipation
|
Due to slowed peristalsis and relaxation of smooth muscle and inhibiting secretions of fluids into the intestinal lumen when opioids bind to opioid receptors in the bowel. | Strategies to manage constipation:
Assess GI system, especially LBM. Give Laxative/stool softener/fiber – Encourage hydrate/mobilize/bowel routine |
| Nausea & Vomiting
|
Increased sensitivity of the vestibular system and stimulation of the chemoreceptor trigger zone in the medulla.
Note: N&V associated with opioid administration lessens with subsequent doses. |
Anti-emetic prn. Anticipate nausea, can give anti-emetic prophylactically
Post op – often ondansetron. Dimenhydrinate often prescribed. |
| Respiratory depression | Decreased sensitivity of respiratory centers in the brain to CO2 when opioids bind to areas in the medulla.
This is compounded with concurrent use of other CNS depressants (alcohol, barbiturates, benzodiazepines) |
Most serious of SE. Can last 4-5 hours
ALWAYS assess RR/depth pre/post opioid Anticipate issues Fentanyl highly apenogenic |
| CNS | drowsiness, sedation, euphoria via activation of different receptors
dysphoria activation of Mu receptors |
Altered LOC – safety concern … assess dizziness, stuporous
Caution with head injury (can mask neuro changes) Codeine causes least CNS changes |
| Urinary retention / hesitancy | due to increased tone of bladder sphincter | Assess in/outs. Palpate bladder, bladder scan post-void
Promote voiding – void q 4hr, measure ↑concern with BPH or if also on anti-cholinergic meds. |
| Cough suppression (anti tussive) | Often codeine is given because of this side effect.
Only analgesic with anti-tussive properties. Codeine is often an ingredient in prescription cough medicines. |
Caution/avoid with peds d/t respiratory depression. |
| Increased ICP | By suppressing respirations, CO2concentrations of the blood ↑, this causes vasodilation of cerebral vessels causing ICP to ↑ | Caution with head injury (mask neuro changes). Keep RR within normal range |
| Hypotension | Blunt baroreceptors reflex and vasodilation resulting in ↓SVR. Release of histamine – causes peripheral vasodilation→ orthostatic hypotension. | Assess BP pre/post analgesic
Assess for orthostatic hypotension Teach client about lightheadedness, dizzy. Fall risk caution |
High Alert Med: The risk of serious adverse reactions, including slowed or difficulty breathing and death, have been reported with the combined effects of morphine with other CNS depressants. Long-term usage of morphine may result in drug tolerance, dependence, and/or misuse. Naloxone is used to reverse opioid overdose.
Respiratory Depression
Respiratory depression is the primary risk of opioids. Respiratory depression occurs more frequently in the elderly or those suffering from conditions accompanied by hypoxia, hypercapnia, or upper airway obstruction, for whom even moderate therapeutic doses may significantly decrease pulmonary ventilation.
Use morphine with extreme caution in clients with chronic obstructive pulmonary disease or cor pulmonale and in clients having a substantially decreased respiratory reserve, hypoxia, hypercapnia, or pre-existing respiratory depression. In such clients, even usual therapeutic doses of morphine sulfate may increase airway resistance and decrease respiratory drive to the point of apnea. Consider alternative non-opioid analgesics, and use morphine sulfate or other opioids only under careful medical supervision at the lowest effective dose in such patients.
Use In Head Injury and Increased Intracranial Pressure
In the presence of head injury, intracranial lesions, or a preexisting increase in intracranial pressure, the possible respiratory depressant effects of morphine and its potential to elevate cerebrospinal fluid pressure may be markedly exaggerated. Furthermore, morphine can produce effects on pupillary response and consciousness, which may obscure neurologic signs of increased intracranial pressure in clients with head injuries.
Hypotensive Effect
Morphine may cause severe hypotension in individuals unable to maintain blood pressure who have already been compromised by a depleted blood volume or drug administration of phenothiazines or general anesthetics. Administer morphine sulfate with caution to clients in circulatory shock, as vasodilation produced by the drug may further reduce cardiac output and blood pressure. Blood pressure is always taken as part of the pre-opioid assessment, then at least 15 minutes after administration, along with pain assessment, heart rate and respiratory status.
Gastrointestinal Effects
Do not administer morphine to clients with gastrointestinal obstruction, especially paralytic ileus because opioids diminish propulsive peristaltic waves in the gastrointestinal tract and may prolong the obstruction. The administration of morphine sulfate may obscure the diagnosis or clinical course in clients with an acute abdominal condition.
Use in Pancreatic/Biliary Tract Disease
Use opioids with caution in clients with biliary tract disease, including acute pancreatitis, as morphine sulfate may cause spasming and diminished biliary and pancreatic secretions.
Nursing Considerations
Opioids can be used for all ages. It should be used cautiously with:
- Pregnancy: Some clients with opioid dependency or with medical conditions that require pain management (myalgia, joint pain), require opioids during pregnancy. It is not well understood all the harms opioids may cause to the fetus due to lack of research for ethical reasons. There have been a few large studies that suggest opioid use during pregnancy has been associated with birth defects such as congenital heart defects and neural tube defects. There does not appear to be evidence of low birth weight as previously determined (Yazdy, Desia & Brogly,2015). Some opiates also appear to have less adverse effect on the fetus than others. For clients who are taking opiates at the time of delivery, the newborn is at risk for neonatal opioid withdrawal syndrome (NOWS). These newborns experience withdrawal symptoms and often need supportive care until stable. For clients who need to be on opiates while pregnant, oversight by a physician is needed to weigh the benefits vs risk of both the mother and fetus.
- Breastfeeding: Opioids are found in breastmilk. If opioid use is required, the smallest dose for the shortest time is advised. Some opioids appear to have more effect such as codeine and tramadol, but all opioids can potentially cause adverse effects of sedation, poor feeding and respiratory depression. It is advised to limit opioid use to 2-3 days post-partum and under health care provider monitoring (Ito, 2018).
- Clients with liver and renal impairment: For clients with renal impairment, a lower dose adjustment is required. As opiates are metabolized in the liver, and can be prescribed with liver disease but in lower doses and close monitoring.
- Older adult: Due to pharmacodynamic changes that occur with aging, the older adult is more susceptible to the adverse effects of opiates, which can increase negative effects on the central nervous system, cardiovascular system, and gastrointestinal system. For example, due to the sedative effects, the risk of falls is high so ensure precautions are in place.
- Other health conditions that require caution, closer monitoring and lower dosages:
- Addison’s disease, hypothyroidism
- prostatic hypertrophy, or urethral stricture
- CNS depression, toxic psychosis
- acute alcoholism, and delirium tremens
- may aggravate convulsions in clients with convulsive disorders
- may induce or aggravate seizures.
Neonatal Opioid Withdrawal Syndrome
Newborns that have been exposed to opioids in utero have a higher risk of health issues post delivery. Neonatal Opioid Withdrawal Syndrome or Neonatal Abstinence Syndrome is a combination of gastrointestinal, respiratory, autonomic and central nervous system disturbances that affect postnatal life adaptation in critical areas of sleep, feeding and autonomic function. Neonates with severe NOW symptoms require prolonged hospitalization and pharmacotherapy, with unknown long-term effects (Yazdy, Desia & Brogly, 2015).
Client Assessment for IV Opioid Administration:
A nurse is preparing to give a client Morphine IV following a pain assessment. The client has 7/10 sharp pain to the right abdominal area, non-radiating, increases with movement. Before the nurse administers the morphine, what else should be assessed?
Always assess vital signs prior to giving an analgesic and especially parenteral route due to the faster onset of action.
- Blood pressure, heart rate (due to hypotensive effects of opioids)
- Respiratory rate and oxygen saturations (due to the risk of respiratory depression)
Once the dose has been given, stay with the client for the first 5 minutes and reassess pain, RR and oxygen sats, as well as BP and HR, particularly if first time dose.
In 15 minutes, reassess pain level and vital signs. The nurse will be anticipating a slight drop in BP and respiratory rate. For some clients, they have a more profound effect and a significant drop in BP or RR occurs. Ensure not to administer the opioid faster than the drug monograph advises, due to a risk a hypotension.
Client Education
It is important to provide accurate information to clients about how to safely use opiates. This is especially true if clients are opiate naive. Additionally, clients might be worried about becoming addicted to opioids even with short-term usage. You can teach your client that most patients who use opioids do not become addicted, but advise using the opioid as directed and for the shortest period of time.
- Do not use alcohol or other CNS depressants: Morphine has addictive effects when used in conjunction with alcohol, other opioids, or illicit drugs that cause central nervous system depression because respiratory depression, hypotension, profound sedation, coma, or death may result. Avoid the use of other opiates, phenothiazines, and sedative/hypnotics and antidepressants.
- Ensure to store in a safe place away from children or pets.
- Driving and Operating Machinery: Opioids can impair the mental and/or physical abilities needed to perform potentially hazardous activities such as driving a car or operating machinery.
- Advise clients about using short-term opiates versus long-term opiates so they know the differences in dose and scheduling.
- Fentanyl Transdermal patch: If using a fentanyl transdermal patch, the client needs specific instructions to ensure safe use. This includes:
- Never apply heat to the patch or surrounding area.
- Never cut or tamper with the patch.
- Use gloves when applying to a clean, hairless area.
- Do not abruptly stop using the patch, consult prescriber.
- Anticipate adverse effects:
- Constipation: advise to start a laxative such as sennakot when starting to take opiate at home. Monitor bowel movements, and if loose stools, use laxatives less often. Ensure client drinks more water and increases fiber intake.
- Sedation and dizziness: opiates are sedating and can lower BP; so do not undertake any activity that can increase risk of falls without precautions in place.
- Nausea: Many opiates will cause some nausea; this will subside over time. Take an anti-nausea medication to minimize the nausea.
- Instruct client to monitor for symptoms of an allergic reaction such as shortness of breath, tight feeling in the throat, hives, nausea or vomiting.

Critical Thinking Out Loud
40-year-old client is admitted to the hospital following a motor vehicle incident. They have multiple injuries that require constant pain relief to give them a manageable level of pain control. Their underlying pain score is 4/10, with pain 8/10 when the physiotherapist completes the therapy sessions. The order might read:
- Hydromorphone po q 4-6 hours PRN
- Morphine 2-5 mg IV q 1 hour PRN for breakthrough pain.
- Acetaminophen 325-650 mg po q 4 hours.
Following an assessment of their pain, the nurse will give the acetaminophen regularly as ordered. They should also give hydromorphone on a regular basis, so the client has sustained pain relief. For the physiotherapy sessions, giving the client Morphine IV prior to the session so they are more comfortable. How much Morphine to give? Factors to consider are: is the client opioid naive? When was the last morphine dose? How much morphine have they been given before and was it effective? What side effects occurred and is it safe to give another dose? Good effective analgesia is an individualized approach.
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 6: Pain and Mobility Medications Answer Key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
Safety Considerations for Opioid Use
The Opioid Crisis in Canada
Almost 25% of Canadians experience chronic pain and opioids have been commonly used for chronic pain management. Opioid prescriptions are also used for treating opioid dependence. However, there is debate about the effectiveness of treating chronic non-cancer pain with opioids based on concerns related to the safe usage of these medications.
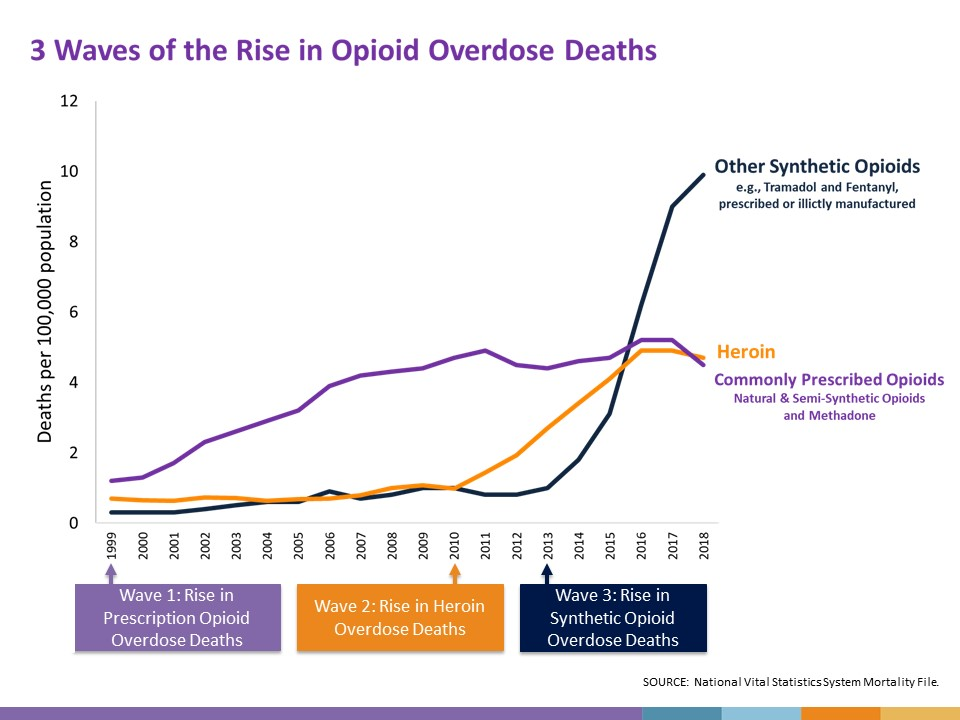
The past 30 years have seen waves of opioid-related deaths starting in the 1990s when overdose deaths were linked to a dramatic increase in prescription opioids for chronic pain. The wave increased again in 2010 when overdose deaths were more commonly related to illicit drug use.[4] Currently, most of the harm related to opioid use is due to the synthetic opioid, fentanyl, which is extremely potent and significantly increases the risk of overdose even in trace amounts. Figure 10.7a depicts the waves of opioid-related deaths in the United States, which closely mirrors the trend in Canada (CDC, 2016).
From 2016 to 2019, there were more than 14,700 opioid-related deaths in Canada (Government of Canada, 2021). In 2016 in British Columbia, the provincial health officer declared a public health emergency under the Public Health Act due to the rise in opioid-related overdose deaths (Government of Canada, 2021).
In response to the public health emergency, the College of Physicians and Surgeons of British Columbia developed Professional Standards and Guidelines: Safe Prescribing of Drugs with Potential for Misuse/Diversion, based on the 2016 CDC Guideline for Prescribing Opioids for Chronic Pain (CDC, 2016). Improving the prescription of opioids through clinical practice guidelines is intended to ensure clients have access to safer, effective pain treatment while also reducing the number of people who misuse or overdose from these drugs. In light of the overdose crises, is important for nurses to provide safe and equitable care for clients experiencing pain.
To learn more about substance use, refer to the British Columbia Center on Substance Use and the Canadian Center on Substance Use and Addiction.
Opioid Analgesic Medication Card
Now let’s take a closer look at the medication card for opioid analgesics (Rosenjack Burchum & Rosenthal, 2016;Vallerand & Sanoski, 2019). Medication cards like this are intended to assist students to learn key points about each medication. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication. Basic information related to each class of medication is outlined below.

Downloadable file (.docx): Opioid Analgesic Medication Card
Clinical Reasoning and Decision-Making Activity 1
A client with metastatic lung cancer is experiencing 6/10 rib pain. The nurse completes their assessment and plans to give the regularly scheduled oral morphine for pain relief.
- What should be included in the assessment prior to giving the analgesic?
- When should the effectiveness of the medication be evaluated?
- What adverse effects would the nurse want to assess for that may put the client at risk?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 6: Pain and Mobility Medications Answer Key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
Opioid Antagonists
Naloxone
Naloxone is a reversal agent used to mitigate risk for opioid-induced respiratory depression by displacing the full opioid agonists. It is safe medication and used to temporarily reduce the effects of overdose from opioids leading to life saving measures of improved breathing. It is only effective if someone has opioids in their system.
Mechanism of Action
Naloxone is an antagonist opioid medication that has a high affinity for μ-opioid receptors, rapidly displacing opioids bound to these receptors. This leads to a reversal of effects — particularly respiratory depression, sedation, and euphoria, but also reverses analgesia. It does not produce opioid-like effects and has no abuse potential.
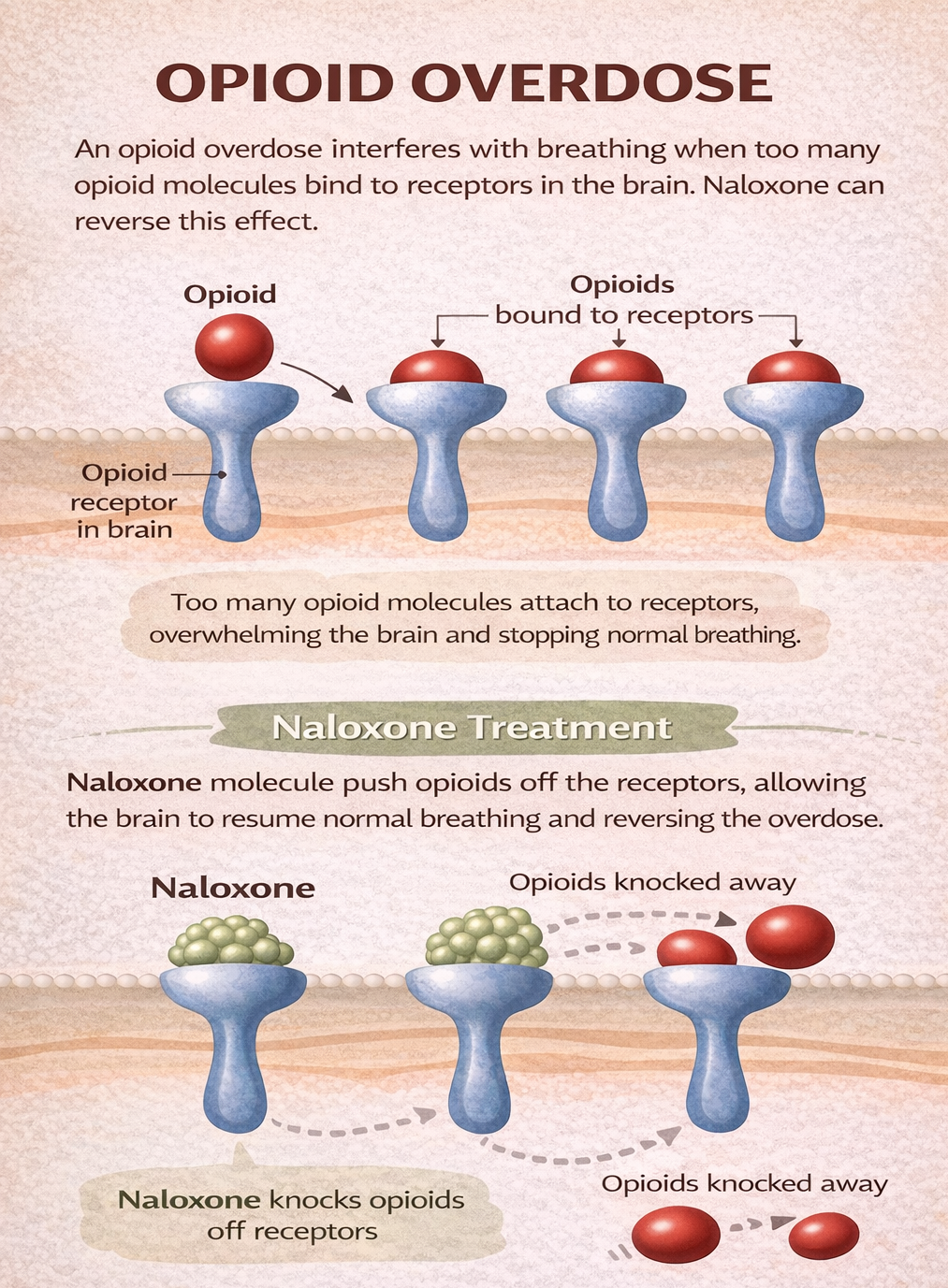
Figure 6.6e Opioid overdose. The action of naloxone in reversing the effects of opioid medications. Naloxone has a high affinity for the mu receptors, and in the presence of an opioid, will bind to available receptors as well as bump off opioid medications. This effect leads to an immediate effect of reversing respiratory depression. (Sheila O./TRU Open Press adapted from harmreduction.org)
Indications for Use
Naloxone is indicated for the complete or partial reversal of opioid depression, including respiratory depression induced by natural and synthetic opioids. It is used as a life-saving measure in the community and hospital settings.
When opioids are taken in large quantities they can cause life-threatening symptoms such as respiratory depression, bradycardia, hypotension along with slurred speech, drowsiness and constricted pupils (Adams et al, 2019). If untreated, symptoms can progress to vomiting, absent pulse and breathing, loss of consciousness and death. Naloxone will rapidly reverse these symptoms of central nervous system depression (Drugbank, 2025). Due to its relatively short duration of action of 30-60 minutes, repeated doses of naloxone are often required. Some people need more than one dose of naloxone at a time if the first dose is ineffective.
Naloxone is available in subcutaneous, intramuscular, nasal spray or intravenous routes. In the community, kits can be obtained with IM injections or nasal spray along with all the other supplies needed to treat an overdose. Obtaining a naloxone kit is relatively easy from pharmacies or mental health clinics with minimal training. First responders all carry naloxone as a first line overdose treatment plan.
Dosage:
- IM or IV: 0.4 mg
- IV infusion: 0.2- 0.4 mg/hr
Watch the following video on how to use naloxone: How to Use a Naloxone Kit on Someone Who Overdosed [1:36] by CBC News (2022) on YouTube.
Nursing Considerations
Assess:
- Respiratory rate less than 10 breaths per min.
- Other: bradycardia, drowsiness or decreased level of consciousness, hypotension, pupil constriction
Administer:
- IM: onset of action is 3-5 minutes, with t1/2 life 60-90 minutes. Since naloxone rapidly reverses opioid effects, the client will immediately experience withdrawal symptoms and no pain relief (Adams et al, 2019).
- Clients who arrive in emergency after receiving naloxone in the community need close monitoring as the effects of Naloxone wear off. The effects of naloxone are about 30-60 minutes, so depending on the amount of opioid they used, they may begin to show signs of overdose again with respiratory depression, slow heart rate and drowsiness.
- Anticipate the need for repeated doses of naloxone, often IV push and sometimes IV infusion depending on how the client is doing.
- Naloxone is widely distributed and crosses the blood brain barrier and placenta.
- Children: Naloxone can be given to children over the age of 12, the safety and effectiveness of naloxone have not been established in younger children. Naloxone is contraindicated for pregnant and lactating women.
Monitor:
- After naloxone is given, assess every 3-5 minutes: sedation score, blood pressure and heart rate, respiratory assessment including respiratory rate and oxygen saturations. Airway management and IV fluids are often part of the treatment plan (Drugbank, 2025). Additional assessment may include ECG.
Adverse/Side Effects
- Adverse effects include tremors, drowsiness, sweating, decreased respirations, hypertension, nausea, and vomiting.
- Clients may also experience acute narcotic abstinence syndrome or withdrawal symptoms for those who are opioid dependent.
- Neonates: opioid withdrawal may also include convulsions, excessive crying, and hyperactive reflexes.
- Naloxone reverses an opioid that was indicated for pain, the pain may return.
- Abrupt reversal of opioid depression or excessive dosages of naloxone is not without risk. Abrupt reversal can lead to ventricular tachycardia or fibrillation, pulmonary edema, coma, encephalopathy and cardiac arrest.
Opioid withdrawal symptoms can be mild to severe and all clients require close monitoring.
- Increased thirst, chills, fever, muscle pain
- CNS: drowsiness, stimulation, confusion, headache, seizures
- GI: nausea, vomiting, diarrhea
- CVS/Resp: tachycardia, tachypnea, hypertension, wheezing, pulmonary edema
Once in an acute care setting, the Clinical Opiate Withdrawal Scale (COWS) will likely be implemented. Go to the link to learn more about COWS. Emergency Care BC: Clinical Opiate Withdrawal Scale—Treatment : Emergency Care BC
Client Teaching
Clients should be advised regarding the risks associated with opioid analgesic use. Clients and their families should be provided information about how to use opioid antagonists. Refer to the College of Pharmacists of BC for information on naloxone and how to use in an overdose: BC Pharmacists. Clients can obtain a naloxone kit free of charge from many mental health clinics or pharmacists.

Downloadable file (.docx): Naloxone Medication Card
Clinical Reasoning and Decision-Making Activity 2
A post-operative client just received naloxone for respiratory depression. When should the client’s respiratory status be reassessed?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 6: Pain and Mobility Medications Answer Key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
Image Description
Figure 6.6d Three Waves of Opioid Overdose Deaths
A line graph that depicts deaths per 100,000 population due to different types of opioids between 1999 and 2018.
- Commonly prescribed opioids (natural and semi-synthetic opiods and methadone): From 1999 to 2011, the death rate per 100,000 population steadily rises from 1 to 5. There is a slight dip after that but it rises again by 2016.
- Heroin: From 1999 to 2010, the death rate per 100,000 remains quite steady at around 1. From 2010 to 2016, the death rate rises steadily to just under 5 per 100,000., then it levels out.
- Other synthetic opioids (e.g., Tramadol and Fentanyl, prescribed or illicitly manufactured): From 1999 to 2013, the death rate per 100,000 remains quite steady at around 1. From 2013 to 2018, the death rate rises steeply to 10 per 100,000.
Below the graph, three waves are identified:
- Wave 1: Rise in prescription opioid overdose deaths started in 1999.
- Wave 2: Rise in heroin overdose deaths started in 2010.
- Wave 3: Rise in synthetic opioid overdose deaths started in 2013.
[Return to Figure 6.6d]
Interactive Activities
References
Adams, M., Urban, C., El-Hussein, M., Osuji, J. & King, S. (2018). Pharmacology for Nurses. A pathophysiological approach (2nd Canadian ed.). Chapter 3: Pharmacokinetics. Pearson Canada Inc: Ontario.
Burchum, J., & Rosenthal, L. (2023). Lehne’s pharmacology for nursing care (11th ed.). Saunders
CBC News. (2022). How to use a naloxone kit on someone who overdosed [Video]. YouTube. https://www.youtube.com/watch?v=6cVMupA4aIs
Centers for Disease Control and Prevention [CDC]. (2018, December 19). Opioid Overdose, Understanding the Epidemic. https://www.cdc.gov/drugoverdose/epidemic/index.html. ↵
Centers for Disease Control and Prevention [CDC]. 3 Waves of the Rise of Opioid Overdose Deaths by National Vital Statistcs System, CDC is licensed under CC0. ↵
CDC. (2016). CDC Guideline for Prescribing Opioids for Chronic Pain. https://www.cdc.gov/mmwr/volumes/65/rr/rr6501e1.htm ↵
Doulton, B. (2014). Pharmacologic management of adult breakthrough cancer pain. Canadian Family Physician, Dec; 60(12):1111–1114.
Drug Bank (2025). Naloxone. Naloxone: Uses, Interactions, Mechanism of Action | DrugBank Online
Emergency Care BC (2025). Clinical Opiate Withdrawal Scale—Treatment : Emergency Care BC Provincial Health Services BC
Fraser Health (2008). Principles of Opioid Management. Hospice Palliative Care Program.
Fentanyl Patch Image: https://www.istockphoto.com/en/photo/fentanyl-patches-gm1454787354-490326416
Government of Canada. (2021). Opioid-related harms in Canada: Integrating Emergency Medical Service, hospitalization, and death data. https://www.canada.ca/en/health-canada/services/opioids/data-surveillance-research/integrating-emergency-medical-hospitalization-death-data.html
Government of British Columbia. (2020). Statistical Reports on Deaths in British Columbia. https://www2.gov.bc.ca/gov/content/life-events/death/coroners-service/statistical-reports ↵
Ito, S. (2018). Opioids in breast milk: pharmacokinetic principles and clinical implications. Journal of Clinical Pharmacology, 58(S10), S151-S163. https://doi.org/10.1002/jcph.1113
Kumar, R., Viswanath, O. & Saadabadi, A. (2024). Buprenorphine. National Library of Medicine. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK459126/
McCuistion, L., Vuljoin-DiMaggio, K., Winton, M, & Yeager, J. (2018). Pharmacology: A patient-centered nursing process approach. pp. 268-270, 324, 332. Elsevier.
Open Resources for Nursing (Open RN). (n.d.). 10.7 Opioid analgesics and antagonists. In Nursing pharmacology. BCcampus. https://opentextbc.ca/nursingpharmacology/chapter/10-7-opioid-analgesics-and-antagonists/
Patient Controlled Analgesia Image: https://commons.wikimedia.org/wiki/File:PCA-02.JPG
Rosenjack Burchum, J., & Rosenthal, L. (2023). Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
UptoDate. (2021). Dose conversion guide for commonly used opioids. https://www.uptodate.com/contents/image?imageKey=PALC/111216
Vallerand, A. & Sanoski, C. (2024). Davis’s Canadian drug guide for nurses (19th ed.). F.A. Davis Company: Canada
Yazdy, M., Desai, R., and Brogly, S. (2015, June). Prescription opioids in pregnancy and birth outcomes: a review of the literature. Journal of Pediatric Genetics, 4(2), 56-70. doi: 10.1055/s-0035-1556740 PMID: 26998394
Media Attributions
- Figure 6.6a Patient Controlled Pump ( CC BY-SA 3.0
- Figure 6.6b Differences between immediate release, controlled release and sustained release medications. (TRU Open Press)
- Figure 6.6c Fentanyl Patch by DanielTahar on Wikimedia Commons is used under a CC BY-SA 4.0 license.
- Figure 6.6d Three Waves of Opioid Overdose Deaths is from National Vital Statistics System, CDC, and is used under a CC0 public domain license. (Retrieved from https://opentextbc.ca/nursingpharmacology/chapter/10-7-opioid-analgesics-and-antagonists/)
- Figure 6.6e Opioid overdose, is by TRU Open Press, adapted from 1.3: Pharmacokinetics I shared under a CC BY-NC-SA 4.0 license and was authored, remixed, and/or curated by Carl Rosow, David Standaert, and Gary Strichartz (MIT OpenCourseWare)

{kind=link}
.jpg){kind=link}