4.15 Adrenergic Receptor Agonists (Catecholamines) V2
This unit will review the three primary adrenergic receptor agonists. We will start with a brief overview of the endogenous role in the body under stress and to maintain homeostasis. This is only a brief introduction to adrenergic agonists.
The autonomic nervous system is made up of the parasympathetic nervous system and the sympathetic nervous system. Together, they help maintain the homeostasis of the autonomic functions of the body.
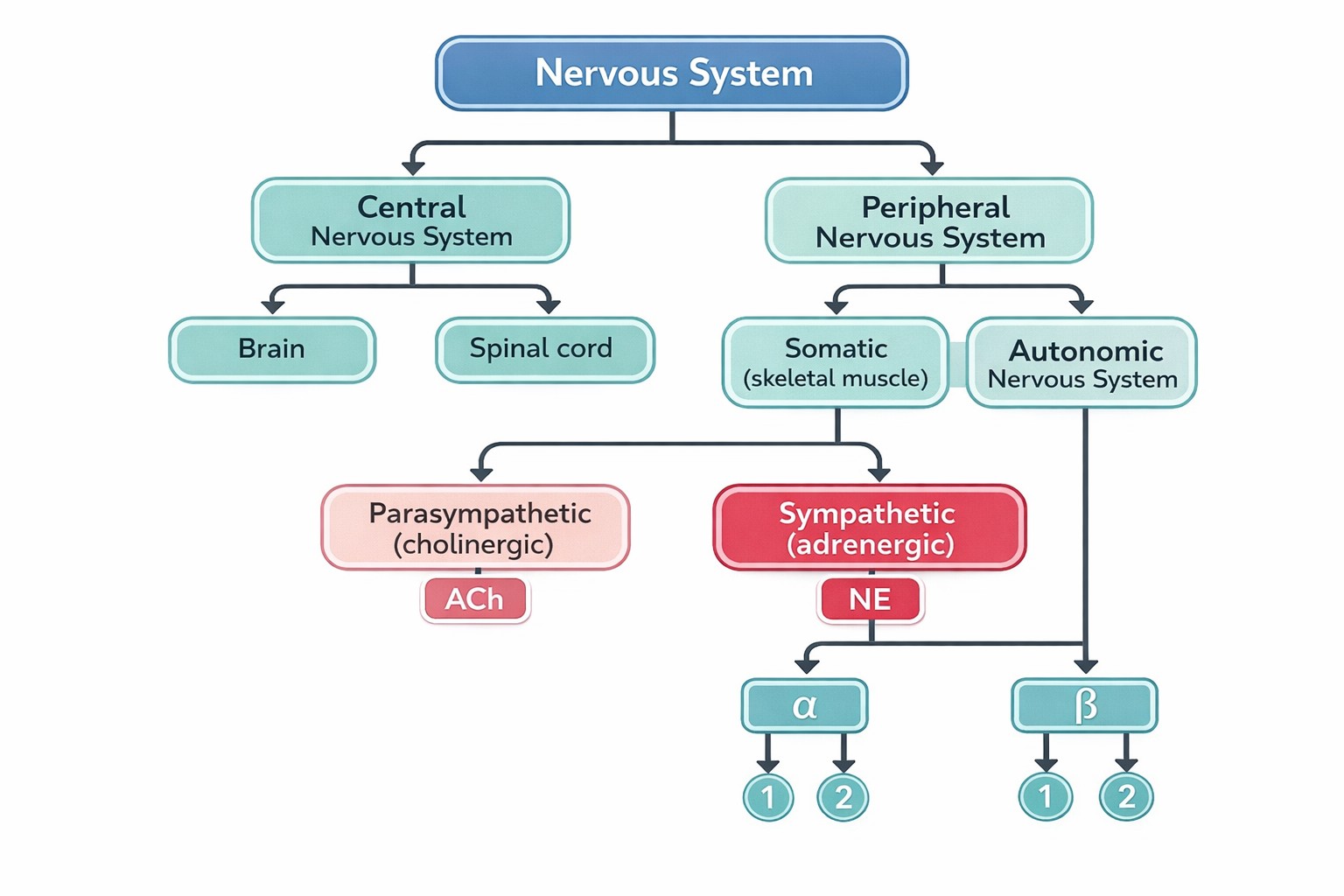
Figure 4.15a Nervous system (Sheila Obudote/ TRU Open Press)
Catecholamines are a group of similar hormones released into the bloodstream in response to physical or emotional stress. They act as neurotransmitters (NT) and hormones and regulate various physiological processes, including stress responses, cardiovascular function, and mood regulation. The primary catecholamines are dopamine, epinephrine (adrenaline) and norepinephrine (noradrenaline).
Norepinephrine and epinephrine, released by the sympathetic nervous system and adrenal medulla, have similar actions but are released under different circumstances. Epinephrine is responsible for the fight or flight response. Under stress, the body prepares for action by releasing epinephrine resulting in an increased heart rate, increased blood pressure, dilated bronchioles and increased blood glucose levels so the body has enhanced physical abilities, energy and alertness which would be vital for survival if a threat is upon us (Khalil, Rosani, & Warrington, 2024). Norepinephrine has similar actions but it helps maintain normal functioning such as increasing alertness and arousal, constricts blood vessels, pupil dilation and affects the sleep-wake cycle.
Dopamine is both a neurotransmitter and hormone and regulates many bodily functions. It regulates mood, motivation and reward, it is essential for motor control, influences gastrointestinal motility, and acts as a vasodilator mostly in the kidneys regulating blood flow and sodium excretion (Khalil, Rosani, & Warrington, 2024).
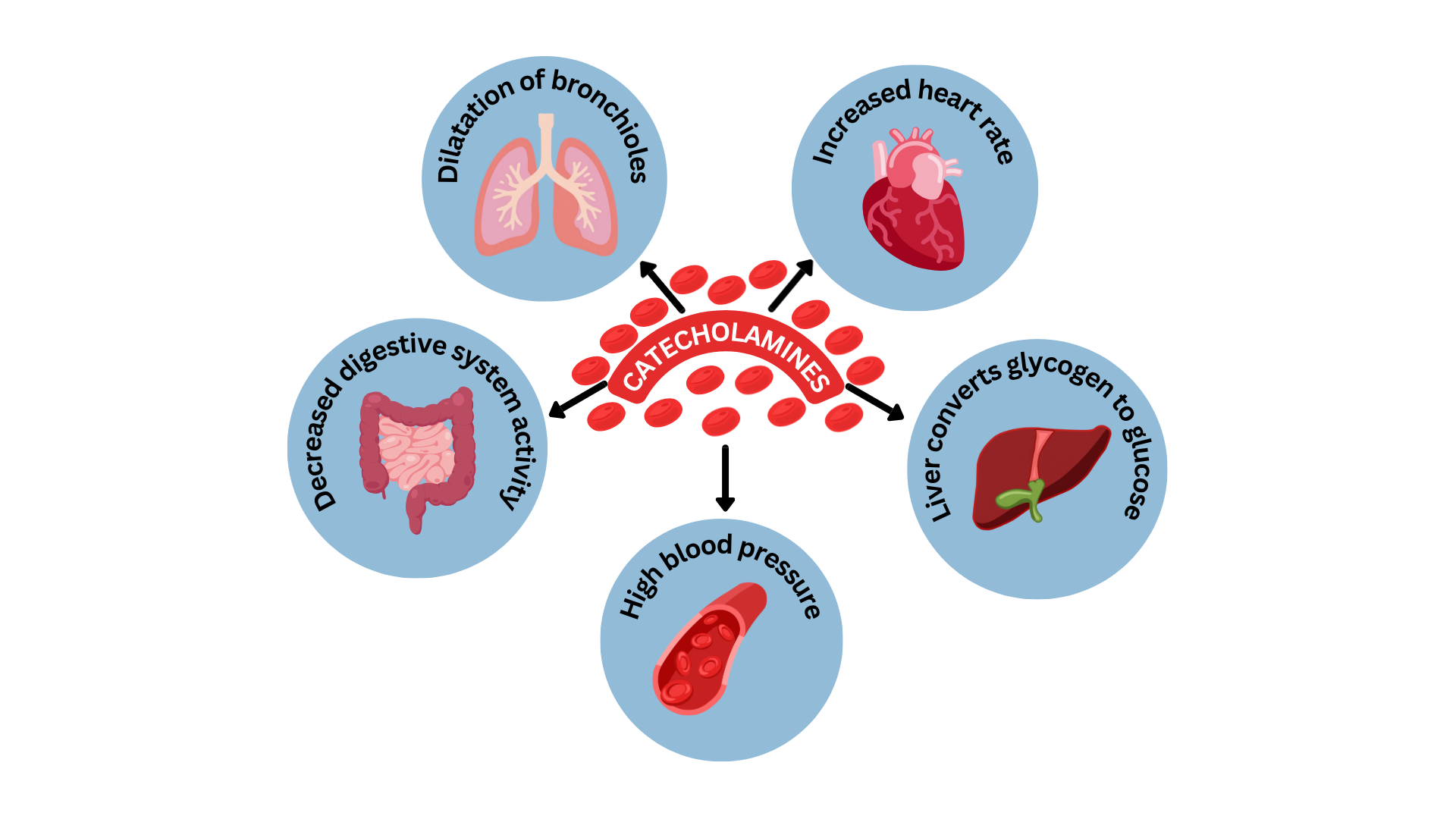
Figure 4.15b Physiological effects of catecholamines on major body systems. (TRU Open Press (2025)/Canva AI; modified from ) CC BY NC SA
Adrenergic Receptors: Adrenergic receptors are located throughout the body, and when activated, they produce a wide variety of physiological responses. In the diagram below, you can see how the activation of any of the four adrenergic receptors will result in different responses. When these receptors are stimulated or blocked, they provide a balance with physiological responses, for example between vasoconstriction or vasodilation.
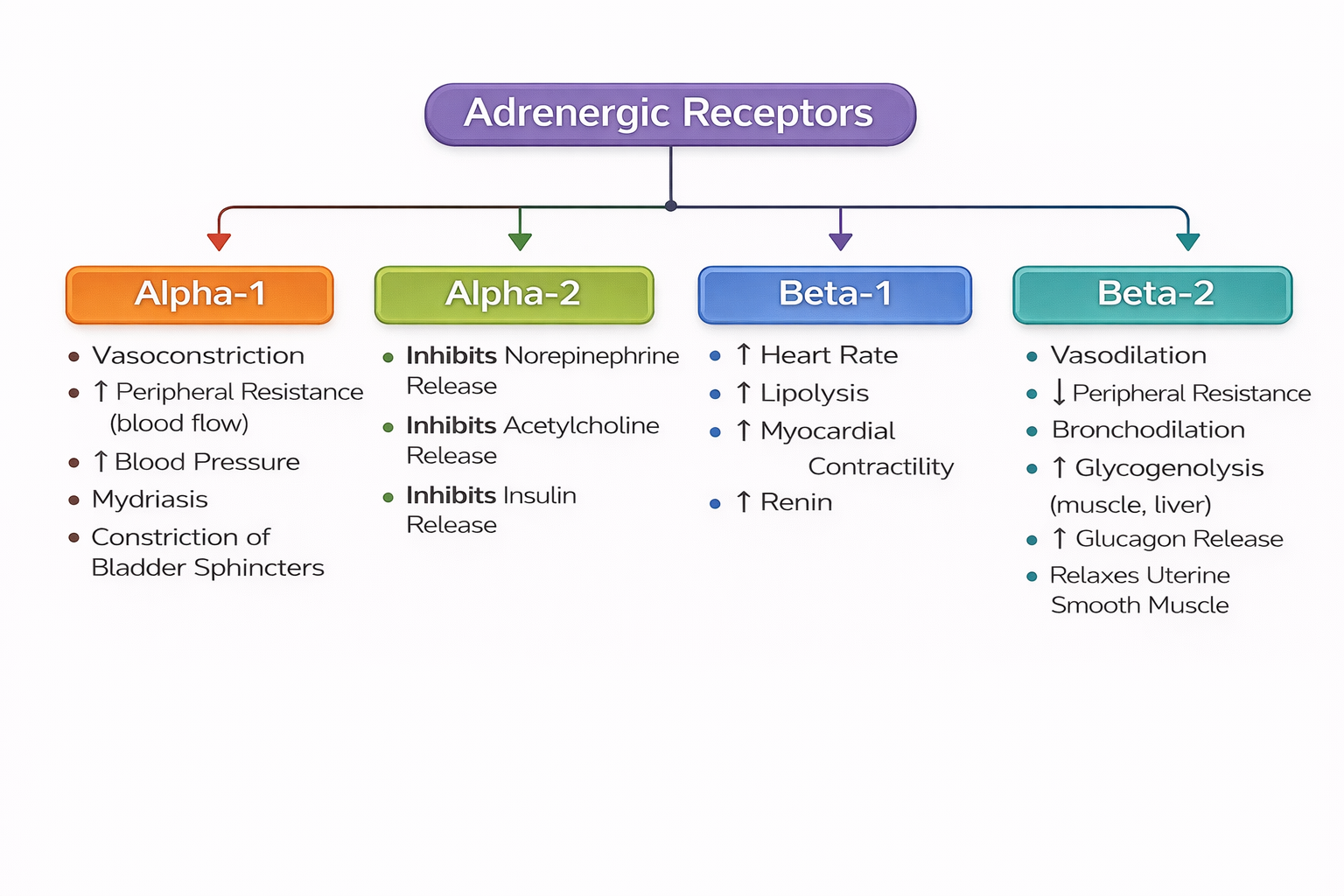
Figure 4.15c Adrenergic receptors (TRU Open Press/2025)
Watch the following video for a overview of the sympathetic nervous system: YouTube or Sympathetic Nervous System: Crash Course Anatomy & Physiology #14 – YouTube.]
When we think about adrenergic agonist medications, they have similar functions to endogenous catecholamines. When administered, they bath the synaptic cleft, activating the adrenergic receptor. Depending on the drug, they can activate the receptor directly, indirectly or a direct-indirect response. For example, epinephrine directly activates the adrenergic receptors. Amphetamines work indirectly by releasing the catecholamines from the vesicles within the synapse which then produces a response. Ephedrine does a mixed action, so it directly and indirectly releases the catecholamines to produce an effect (Rosenjack Burcham & Rosenthal, 2019). Recall that adrenergic antagonist medications, would block the receptor action, producing the opposite effect. For example, the beta-1 antagonistic action of Metoprolol would lead to a decrease in heart rate among other actions.
Catecholamines are often called sympathomimetics due to their effects on the sympathetic nervous system. This unit will only focus on epinephrine, norepinephrine and dopamine, but other adrenergic drugs exist. Adrenergic drugs are used for a wide variety of conditions. Depending on the receptors they activate and their affinity for certain tissues. Each adrenergic drug will be examined separately due to their specific effects on the body and their uses in practice.
Did you know?
Catecholamines are named for their chemical structure. Catechol group and an amine group. Due to their chemical structure, they cannot be taken orally, have a short half-life (so short duration of action) and cannot cross the blood brain barrier. What does this mean in a stressful situation? Endogenous epinephrine or norepinephrine are released due to a stress response, so the person can think quickly and have the energy and increased heart rate and BP to run away. But, once the stress is over, the neurotransmitters are quickly eliminated through the kidneys. They will also have minimal effect on the CNS as they don’t cross the BBB (Rosenjack Burcham & Rosenthal, 2019). In practice, we administer these drugs to increase the heart rate or increase the BP in situations such as sepsis. They are given parenterally and depending on the use, by infusion.
Epinephrine (Adrenalin)
Epinephrine, a sympathomimetic catecholamine, is a widely used medication to manage a variety of medical conditions due to its agonist effect on both alpha (α-1 and α-2) and beta (β-1 and β-2) receptors. It works both centrally and peripherally, thereby producing a range of sympathomimetic effects. The effects are dose dependent, with lower doses activating beta receptors enhancing bronchodilation and cardiac activity (increasing heart rate and improving cardiac output). At higher doses, epinephrine activates α-receptors to induce vasoconstriction and increase vascular tone (Dalal & Grujic, 2024). Other effects include increasing blood glucose levels by stimulating glycogenolysis and lipolysis. This catecholamine also dilates the airways to improve oxygen intake.
Indications for Use
Epinephrine is used to treat type 1 hypersensitivity reactions (including anaphylaxis), acute bronchospasm during asthma attacks, cardiac resuscitation (treatment for ventricular fibrillation, pulseless ventricular tachycardia, asystole, pulseless electrical activity), hypotension in severe shock, or for local injection to control superficial bleeding.
Mechanism of Action
Let’s take a look at how epinephrine exerts its effects, by reviewing how each receptor activation has a different function within the body.
- Alpha-1 adrenergic effects: vasoconstriction. Used for delaying absorption of local anesthetics, to control superficial bleeding and increase blood pressure.
- Alpha-2 adrenergic effects: inhibits the release of norepinephrine (which causes vasoconstriction) and increases vascular permeability. Alpha-2-receptors are also found on the pancreatic β-cells and when stimulated, insulin secretion is inhibited leading to elevated blood glucose levels.
- Beta-1 adrenergic effects: Beta-1 receptors are found mostly in the heart, and used in cardiac resuscitation to improve cardiac output, stroke volume and heart rate.
- Beta-2 adrenergic effects: Beta-2 receptors are located in the lungs, skeletal muscle and blood vessels, leading to bronchial smooth muscle relaxation and helps alleviate bronchospasm, wheezing, and dyspnea that may occur during anaphylaxis. It is also used for asthma and bronchitis (Khalil, Rosani, & Warrington, 2024; Rosenjack Burcham & Rosenthal, 2019).
Pharmacokinetics
Epinephrine is not given orally due to the rapid inactivation by two enzymes (monoamine oxidase and catechol-O-methyltransferase) in the liver before the drug can reach systemic circulation.
It is administered parenterally (intravenously (IV), subcutaneously, intramuscularly) and inhalation. If IV, it can be given IV push or by infusion depending on the rationale. Following IV administration, it is rapidly absorbed into the bloodstream and distributed throughout the body. Its half-life is very short, less than 5 minutes, so if given IV push, repeated doses are required every 3-5 minutes. It is eliminated through metabolic pathways with the liver having a primary role in clearing epinephrine from the bloodstream and from the body. Elimination, to a lesser extent, comes from the kidneys, skeletal muscles and mesenteric organs (Dalal & Grujic, 2024).
Nursing Considerations
Administration: parenteral (IV, SQ, IM) and inhalation.
Dosing and route will depend on the medical condition. For example:
- Anaphylaxis: epinephrine 0.3-0.5 mg IM or SQ into the anterolateral aspect of the thigh every 5 to 10 minutes as needed. Do not exceed 0.5 mg.
Autoinjector (Epipen): concentrations vary.
- Anaphylactic shock: IV in a 0.1 mg/mL solution or via IV infusion of 5 to 15 mcg/min, with adjustments based on clinical response. Intraosseous can be used if IV access is not available. Onset of action less than 2 minutes for IV route with duration of action up to 30 minutes. Intranasal epinephrine 2 mg spray if IV access is not readily available. Intranasal spray with a single 2 mg spray can also be used (Dalal & Grujic, 2024).
- Cardiac resuscitation:for cardiac arrest due to asystole, ventricular fibrillation, pulseless electrical activity, or pulseless ventricular tachycardia, Epinephrine (1:10,000)1 mg IV or IO q 3-5 minutes. If no IV or IO access, inhaled dose through endotracheal tube until IV access established.
High alert med: Epinephrine is available in different concentrations and strengths. Always check the orders carefully and have a second verifier to check concentration, dosage, route and infusion pump settings (Vallerand & Sanoski, 2021). Consult a pharmacist or product monograph.
- Extravasation risk: due to the vasoconstrictive action, the administration of epinephrine should be closely monitored to prevent extravasation into surrounding tissues, as it may result in local tissue necrosis and other complications. It is contraindicated for use in fingers, toes, ears, nose, or genitalia when used with local anesthetic due to the vasoconstrictive action.
- Contraindicated in clients with narrow-angle glaucoma.
- Administer with caution to the elderly and those with pre-existing cardiovascular disease.
- When administering IV, monitor vitals (blood pressure, heart rate and respiratory rate) and cardiovascular and respiratory systems closely; if blood pressure increases sharply, give rapid-acting vasodilators. Monitor IV site for extravasation. Discard IV solution if discoloured.
- Renal impairment: epinephrine can constrict renal blood vessels and decrease urine output. Close monitoring for clients with renal disease.
- If used for bronchodilation, assess respiratory status pre and post dosages. Assess for paradoxical bronchospasm.
- Pediatric Clients: For infants and pediatric clients, dosages will be adjusted.
- Pregnancy: in the case of anaphylaxis or cardiac arrest, the use of epinephrine may be needed. Due to its effect on β2-adrenergic receptors, which causes tocolysis, epinephrine opposes oxytocin’s actions on the uterus and may delay labor. It may also cause anaphylaxis-induced hypotension in pregnancy, as it may cause uterine vasoconstriction, reducing oxygen delivery to the fetus (Dalal & Grujic, 2024; Rosenjack Burchum & Rosenthal, 2019).
Adverse/Side Effects
Depending on the dose, alpha or beta receptors are activated, potentially producing different adverse effects.
- Hypertensive crisis:
- excessive alpha-1 activation can lead to a dramatic increase in blood pressure. Cerebral hemorrhage could occur. Monitor blood pressure and heart rate closely.
- Dysrhythmias:
- overstimulation of beta-1 receptors in the heart can lead to dysrhythmias or tachycardia. Obtain a baseline ECG and ongoing ECG monitoring for changes.
- Bronchospasm:
- rebound bronchospasm can occur with more than three inhaled dosages. Monitor respiratory status pre and post administration.
- Hyperglycemia:
- activation of beta-2 receptors in the liver and skeletal muscle can cause the breakdown of glycogen, leading to hyperglycemia in diabetic clients. Monitor blood glucose more closely and anti-diabetic meds may need to be adjusted. For non-diabetic clients, the pancreas will release more insulin to maintain normal blood glucose readings.
- Tremors:
- Due to beta-2 stimulation of the skeletal muscles, tremors is a common side effect. Tremors will decrease over time. Start with low doses to minimize the effect.
(Rosenjack Burchum & Rosenthal, 2019; Dalal & Grujic, 2024; Vallerand & Sanoski, 2021).
Example in Practice
A hospitalized client has been found unresponsive. He is pulseless and CPR is initiated. A code blue is called. The ECG shows pulseless ventricular tachycardia. Following the cardiac arrest protocol, defibrillation is provided, with continual CPR and other measures such as airway management. Epinephrine (1:10,000) 1 mg IV/IO every 3-5 minutes is ordered. Give over one minute, followed by saline flush. Epinephrine is given to increase blood pressure and stimulate heart function.
Client Teaching
For asthma or bronchodilation purposes – inhalation:
- Use correct administration technique
- Rinse mouth after treatment with warm water
- Maintain adequate hydration to avoid thick secretions.
- Notify health care provider if pregnant
For anaphylactic reactions – EpiPen use:
- Epinephrine formulated in a pen for injection is known as EpiPen. EpiPen is used for severe allergic reactions after exposure to an allergen like a bee sting. It will increase blood pressure, suppress glottal edema and counteract bronchoconstriction.
- Teach client correct EpiPen technique and usage.
- Check expiration date, store at room temperature, and protect from light.
- Effects fade after 15-20 minutes, so seek medical care immediately.
Epinephrine Medication Card
Now let’s take a closer look at the medication card for epinephrine (UptoDate, 2025). Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.
Downloadable file (.docx): Epinephrine Medication Card
Norepinephrine (Noradrenaline)
Endogenous epinephrine and norepinephrine (NE) work together to prepare the body to respond to acute stress by enhancing physical performance and alertness, ensuring that energy and oxygen are efficiently delivered to vital organs and muscles (UptoDate, 2021). When norepinephrine is given as a medication, it is used as a potent vasoconstrictor or vasopressor, increasing blood pressure by narrowing blood vessels. It is also used in low doses to improve cardiac output. It is only used in critical care areas with close hemodynamic monitoring.
The trade name is levophed.
Mechanism of Action
Norepinephrine is used as a peripheral vasoconstrictor due to its activation of alpha-1 receptors. It also has an inotropic effect on the heart and dilator of coronary arteries due to beta-1 adrenergic action. So, it is very similar to epinephrine, except it does not activate beta-2 receptors and minimal effect on alpha-2 receptors.
Indications for Use
- The use of norepinephrine is limited and is it is only given in critical care areas for clients with critically low blood pressure due to distributive shock or in cardiac arrest.
- At low doses, less than 2 mcg/min, the beta-1 effects are more pronounced with improved cardiac output. At higher doses of greater than 3 mcg/min, alpha-1 predominates, with vasoconstriction and increased systemic vascular resistance. NE can also increase cerebral blood flow with traumatic head injury that have impaired autoregulation (Smith & Maani, 2024).
Pharmacokinetics
Norepinephrine has a rapid onset of action with steady state obtained within five minutes. With a half life of approximately 2.5 minutes, it is administered by IV infusion. It is metabolized by the same enzymes in the liver as epinephrine, namely catechol-O-methyltransferase (COMT) and monoamine oxidase (MAO). It is excreted through the kidneys.
Jessica/Jan 14, 2026: @Copyeditor, please note that the nursing considerations in the sections above and below this part of the chapter are presented as bullet-point lists, except for this one section.
[DC/ Jan28: I think some of these sections should definitely be bulleted and it looks like some of them may have been previously bulleted already but lost the formatting, based on how they’ve been written. For content that is only one thought, such as “Mechanism of Action,” you don’t need a single bullet, but for subsections that have more than one thought, you should use bullets (E.g., “Indications for Use”] ok, this makes sense.
Nursing Considerations
High alert medication: norepinephrine is a potent vasopressor. Always have a second verifier for orders, drug calculations and infusion rates. Refer to pharmacist or drug monograph.
- Norepinephrine is only given by IV infusion due to its very short half-life and it is preferred to administer through a central line. It can be administered through a large bore peripheral line such as an antecubital fossa but very careful monitoring is required to avoid the risk of extravasation at the site. Adequate fluid resuscitation is required before and during therapy.
IV infusion
- NE is titrated to the desired arterial blood pressure or mean arterial pressure. A typical rate is 2 to 12 μg/min with close monitoring q 5-15 minutes to the set parameters in the orders. Infusions can go up to 30 μg/min depending on response. ECG monitoring is also required. Norepinephrine is only administered in critical care areas (Vallerand & Sanoski, 2021).
- Monitor urine output hourly, to ensure at least 30 mls/hr.
- Upon discontinuation, taper down slowly.
Lifespan considerations: Norepinephrine can be used for pediatric clients in septic shock. It can also be used in pregnancy, but reserved for profound hypotensive states or cardiac arrest. In the older adult, start the infusion at a low rate due to potential for renal and hepatic insufficiency with age.
Drug Interactions
- Drug interactions are similar to epinephrine. MAO inhibitors, tricyclic antidepressants and beta blockers can result in severe hypertension.
- Alpha adrenergic drugs can prevent norepinephrine’s hypertensive effects (Vallerand & Sanoski, 2021).
Adverse Effects
- Many of the adverse effects are the same as with epinephrine, and related to the alpha-1 effects, and are tachydysrhythmias, angina, and hypertension.
- There is a risk of end-organ hypoperfusion, and as such, the client should be hydrated appropriately. Reflex bradycardia via the baroreceptor reflex can occur, with cardiac output remaining unchanged despite the beta-1 action (Smith & Maani, 2024).
- Extravasation: This is a potential risk with peripheral IV administration, with the med leaking into local tissue and causing significant ischemia and subsequent necrosis. If it occurs, stop the infusion, draw back any injected medication if possible, and then treat the infiltrated area with phentolamine (non-selective alpha-adrenergic antagonist). Do not continue to use that site, and preferably reestablish the infusion with a different extremity or a central line (Smith & Maani, 2024).
Dopamine
Dopamine is a versatile catecholamine that functions as both a neurotransmitter and a hormone. In the central nervous system, dopamine is crucial for regulating mood, motivation, and reward, playing a significant role in the brain’s pleasure and reward pathways. This chemical messenger is also essential for motor control and acts as a vasodilator, particularly in the kidneys, where it helps regulate blood flow and sodium excretion. Additionally, dopamine influences gastrointestinal motility and modulates the release of various hormones, making it integral to multiple physiological processes.
Indications for use
As a medication, dopamine is used to treat hypotension, bradycardia and cardiac arrest. It has dose dependent effects on targeted arteries in the kidneys, heart and brain. It is administered through an infusion.
- Low doses: 0.5-3 μg /kg/min, stimulates dopaminergic (D1) receptors on the visceral vasculature, producing vasodilation, particularly in the kidneys, which increases urinary flow.
- Moderate doses: 2-10 μg /kg/min, stimulates dopaminergic and beta-1 receptors, increasing cardiac output by improving contractility and also renal vasodilation.
- High doses: >10 μg /kg/min, stimulates alpha-1 receptors, resulting in peripheral vasoconstriction improving blood pressure but can cause renal vasoconstriction (Vallerand & Sanoski, 2021).
Mechanism of Action
Dopamine is derived from tyrosine and is a precursor to norepinephrine and epinephrine and is also a neurotransmitter in certain areas of the central nervous system. It is a major transmitter in the extrapyramidal system of the brain and important in regulating movement. Dopamine exerts an agonist action on beta-adrenergic receptors and indirectly by causing release of NE from storage sites in sympathetic nerve endings resulting in positive chronotropic (increased heart rate) and inotropic effects (increased cardiac contractility) on the myocardium. In the brain, dopamine acts as an agonist to the five dopamine receptor subtypes (D1, D2, D3, D4, D5) (DrugBank, 2025; Sonne, Goyal & Patel, 2025).
Pharmacokinetics
Dopamine is administered by IV infusion, with onset of action within 1-2 minutes. It has a short half life of 2 minutes, with a duration of action of 10 minutes. It is not given orally as it would undergo extensive first pass effect. Dopamine is rapidly metabolized in the liver by MAO and catechol-O-methyltransferase, with excretion primarily through the kidney.
Nursing Considerations
- High alert medication: As a potent vasoactive medication, always have a second verifier for orders, drug calculations and infusion rates. Refer to pharmacist or drug monograph.
- Administration: Dopamine is administered into a large peripheral vein (antecubital fossa) or central line via infusion pump. It comes prepared in premixed 250- or 500-mL bags (ie. 400 mg/500 mL), or for dilution.
- Monitoring:
- Dopamine is given in critical care areas. Monitor BP, heart rate, ECG, central venous pressure (CVP) and urine output continuously.
- Report any changes such as low urine output or arrythmias. If low urine output decreases without hypotension, notify prescriber as dosage may need to be reduced.
- Monitor peripheral pulses and report any mottling or cool extremities.
- Close monitoring of blood pressure; adjust infusion if hypotensive and report changes.
- Ensure client is well perfused and correct hypovolemia.
- Extravasation risk: careful monitoring of site for skin irritation, necrosis and sloughing of tissue. If it occurs, flush with NS and phentolamine.
- Taper dose down for discontinuation.
- Dopamine is safe to administer to pediatric and older adults, with dosages adjusted.
- Pregnancy: there is no current data on safety during pregnancy, but should not be withheld due to life-threatening risk of untreated maternal shock. (Soone, Goyal & Patel, 2025; Vallerand & Sanoski, 2021)
Adverse/Side Effects
- Adverse effects include: Arrythmias, hypotension, angina, palpitations and decreased blood flow to the extremities.
- Side effects may include nausea, headache and dyspnea.
Client Teaching
Clients should contact their health care provider immediately if experiencing unusual sweating, dizziness, heart palpitations, or chest pain.
Dopamine Medication Card
Now let’s take a closer look at the medication card for dopamine (Sonne, Goyal & Patel, 2025; UptoDate, 2021; Vallerand & Sanoski, 2021). Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.
Downloadable file (.docx): Dopamine Medication Card
Interactive Activities
References
- Bassem Khalil; Alan Rosani; Steven J. Warrington (2024). Physiology, Catecholamines. National Library of Medicine.Stat Pearls. https://www.ncbi.nlm.nih.gov/books/NBK507716/
- Dalal, R. & Grujic, D. (2024). Epinephrine. National Library of Medicine. Stat Pearls. Epinephrine – StatPearls – NCBI Bookshelf
- DrugBank (2025). Dopamine. https://go.drugbank.com/drugs/DB00988
- Rosenjack Burchum, J., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
- Sealock, K. & Seneviratne, C. (2021). Lilley’s Pharmacology for Canadian Health Care Practice (4th ed.). Elsevier: Canada
- Smith, M. & Maani, C. (2024). Norepinephrine. National Library of Medicine. Stat Pearls. https://www.ncbi.nlm.nih.gov/books/NBK537259/
- Sonne, J., Goyal, A. & Patel, P. (2025). Dopamine. National Library of Medicine. Stat Pearls. Dopamine – StatPearls – NCBI Bookshelf
- UpToDate (2021). Dopamine. https://www.uptodate.com/contents/search
- UpToDate (2021). Epinephrine. https://www.uptodate.com/contents/search
- Vallerand, A. & Sanoski, C. (2021). Davis’s Canadian drug guide for nurses (18th ed.). F.A. Davis Company: Canada
- TRU Open Press. (2025). Physiological effects of catecholamines [AI-generated illustration]. Created using Canva AI (Premium).
Note. Illustration generated using Canva AI (Premium) by TRU Open Press (2025). Image is original to this work and licensed under the same Creative Commons CC BY NC SA licence as the text unless otherwise noted. [DC/Jan28: please see image note above!]
