7.9 Antilipemic Medications
Pharmacological treatment for managing dyslipidemia for the prevention of cardiovascular disease begins with screening individuals that includes age, health issues, family history, lifestyle factors, and lab work (Canadian Cardiovascular Society, 2021). Review unit 7.2 Conditions and Disorders related to Perfusion, Dyslipidemia.
Antilipemic agents are used to treat hyperlipidemia and dyslipidemia that may lead to additional health problems such as stroke, myocardial infarction, angina, and heart failure. The risk of atherosclerosis and coronary artery disease is directly related to increased levels of low-density lipoproteins (LDLs). If LDL levels decrease, this can slow the progression of atherosclerosis.
If after lifestyle changes are not successful at improving cholesterol levels, anti-lipemic meds are initiated. This therapy is long term and should be used in adjunct with a healthy diet and exercise regime. Some of the meds are used primarily to lower low-density lipoproteins (LDLs), some for lowering triglycerides, and others can help raise high density lipoproteins (HDLs).
Statins are often the first medication to be started and depending on the response, other cholesterol lowering meds will be added.
Treatment Guidelines
- Cholesterol screening done every 5 years for adults 40-75 years of age (earlier if risk factors for CAD). Labs include total cholesterol, LDL, HDL, triglycerides (TG).
- Identity high risk factors, including lifestyle and health issues (diabetes, family history of CAD).
Non- pharmacological interventions: diet, exercise, weight control, smoking cessation
LDL not lowered with diet, exercise, lifestyle changes → drug therapy is initiated along with ongoing lifestyle modifications
- Drug Therapy: HMB-CoA reductase inhibitors “statins” →reduce LDLs
- If ineffective, and depending on ongoing blood work, add on:
Bile-acid sequestrants – cholestyramine, colestipol and colesevelam (reduce LDLs)
Cholesterol absorption inhibitors – Ezetimibe (reduce LDLs)
- Along with the above, may add on drugs to raise HDL. Ie. Fibrates (lower TG, increase HDL)
To learn more about these interventions go to the 2021 Canadian Cardiac Society Dyslipidemia Guidelines and Resources, go to the following link: https://ccs.ca/guideline/2021-lipids/
In this unit, we will cover the following classes of meds:
- HMG-CoA Reductase Inhibitors (statins),
- Bile Acid Sequestrants,
- Fibrates,
- Niacin,
- Cholesterol Absorption Inhibitors.
HMG-CoA Reductase Inhibitors (statins)
HMG-CoA reductase inhibitors, more commonly known as statins, are the first line treatment to manage dyslipidemias and prevent cardiovascular disease. There are a number of meds in this class, including atorvastatin, lovastatin and simvastatin, that all differ in potency, metabolism and potential for side effects. For example, atorvastatin is more potent with higher ability to lower LDLs, whereas rosuvastatin is more hydrophilic with fewer muscle related side effects. Based on the client profile including age, risk factors and lab values, the prescriber will determine the most appropriate statin. Statins need to be used along with dietary and lifestyle modifications.
Atorvastatin will be our prototype medication.
Mechanism of Action
Atorvastatin inhibits HMG-CoA reductase and cholesterol synthesis, which reduces LDL (low density lipoprotein). Statins decrease cholesterol production in the liver by preventing HMG-CoA conversion to mevalonate. HMG-CoA is a rate limiting enzyme in cholesterol synthesis. When this enzyme is reduced, cholesterol production is decreased, resulting in hepatocytes making more HMG-CoA reductase (restoring cholesterol synthesis), increasing LDL receptor expression, and enhancing clearance of LDL from circulation. With more LDL receptors, the liver can remove more LDLs from the blood (McIver & Siddique, 2025).
Along with lowering LDL levels, statins also decrease the production of very low density lipoproteins (VLDLs), resulting in lower VLDL levels and triglyceride levels. Statins also increase HDLs levels (Rosenjack Burchum & Rosenthal, 2019).
Indications for Use
This medication is used for hyperlipidemia and the prevention of cardiovascular disease. It primarily lowers LDLs, but also has an effect on lowering triglycerides and increasing HDLs. Statins decrease the risk of CV disease, such as myocardial infarction, stroke, revascularization procedures, and angina. It is also prescribed for type 2 diabetics who have multiple risk factors to lower their CV risk (McIver & Siddique, 2025). Other effects include anti-inflammatory, anti-oxidant (helps protect cells from damage) and anti-proliferative (inhibits growth and division of cells) effects. They also have anti-inflammatory effects and improve endothelial dysfunction and vascular remodelling, helping to stabilize atherosclerotic plaques and reducing thrombosis. The extent of these other actions in improving CV health is less clear, and statins continue to be used for mostly for the reduction of lipid levels (Feingold, 2024).
Pharmacokinetics
Statins are rapidly absorbed after administration, with peak effect in 1-2 hours. It has extensive first pass effect. It is metabolized in the liver via CYP3A4 and CYP3A5. It is excreted in the bile.
Nursing Considerations
Administration: oral. Take at same time each day, with or without food.
For most statins, it is advised to take statins at bedtime as endogenous cholesterol synthesis occurs during fasting at night.
Atorvastatin has a long half life, so taking the med at any time of the day is acceptable, but need to be consistent with taking it at the same time.
Labs: liver enzymes (AST/ALT), creatine kinase (CK), lipid profile. Labs are drawn before therapy, 6 months after initiation and then every 5-12 months. Blood glucose levels drawn prior to therapy and regularly, depending on risk for diabetes.
Renal function: Renal function is not a concern with atorvastatin. Other statins would require a dose reduction if severe renal impairment, such as lovastatin or simvastatin.
Do not use with clients who have hepatic disease.
Pregnancy: contraindicated with clients who are pregnant or breastfeeding. If planning on becoming pregnant, stop statins three months prior to becoming pregnant.
Pediatrics: typically not given to children, but may be given in children 8-10 years of age with severe pediatric dyslipidemia.
Use caution with older adult due to increased risk for myopathy.
Drug Interactions:
Depending on the statin, drug interactions can be a concern due to effects with CYP3A4 metabolism. There are many meds that can interact with statins. If the client is on many other meds, atorvastatin may not be ideal as drugs that inhibit CYP3A4 will increase atorvastatin levels. In this case, other statins would be prescribed such as rosuvastatin. Drug interactions can occur with certain antibiotics, antifungals, calcium channel blockers, leading to higher statin levels and more risk for adverse effects.
Avoid grapefruit juice as it deactivates CYP3A4, leading to risk of serious adverse effects such as myopathies and elevated blood sugar levels.
Adverse/Side Effects
Generally well-tolerated with side effects uncommon. Most side effects are transient.
Side effects: headache, nausea, constipation, dyspepsia.
Adverse effects:
- Myopathy: injury to muscle tissue occurs in 5-10% of clients. Clients experience muscle aches, tenderness or weakness and can be diffuse or localized. Myositis (muscle inflammation) is rare, leading to elevated CK and potassium levels. Rarely, this can lead to rhabdomyolysis.
- Rhabdomyolysis is a condition in which damaged skeletal muscle breaks down rapidly, causing muscle pain and weakness. Labs show elevated myoglobin and marked elevation of CK which can cause renal impairment due to CK plugging up glomeruli. Symptoms include renal impairment and a characteristic tea-coloured urine (DailyMed, 2025). Increased risk of myopathy are the older adult, low vitamin D and coenzyme Q levels, high doses of statins, concurrent use of fibrates and those with multiple health disorders.
- Hyperglycemia: may increase blood sugar levels due to increasing insulin resistance or impairing insulin secretion in the beta cells. Risk of developing diabetes type 2 in pre-diabetic clients. Can raise H1C and random glucose levels.

Client Teaching
- Clients should take the prescribed medication as directed and do not double up missed doses.
- Avoid or limit consumption of grapefruit juice during drug therapy.
- Continue with dietary and lifestyle modifications.
- Inform client if they experience any muscle pain, tenderness, or weakness, these should be reported to the healthcare provider.
- When obtaining a prescription, ensure that their prescribed statin is not substituted for a different statin.
- If you plan to become pregnant, inform your health care provider. Statins are avoided during pregnancy.
- Inform prescriber is planning on taking any OTC medications, herbal supplements or vitamins as they may interact with the med.
Vallerand & Sanoski (2024)

Downloadable file (.docx): Atorvastatin Medical Card
Fibric Acid Derivatives (Fibrates)
Gemfibrozil, is a fibrate used to treat hypercholesterolemia and mixed dyslipidemia. It is used mostly to lower triglyceride levels, but can also raise HDL levels. It has minimal effects on lowering LDL levels. They are used less often due to higher risk of adverse effects when used with other antilipemic meds. As with all the antilipemic meds, dietary and lifestyle factors should be implemented. Other fibrates are fenofibrate and fenofibric acid.
Mechanism of Action
Fibrates work by decreasing plasma TG levels by lowering VLDL levels. They bind to PPAR-alpha, breaking down particles that make TGs in the liver. This can decrease TGs by as much as 30-60% They also breakdown cholesterol and suppress fatty acids from adipose tissue, and lastly increase the excretion of cholesterol in bile (Patel, Mathew & Singh, 2025; Vallerand & Sanoski, 2024).
Nursing Considerations
Administration: well- absorbed orally, excreted mostly unchanged in the kidney. Gemfibrozil should be taken before meals, and fenofibrate with meals to enhance absorption. Often BID dosing.
Labs: prior to therapy and regularly:
- Cholesterol levels (total cholesterol, LDL, HDL, TG), liver enzymes, CBC, Lytes and glucose
May cause hepatic dysfunction, monitor liver enzymes
Contraindicated if there is severe renal impairment.
May cause gallstones due to increased biliary cholesterol saturation. Monitor for symptoms of gall bladder disorder, such as RUQ pain, decreased tolerance to fried foods and bloating.
Pregnancy: high TGs can induce pancreatitis, so if TGs are elevated during pregnancy, then treat with omega-3 fatty acids with fenofibrate/gemfibrozil during the second trimester (Patel, Mathew & Singh, 2025).
Older adult: increased risk of myopathy if using both statins and fibrates.
Drug Interactions
- Statins: increased risk of statin-induced myopathy, leading to rhabdomyolysis. Monitor for muscle pain
- Warfarin: displaces warfarin from albumin leading to increased anticoagulant effects. Monitor INR and may need to reduce warfarin dosage.
Adverse/Side Effects:
Common side effects include abdominal pain, epigastric pain and diarrhea. Less common effects include blurred vision and muscle pain.
Client Teaching
- Take medication as directed, do not double up if dose missed.
- Take along with implementing dietary and lifestyle changes. Reduced fat, cholesterol and CHO foods, limit alcohol, exercise and quit smoking
- Inform client to report any abdominal pain, nausea, fever, muscle pain.
- Inform client to tell prescriber if they plan to become or are pregnant.
(Patel, Mathew & Singh, 2025; Vallerand & Sanoski, 2024).
Bile Acid Sequestrants
This class of meds has been around the longest and was once the mainstay in lipid-lowering therapy. They are not as potent as other med classes and are less tolerated, so they are used less today.
Mechanism of Action
Bile acid sequestrants bind to bile acids in the intestine, forming an insoluble complex that gets excreted in the feces resulting in a depletion of bile acids in the enterohepatic circulation. As bile acid concentrations decrease, more hepatic cholesterol converts to bile acids; this reduces hepatic cholesterol and increases hepatic LDL receptors to uptake LDL, resulting in a decrease in LDL blood concentrations (Lent-Schochet & Jialal, 2023).
Indications for Use
Bile acid sequestrants are used for hypercholesterolemia without hypertriglyceridemia. They are used in combination with other meds or monotherapy. They can lower LDL-C between 15 to 30% (Lent-Schochet & Jialal, 2023).
There are three types of bile acid sequestrants.: cholestyramine, colestipol and colesevelam. Colesevelam is the newer of the three and better tolerated. It is also used for clients with diabetes mellitus type 2 (T2D) to lower LDL and hemoglobin (Hb)A1c (Lent-Schochet & Jialal, 2023).
Colesevelam will be our prototype drug.
Nursing Considerations
Administration: oral in either a tablet or granules, usually in divided doses during the day. Dosages start low and taper up.
Assess lipid profile before initiating therapy. Lipid reduction can be observed after 2 weeks of therapy. Check fasting lipid profile 4-12 weeks after initiating therapy, then q 3-12 months.
Risk of GI obstruction, monitor bowel movements and fluid intake.
Can decrease blood glucose levels. Monitor blood glucose in diabetic clients.
Drug Interactions
Bile acid sequestrants decrease the absorption of many drugs by binding and excreting in the feces if taken at the same time. Medications known to form a complex with colesevelam include warfarin, thiazide diuretics, digoxin and some antibiotics. Take these meds one hour before or 4 hours after colesevelam.
Do not take fat soluble vitamins (vitamins A, D, E, K) within 4 hours of colesevelam (Rosenjack Burchum & Rosenthal, 2019).
Adverse/Side Effects
Side effects are gastrointestinal:
- Bloating, vomiting, heartburn, loss of appetite, indigestion, and upset stomach.
- Constipation especially in larger doses and older adults.
- Exacerbate peptic ulcer disease and hemorrhoids.
Client teaching:
- Take as prescribed. Do not take the powder dry.
- To avoid constipation, monitor bowel movements. Increase fluid intake and fiber in diet.
- Decreased effect of some meds if taken at the same time, inform client to take as prescribed.
- Monitor blood glucose levels if diabetic.
Cholesterol Absorption Inhibitor
Cholesterol absorption inhibitors are used alone or along with other antilipemic drugs such as HMG-CoA inhibitors. They are used to manage hypercholesterolemia.
The prototype med will be Ezetimibe.
Mechanism of Action
Ezetimibe blocks the absorption of cholesterol in the small intestines and reduces the delivery of intestinal cholesterol to the liver. It also reduces the hepatic cholesterol stores and increases the clearance of cholesterol from the blood. This results in a reduction of LDLs. It is is unique in that it does not affect the absorption of fat-soluble nutrients such as fat-soluble vitamins, triglycerides, or bile acids (Drug Bank, 2026).
Indications for Use
This medication is used for treatment of hyperlipidemia and familial hypercholesterolemia. It can reduce total cholesterol and LDL levels by up to 20%. It is used as a monotherapy or in combination with statins.
Ezetimibe, when used along with statins, provides a synergistic approach to lower LDL cholesterol by inhibiting both intestinal absorption and liver production. For high risk clients, this combination is safer than doubling the dose of statins alone (Nodari et al, 2007).
Nursing Considerations
Administration: oral dosage, taken once a day. Can be taken with or without food.
Labs: prior to therapy, liver enzymes and lipid panel. Monitor lipid panel 2-4 weeks after initiation, and then regularly.
If medication is combined with HMG-CoA reductase inhibitors, do not give to pregnant or breastfeeding clients.
Drug interactions: risk of gallstones if given with fibrates. Slight increased risk of liver toxicity with statins.
Adverse/Side Effects
Minimal side effects with monotherapy. Usually transient.
Side effects: runny nose, sore throat, headache
Use with caution when ezetimibe is combined with additional medication. Monitor for arthralgia, rhabdomyolysis if taking statins.
Client Teaching
- Clients should take the prescribed medication as directed and avoid consuming grapefruit juice during drug therapy.
- The medication should be used with dietary and lifestyle modifications.
- Inform client if they experience muscle pain, tenderness, or weakness, this should be reported to the healthcare provider.
- If you plan to become pregnant, inform your health care provider.
- Inform prescriber is planning on taking any OTC medications, herbal supplements or vitamins as they may interact with the med.
Vallerand & Sanoski, 2024
Nicotinic Acid
We will briefly review nicotinic acid. It is not commonly used anymore but may be prescribed in certain circumstances. Although it is a vitamin, it does have significant adverse effects that requires close monitoring.
Niacin, nicotinic acid and also known as vitamin B3, has been previously used to reduce cardiovascular events in clients with previous myocardial infarctions. It reduces LDLs, reduces triglycerides, and raises HDLs. It is rarely used today due to adverse effects, and lack of additional benefit when added to statins. But, for clients with a high risk of an MI and who cannot take statins, it is an option.
The most common side effect is cutaneous flushing due to the increase in prostaglandin release in the capillary beds. This can be mitigated if the client takes aspirin 30 minutes prior to their dose.
Other adverse effects include dyspepsia and nausea, although mild. In high doses, it can lead to high levels of uric acid resulting in gout, impaired glucose tolerance resulting in diabetes, and an increase in liver toxicity. It is contraindicated with active peptic ulcer disease and liver disease (DailyMed, 2025).
Careful monitoring is important, including assessing liver function, uric acid levels, and blood glucose monitoring.
Comparing Anti-Lipemic Medications
To help with comparing the medications and to learn important considerations for each medication, refer to the Chapter 7 Comparing Anti-lipemic Medications. This is a downloadable and editable document to allow you to update and add content. In clinical practice, always refer to current drug references for administration.
Clinical Reasoning and Decision-Making Questions
- A client is ordered a cholesterol absorption inhibitor: Ezetimibe. Which statement is true about this medication?
- Taken once a day due to long duration of action
- Avoid taking med with any food as absorption will be decreased.
- Only take the med in the evening due to cholesterol synthesis occurs at night.
- Taken TID as short duration of action. Sprinkle the granules on food.
2. The nurse has been caring for a patient admitted with dehydration. The patient has been taking Bile Sequestrant (colesevelam) regularly and complains of nausea. Which assessment finding would be of most concern for the nurse?
- Bloating after med administration
- Flatulence and belching
- Hypoactive bowel sounds and abdominal distension
- Indigestion and abdominal distention.
3. A client is started on HMG CoA inhibitor: Atorvastatin. Based on the cholesterol lab values, why would this med be prescribed?
- It lowers total cholesterol, HDL and LDL levels.
- It lowers total cholesterol and triglycerides (TG) moderately.
- It lowers LDLs minimally and raises HDL levels.
- d. It primarily lowers LDL levels with a decrease in total cholesterol and TG. HDL’s will be elevated.
4. The nurse provides some health teaching for a client starting on Atorvastatin. What will be important to include?
-
Report muscle aches and tenderness immediately
-
Report any dark stools and abdominal discomfort
-
Anticipate nausea and diarrhea which will reside after a few months.
-
Return for lab work in two weeks to see if the statin is working.
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 7: Cardiovascular Medications Answer key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
References
Canadian Cardiovascular Society. (2021). Dyslipidemia guidelines and resources. https://ccs.ca/guideline/2021-lipids/
DailyMed. (2025a). Atorvastatin calcium. U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=73cefb0b-1747-4fe0-b252-377f4ed94c6f
DailyMed. (2025b). Niacin. U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/
DrugBank. (2026). Ezetimibe. https://go.drugbank.com/drugs/DB00973
Feingold, K. R. (2024). Cholesterol lowering drugs. In Endotext. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/
Lent-Schochet, D., & Jialal, I. (2023). Antilipemic agent bile acid sequestrants. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK549906/
McIver, L., & Siddique, M. (2025). Atorvastatin. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK430779/
Nodari, S., Rocca, P., Saporetti, A., Bettari, L., Foresti, A., et al. (2007). The combination of ezetimibe and statin: A new treatment for hypercholesterolemia. Heart International, 3(1), Article 12. https://doi.org/10.4081/hi.2007.12
Patel, P., Mathew, C., & Singh, P. (2025). Fibric acid antilipemic agents. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/
Rosenjack Burchum, J., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier.
Vallerand, A. H., & Sanoski, C. A. (2024). Davis’s Canadian drug guide for nurses (19th ed.). F. A. Davis.
Media Attributions
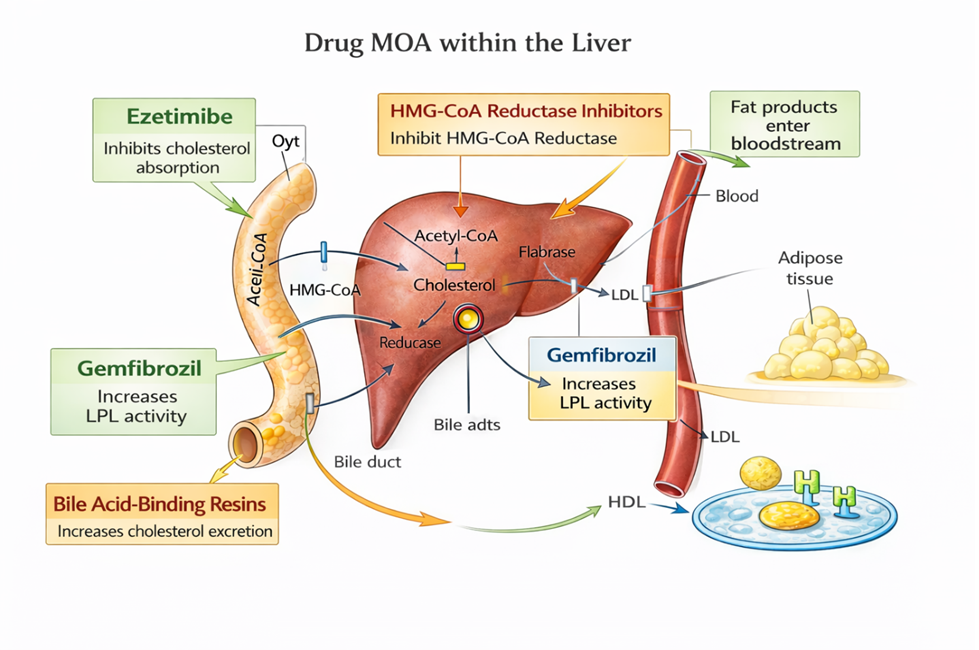
- 7.9a Mechanism of action of the different anti-lipemic medications is by Sheila Odubote, TRU Open Press; subject to the CC BY-NC-SA license.
- 7.9b File:RhabdoUrine.JPG – Wikimedia Commons by James Heilman, MD, on Wikimedia Commons, is used under the CC BY-SA 3.0 license.
- 7.9c Mechanism of action differences between ezetimibe and statins is by Sheila Odubote, TRU Open Press; subject to the CC BY-NC-SA license.

{kind=link}