11.5 Antidiabetics: oral medications V2
There are a number of oral anti-diabetic medications available to manage type 2 diabetes. Type 2 diabetes is complex, especially as the disease progresses and the client develops different health complications. Treatment will aim to prevent hyperglycemia and reduce the risk of cardiovascular (CV) and microvascular complications (Lipsombe et al, 2018). There are many factors the prescriber considers when prescribing oral agents:
- degree of hyperglycemia,
- medication efficacy for reducing diabetes complications (microvascular and/or CV) and lowering glucose,
- medication effects on the risk of hypoglycemia, body weight, other side effects,
- concomitant medical conditions, including level of frailty,
- renal function,
- ability to adhere to regimen,
- broader health and social needs, affordability of medications,
- patient values and preferences.
Lipsombe et al, (2018).
The importance of glycemic control in diabetes:
Controlling postprandial hyperglycemia is essential especially in the early years after a diabetes diagnosis. Good control reduces the incidence and progression of microvascular complications and in the long term (over 10 years) the risk of cardiovascular diseases (Lipsombe et al, 2018; Senior et al, 2020).
To obtain good glycemic control, healthy lifestyle behaviours that includes diet modifications and moderate exercise is needed for any anti-diabetic therapy.
The overall goal with treatment is to achieve an A1C of less than 7% for most clients.
Pharmacotherapy is started early and after a trial of healthy behaviour interventions. Metformin is the first line treatment if glycosated hemoglobin (A1C) target is not achieved after 3 months. Metformin is the first medication used due to its high safety profile, low cost and heart benefits. As the disease progresses, the addition of other oral meds will depend on many factors (outlined earlier), but controlling hyperglycemia and preventing CV disease are primary concerns. The addition of other medications may look like the following: the client is on metformin along with following healthy lifestyle behaviours. As the glycemic control gets worse, sulfonylurea medication (glipizide) is added. Over time, then the addition of a DPP-4 agent or SGLT2 inhibitor may be considered as they are associated with effective A1C lowering with less hypoglycemia than insulin or Thiazolidinediones (TZDs).
For some clients, insulin will be required. The addition of insulin is based on the degree of glycemic control. It may be decided to add insulin to oral anti-diabetic medication regime, so the insulin dose is small but still provides good glycemic control with less risk of hypoglycemia. In summary, the decision with all these medications is to manage any medication side effects, other health status issues such as hypertension or weight gain, and minimize microvascular complications (Lipsombe et al, 2018).
In this unit, the following meds that will be covered are:
- Biguanides (metformin)
- Sulfonylureas (glipizide)
- Alpha-glucosidase inhibitor (acarbose)
- Sodium-glucose cotransporter 2 inhibitors (canagliflozin),
- Dipeptidyl peptidase-4 (DPP-4) (sitagliptin)
Other medications that will not be covered include Thiazolidinediones (pioglitazone) and Cycloset (bromocriptine). Pioglitazone is what is considered an insulin sensitizer, and works by decreasing insulin resistance. It is an option for those who can’t take metformin or glipizide.
Bromocriptine, a sympathomimetic dopamine D2 receptor agonist, helps reverse insulin resistance and decreases glucose production (Ganesan, Rana & Sultan, 2023)
For an overview of how oral anti-diabetic medications work, watch the following YouTube video: Hasudungan, A. (2016). Pharmacology -Diabetic Medications. Pharmacology – Diabetes Medication
Biguanides
Metformin is in the only medication in the biguanide class of antihyperglycemics. It is the first medication that is prescribed for the majority of type 2 diabetic clients. It is effective, safe and low cost, making it an ideal drug as first line therapy. The therapeutic goal should be to decrease both fasting plasma glucose and glycosylated hemoglobin levels to near normal by using the lowest effective dose of metformin (Liscombe et al, 2018). Metformin can be used as monotherapy or in combination with sulfonylurea or insulin.
One of the distinct advantages of metformin is that it does not cause weight gain, making it ideal for clients overweight or average weight.
See Figure 11.5a for an image of a metformin tablet.

File:Metformin 500mg Tablets.jpg File:Metformin 500mg Tablets.jpg – Wikimedia Commons
Indications for use:
Metformin is used for type 2 diabetic clients as well as pre-diabetes and gestational diabetes. It improves glycemic control by lowering fasting and post-prandial blood glucose levels and improves glucose tolerance. It is quite effective and can lower A1C by 1.5-2%.
Off label, metformin can also be used for polycystic ovary syndrome (PSOS). PSOS is an endocrine disorder affecting androgen production and metabolism, resulting in irregular periods, infertility hirsutism and ovarian cysts. Metformin can increase insulin sensitivity and decrease insulin levels which indirectly can lower androgen levels. This results in improved glucose tolerance, improved ovulation and an increase in pregnancy rates (Rosenjack Burchum & Rosenthal, 2019).
Mechanism of Action
Metformin decreases hepatic glucose production, decreases intestinal absorption of glucose, and improves insulin sensitivity by increasing peripheral glucose uptake and utilization. It is quite effective in reducing A1C to near normal. Metformin has also shown benefit in reducing myocardial infarction in overweight clients (Lipscombe et al, 2018).
The benefit of metformin is that it does not produce hypoglycemia and does not cause weight gain. Unlike sulfonylureas, metformin does not produce hypoglycemia.
Nursing Considerations
Administration:
- Metformin should be given in divided doses with meals. Taking it with a meal will reduce the GI effects.
- Oral formula only, immediate release and extended release.
- May take up to 4 weeks to be fully effective.
As metformin does not cause hypoglycemia, it is suitable for clients who do not eat meals regularly. If they skip a meal, the blood sugars will not be affected (Rosenjack Burchum & Rosenthal, 2019).
Not metabolized and excreted unchanged in the kidney. It’s onset of action is one hour, and has a long t1/2 of 17 hours, therefore takes up to 4 days to leave the system.
Monitoring
- Fasting blood sugar and pre-meal blood sugar as recommended by prescriber. Hgb A1C twice a year or more frequently depending on glycemic control.
- Renal function, complete blood count (CBC), B12 and folate at start of therapy and then yearly (Ganesan, Rana & Sultan, 2023)
Contraindicated in clients with kidney disease (e.g., serum creatinine levels ≥ 115 μmol/L [males] or ≥ 95μmol/L [females]).
Contraindicated with hepatic disease, heart failure, metabolic acidosis or the elderly.
Caution with CT scan: temporarily discontinue metformin undergoing radiologic studies involving IV administration of iodinated contrast, due to acute alteration of renal function.
Caution with surgery: clients who are going for surgery, Metformin should be held on the day of surgery and restarted 48 hours after surgery. Renal function, creatinine, will be monitored.
Drug Interactions:
Advise clients to not take new medications or herbal supplements without consulting with their prescriber.
- The effects of metformin are increased with furosemide, cimetidine, and digoxin.
- Ginseng and garlic herbal supplements have an additive effect leading to hypoglycemia
Adverse/Side Effects
The most common side effects are decreased appetite, nausea and diarrhea which go away after a few weeks. Common adverse reactions include vomiting, weakness, flatulence, indigestion, abdominal discomfort, and headache.
Reduction in B12 levels and folate with long term use. B12 deficiency can contribute to peripheral neuropathy which is a long-term consequence of diabetes. B12 levels should be monitored yearly and the client should be taking supplements (Rosenjack Burchum & Rosenthal, 2019).
Lactic Acidosis Risk:
- Lactic acidosis is a rare, but serious, metabolic complication that can occur due to metformin accumulation, often due to high doses or acute kidney injury so it is not excreted. Symptoms include hypotension, bradycardia, diarrhea and dizziness, and often subtle nonspecific symptoms such as malaise, myalgias, increasing somnolence, and nonspecific abdominal distress.
- when it occurs, it is fatal in approximately 50% of cases.
- The risk of lactic acidosis increases with the degree of renal dysfunction and the client’s age. Metformin inhibits the mitochondrial oxidation of lactic acid. If metformin is not normally excreted, it accumulates, and lactic acid occurs.
- Hold metformin in the presence of any condition associated with hypoxemia, dehydration, or sepsis. Because impaired hepatic function may significantly limit the ability to clear lactate, metformin should be avoided in clients with hepatic disease.
(Ganesan, Rana & Sultan, 2023)
Client Teaching
- Clients should take the medication at the same time each day.
- This medication does not cause hypoglycemia. But clients should be instructed regarding the signs of hyperglycemia and hypoglycemia.
- The client may be at risk for lactic acidosis and should report chills, low blood pressure, muscle pain, or dyspnea immediately to the healthcare provider.
- The use of medications like metformin can cause a metallic taste in the mouth.
- May cause GI upset, but will subside after a few weeks.
- Regularly monitor blood glucose levels.
- If going for surgery, anticipate metformin to be discontinued the day before surgery and resumed 48 hours afterwards.
- Avoid or limit alcohol intake as it can increase risk of hypoglycemia and lactic acidosis.
Sulfonylureas
Sulfonylureas are considered a second line treatment option after metformin. They can be taken as monotherapy or along with other anti-diabetic meds.
Our prototype medication is glipizide. Glyburide is the long-acting formula.
Mechanism of Action
Sulfonylureas, also called ‘insulin secretagogues” due to the action of mimicking insulin. It works by stimulating insulin secretion from the beta cells of pancreatic islet tissue. It is dependent on functioning beta cells and works regardless of blood sugar levels. They stimulate insulin release by blocking ATP-sensitive potassium channels in the cell membrane, the membrane depolarizes, permitting calcium into the beta cell and thereby releases insulin. Secondary actions include reducing glucagon production in the liver and increasing insulin sensitivity in peripheral tissues, which overall reduces blood glucose levels (Rosenjack Burchum & Rosenthal, 2019).
Nursing Considerations
Administration: oral only, taken once a day or BID.
- Take 30 minutes before a meal
- Immediate release formula is glipizide, taken once daily or BID.
- Long-acting formula is glyburide, taken once or twice a day. Duration of action is 16-24 hours.
- Effectiveness will diminish over time.
- Onset of action 45-50 minutes, with t 1/2 10 hours
Metabolized in the liver by P450 enzymes and renally excreted.
Contraindicated with glucose 6-phosphate dehydrogenase (G6PD) deficiency as can lead to hemolytic anemia.
Monitoring:
- Ensure to check blood glucose regularly
- Observe for signs of hypoglycemia (sweating, hunger, weakness, tachycardia, tremor, dizziness)
- Ensure client eats regular meals and does not skip
- Avoid alcohol
- Monitor renal function (GFR, creatinine, BUN) and liver function
- Before first dose, ensure no allergy to sulfa antibiotics
Do not use if pregnant as it will cross placental barrier and may lead to teratogenic effects. The only oral anti-diabetic medication to take while pregnant is metformin.
Gliclazide preferred over glyburide due to lower risk of hypoglycemia.
Drug Interactions:
- Increased risk of hypoglycemia with nonsteroidal anti-inflammatory agents or drugs that are highly protein bound.
- Cross sensitivity with sulfa antibiotics. If allergic to sulfa antibiotics, should be avoided.
- Beta blockers can suppress insulin release, leading to diminished sulfonylurea effects.
(Lipscombe et al, 2018; Vallerand & Sanoski, 2024)
Adverse/Side Effects
The two main side effects are hypoglycemia risk and weight gain.
Risk of hypoglycemia (recall it lowers blood sugar levels regardless of level). Hypoglycemia risk increased if:
- elderly client. Avoid if client over 80 years of age
- taking the long-acting formulation, Glyburide.
- alcohol should be avoided to prevent hypoglycemia
- Skipping meals
Client Teaching
- Clients should take the medication at the same time each day. If a dose is missed, take as soon as you remember, unless close to the time of the next dose.
- It is important that clients understand that the medication helps control episodes of hyperglycemia but does not cure diabetes.
- Clients should be instructed regarding the signs of hyperglycemia and hypoglycemia.
- The use of sulfonylureas and alcohol may cause a disulfiram-like reaction, such as flushed skin, tachycardia, nausea and abdominal pain.
- Advise client to monitor pre-meal glucose periodically.
- If sick, monitor glucose and ketone levels. If not eating, do not take sulfonylurea med.
- Use sunscreen due to risk of photosensitivity.
- Carry a form of sugar in case of hypoglycemia
(Ganesan, Rana & Sultan, 2023; Vallerand & Sanoski, 2024)
Alpha–glucosidase Inhibitors
Alpha-glucosidase inhibitors (AGI) are a class on anti-diabetic medications that are used for clients who do not tolerate metformin or sulfonylureas, or who are a high risk of hypoglycemia. They are also used for clients with impaired glucose tolerance, which can delay the onset of diabetes (Akmal, Patel & Wadhwa, 2024). They are used as an adjunct to healthy diet and exercise.
The prototype medication is acarbose. Other medication in this class is miglitol.
Mechanism of action
Acarbose hampers the digestive enzyme, alpha-glucosidase, that breaks down carbohydrates into smaller sugars that can be absorbed by the intestines. This slowing of the digestion and absorption of carbohydrates results in a slower rise in blood sugar levels and insulin has more time to work effectively. In more detail, acarbose competitively inhibits alpha-glucosidase enzymes in the intestinal brush border cells that digest dietary starch. This results in inhibiting polysaccharide reabsorption and the metabolism of sucrose to glucose and fructose (Ganesan, Rana & Sultan, 2023).
This action is useful in reducing postprandial hyperglycemia, and also glycosylated hemoglobin levels and also reduce postprandial insulin concentration. AGIs also reduce glucose variability throughout the day which is a contrast to other oral anti-diabetic meds (Akmal, Patel & Wadhwa, 2024).
AGIs are sometimes referred to as ‘starch blockers’.
Nursing Considerations
Administration: oral dosing, taken three times a day, with ‘first bite of a meal’. Peak effect is one hour. Dose should be started low and tapered up depending on adverse effects and desired glycemic control.
Contraindicated with bowel disease such as inflammatory bowel disease or Chron’s disease.
Contraindicated with hepatic disease. Monitor liver enzymes (AST and ALT) as there is a slight risk of hepatitis. Risk decreases over time.
Drug Interactions:
Acarbose can decrease the absorption of acetaminophen, digoxin and propranolol.
(Akmal, Patel & Wadhwa, 2024).
Adverse/Side Effects
AGIs are very safe, and are not absorbed systemically. They do not cause hypoglycemia or weight gain, as with other oral meds.
Side effects of flatulence and diarrhea are common and subside over time. Flatulence is due to the fermentation of unabsorbed carbohydrates in the intestine.
Other side effects include: abdominal distention and borborygmus. May cause decreased absorption of iron.
Client Teaching
- Clients should take the medication as prescribed. Take the med with each meal, three times a day and with the first bite of their meal.
- It is important that clients understand that the medication will help with glycemic control.
- Routine blood work including blood glucose levels and A1C are required. Liver enzymes will be assessed prior to therapy and periodically.
- Do not start new medications or herbal supplements without discussing with prescriber.
Dipeptidyl peptidase-4 (DPP-4)
Also known as the ‘gliptins’, DPP-4 inhibitors are a well-tolerated anti-diabetic medication that works by stimulating glucose-dependent insulin secretion, inhibits glucagon release and slows gastric emptying. In Canada, there a number of combination or individual medication formulations available. All DPP-4 inhibitors end in ‘-gliptin’, and include sitagliptin, saxagliptin, vildagliptin, and linagliptin. Our prototype medication in this class will be sitagliptin.
What is DPP-4?
DPP-4 is an enzyme that acts on incretin hormones, mainly GLP-1 (glucagon-like peptide-1) and GIP (gastric inhibitory peptide), both which maintain glucose homeostasis by increasing insulin secretion and decreasing glucagon secretion.
- GLP-1 is a hormone secreted by enteroendocrine L cells of the small intestine, which lowers blood glucose by stimulating insulin secretion, reducing glucagon concentrations, and delaying gastric emptying.
- GIP is a hormone secreted in the stomach and proximal small intestine by neuroendocrine K-cells.
These incretins are released within minutes of food intake, and DPP-4 degrades these hormones immediately due to their short half-life. By inhibiting the DPP-4 enzyme, DPP-4 inhibitors increase the levels of GLP-1 and GIP, which in turn increase beta-cell insulin secretion in the pancreas, thereby reducing postprandial and fasting hyperglycemia (Kasina & Baradhi, 2023).
Mechanism of Action
Sitagliptin is an orally-active inhibitor of dipeptidyl peptidase-4 (DPP-4) enzyme that slows the inactivation of incretin hormones involved in the regulation of glucose homeostasis. The incretin hormones, glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide (GLP-1), become deactivated, and control glucose by decreasing glucagon release, increasing glucose-dependent insulin release, decreasing gastric emptying and increasing satiety. The main effects are increasing insulin release and decreasing glucagon levels in the circulation. See figure 11.5b.
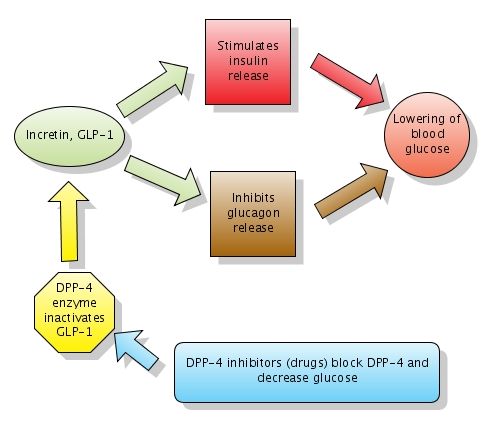
Incretins_and_DPP_4_inhibitors.jpg (488 × 427 pixels, file size: 26 KB, MIME type: image/jpeg
Retrieved from File:Incretins and DPP 4 inhibitors.jpg – Wikipedia
Nursing Considerations
Administration: oral dosing, taken once a day. Can be taken with or without food. Can be taken before or after meals.
It is absorbed rapidly with a duration of action of 24 hours.
Dose adjustment should occur for clients with kidney disease depending on their glomerular filtration rate.
Monitoring includes A1C prior to therapy and periodically. Monitor renal function prior to and periodically during therapy.
There are no adverse drug interactions. Increased risk of hypoglycemia if taken with insulin or sulfonylurea medications.
Adverse/Side Effects
Sitagliptin is generally well-tolerated. It has a slight risk of causing hypoglycemia, especially if taken with other oral anti-hypertensives.
Risk of nasopharyngitis, with symptoms such as runny nose and sore throat.
It may cause an increased serum creatinine levels so monitor renal panel periodically.
In rare circumstances, it may cause:
- Pancreatitis: symptoms such as upper abdominal pain, anorexia, nausea, and fever.
- severe joint pain or myalgia
- hypersensitivity reaction such as Steven-Johnson syndrome. DPP-4 is found in T cells, so inhibiting DPP-4 may lead to an increased hypersensitivity response. Report any rash, blisters/erosions.
Report hypersensitivity reactions, blisters/erosions, headache, or symptoms of pancreatitis, heart failure, severe arthralgia, and upper respiratory infection.
(Ganesan, Rana & Sultan, 2023; Kasina & Baradhi, 2023)
Client Teaching
- Take the medication at the same time each day. Do not double up a dose if one is missed.
- Inform client this med helps control hyperglycemia, and is a long-term medication.
- Ensure to continue with a healthy diet and exercise plan.
- Clients should stop taking the medication if symptoms of hypersensitivity occur such as a rash, swelling of the tongue or face, difficulty breathing. Follow up immediately with their provider to determine the next course of treatment.
(Vallerand & Sanoski, 2024)
Sodium-glucose Cotransporter 2 Inhibitors
Sodium-glucose cotransporter 2 inhibitors (SGLT-2i) are prescribed for type 2 diabetic clients with later stage diabetes that have cardiovascular disease or with end-stage renal disease or diabetic nephropathy. It is also prescribed to heart failure clients without diabetes. SGLT2 drugs improve glycemic control, lowering A1C levels by 0.5% to 1.0% in clients with T2DM (Padda, Mahtani & Parmar, 2025). They also reduce the risk of cardiovascular death including nonfatal MI and stroke, and reduce the risk of end-stage renal disease (Vallerand & Sanoski, 2024).
Medications in this class include canagliflozin and dapagliflozin. Our prototype medication will be canagliflozin. Canagliflozin is always used along with a healthy diet and exercise.
Mechanism of Action
SGLT-2 inhibitors work in the proximal renal tubule. They inhibit glucose being reabsorbed back into the blood stream so more glucose is excreted in the urine. Water will follow glucose, so the client will experience increased urination. Overall, it inhibits the reabsorption of glucose, lowers the renal threshold for glucose and increases the excretion of glucose in the urine (Vallerand & Sanoski, 2024).
What is sodium-glucose cotransporter-2?
SGLT-2 is a transport protein of glucose uptake in cell membranes. They are located in the proximal tubule of the nephron and also in the small intestine. SBLT-2 is responsible for 80-90% of filtered glucose reabsorption back into the bloodstream. SGLT-2 inhibitors block this transport, so more glucose is excreted by the kidney.
Nursing Considerations
Administration: taken orally, once a day before breakfast.
Metabolized in the liver, and renally excreted.
Pediatric clients: can be used for clients over the age of 10.
Drug interactions:
- Hyperkalemia risk with clients also on angiotensin-converting enzyme inhibitor or angiotensin receptor blockers. Monitor electrolytes and renal function. This is more of a concern if client as renal impairment (Padda, Mahtani & Parmar, 2025).
- Hypoglycemia risk with clients taking insulin secretagogues, such as a sulfonylurea, or insulin. Dose reduction of the insulin secretagogue or insulin to minimize this risk.
- Lithium: clients on lithium and SGLT-2 inhibitors can have reduced serum lithium concentrations. This is due to lithium-glucose reabsorption is decreased, resulting in higher amount of renal excretion of sodium, glucose, and lithium. Concurrent use of an SGLT2 inhibitor with lithium can reduce serum lithium concentrations (Padda, Mahtani & Parmar, 2025).
- If the client is on a diuretic such as furosemide, dosage may need to be reduced.
There are cardioprotective effects to make it advantageous for clients with cardiovascular disease. These include:
- Blood pressure reduction: by inhibiting SGLT2 in proximal tubules, resulting in an increase in distal tubular sodium delivery, resulting in suppressing the renin-angiotensin-aldosterone system. This leads to a reduction in preload, driven by natriuresis and diuresis, and afterload, mediated by arterial vasodilation.
- Weight loss due to a slight decrease in adipose tissue and interstitial fluid
- Small increase in HDL
- Potentially improving cardiac efficiency and exerting antiarrhythmic effects through membrane potential stabilization (Padda, Mahtani & Parmar, 2025).
Other benefits include improved glycemic control with a reduced A1C, and no risk of hypoglycemia. It also reduces the progression of nephropathy. SGLT2 inhibitors also decrease effective circulating volume, lower blood pressure, and induce modest weight loss.
Monitoring:
Labs: prior to therapy and periodically: A1C, renal panel, electrolytes, serum lipid levels.
Monitor for hypoglycemia and volume depletion (dizziness, weakness, orthostatic hypotension).
Close monitoring is required for the older adult, clients with hypotension, renal insufficiency with a GFR less than 45, and clients with history of urinary tract infections (UTI).
- History of UTIs: due to glycosuria from SGLT-2 inhibitors, there is a higher risk of UTIs. Ensure the client has good perineal hygiene, and is well-hydrated.
- Hypotension risk: SGLT-2 inhibitors may cause hypotension. Assess for dizziness or syncope. Ensure the client is well-hydrated.
- SGLT-2 inhibitors can cause euglycemic diabetes (Normal blood glucose but with increased ketones in the urine). Monitor ketone levels periodically. If the client is sick or can’t drink, ensure to check ketones and notify prescriber.
Renal or hepatic impairment: SGLT2 inhibitors is not recommended for glycemic control in clients with an eGFR less than 30 mL/min/1.73 m². For mild to moderate hepatic impairment, dose adjustment of SGLT2 inhibitors is not required.
Pregnancy: Not recommended for clients who are pregnant, due to risk of fetal harm especially in the 2nd and 3rd trimesters.
Surgery or major illness: for clients going for major surgery or who are very ill, hold SGLT-2 inhibitors.
(Lipsombe et al, 2018; Padda, Mahtani & Parmar, 2025; Vallerand & Sanoski, 2024).
Adverse/ Side Effects
Sodium-glucose cotransporter-2 inhibitors are generally well-tolerated with a good safety margin. For clients who are more at risk for adverse effects, close monitoring is required.
Adverse effects include:
- Urinary tract infections and female genital mycotic infections (vulvovaginal candidiasis, bacterial vaginitis): glycosuria creates a favourable environment of bacterial growth, resulting in infections.
- Acute kidney injury: higher risk due to the decrease in intravascular volume. Older adults, those on diuretics or those with renal impairment are more at risk.
- Small increase in LDL-C: monitor lipid profile prior to therapy and periodically. Clients may also experience a small increase in HDLs.
- Diabetic ketoacidosis: less common but monitor for symptoms of DKA such as metabolic acidosis, ketones in the urine, and hypoglycemia. Discontinue SGLT-2 inhibitors.
- Hypotension and intravascular volume reduction: monitor for dizziness, assess blood pressure. Additional hydration may be required.
Client Teaching:
- Take the medication at the same time each day. Do not double up a dose if one is missed.
- Inform client this med helps control hyperglycemia, and is a long-term medication.
- Review signs of hypoglycemia with the client. If hypoglycemia occurs, drink orange juice, eat 2-3 tsp of sugar or honey.
- Monitor blood sugars periodically and urine ketones, especially when unwell or under stress.
- Ensure to continue with a healthy diet and exercise plan.
- Inform client of a risk of urinary bacterial or yeast infections, and monitor for symptoms. Ensure good personal hygiene and hydration.
- Report any new pain or tenderness, sores or infections especially if it involves the feet or legs, genital area. Report any fever or unexplained malaise.
- Clients should stop taking the medication if symptoms of hypersensitivity occur such as a rash, swelling of the tongue or face, or difficulty breathing. Follow up immediately with their provider to determine the next course of treatment.
(Vallerand & Sanoski, 2024)
Oral Anti-Diabetic Medication Card
Now let’s take a closer look at the oral anti-diabetic medications. This table is intended to consolidate the information about each medication. Access the downloadable and editable format to add information that helps you with learning about each medication.As information with medications is always changing, refer to a drug reference or monograph. Comparing Oral Anti-Diabetic Medications table
Note:
- All anti-diabetic medications require healthy lifestyle behaviours such as healthy diet, moderate exercise and limit alcohol intake.
- Tight glycemic control is important to prevent hyperglycemia and minimize long term cardiovascular complications.
- Oral anti-diabetic therapy usually begins with metformin, and then additional meds added to improve glycemic control and manage health issues.
| Class | MOA /Therapeutic effects | Administration Considerations /Key points | Adverse/Side Effects |
| Sulfonylureas
Gliclazide “insulin secretagogues” |
MOA: Stimulates pancreas to make more insulin & reduces glucagon levels
Reduce FBG & glycosylated hemoglobin to near normal |
|
|
| Biguanide
Metformin |
MOA: Blocks livers release of glucose and ↓ insulin resistance. Increases glucose uptake by cells (muscle, fat)
PCOS: increases insulin, results in decrease androgen levels Safe with Gestational Diabetes
Reduce FBG & glycosylated hemoglobin to near normal |
|
• Common AEs: GI -diarrhea, nausea/vomiting, weakness, flatulence, indigestion, abdominal discomfort, and headache
• Metallic taste Stop immediately if signs of lactic acidosis (LA) or any condition associated with hypoxemia, dehydration, AKI, or sepsis occurs. • Risk of LA with furosemide, cimetidine. • Drop in B12 levels with long term use. Monitor and take supplements if needed. |
| DPP-IV inhibitor
Sitagliptin
“gliptins” |
MOA: Inhibits DPP-4 – inhibits incretin GIP and GLP-1 decrease glucagon release and increase insulin release, decr gastric emptying and increase satiety
Reduce FBG & glycosylated hemoglobin to near normal |
|
• Hypoglycemia
• Upper respir tract infections, sore throat, diarrhea, headache Slight risk of Steven Johnson syndrome – report hypersensitivity reactions, assess for rash, blisters/erosions. • Assess for symptoms of pancreatitis, heart failure, severe arthralgia • Slight risk of pancreatitis |
| Alpha Glucosidase Inhibitors
Acarbose “starch blockers”
|
MOA: inhibits alpha- gluc digestive enzyme that breaks CHOs into simple sugars in intestine… slower absorption of CHO and slower rise in BG. Does not depend on insulin.
|
|
• Flatulence, diarrhea – decreases with time
• Do not take if bowel disorders • Monitor se Creatine and se transaminase levels q 3months first year of tx then yearly • Decrease iron absorption
|
| Sodium Glucose Cotransporter 2 inhibitors
Canagliflozin
|
MOA: Inhibits SG cotransporter 2 in proximal tubule of renal glomeruli – 90% reduction of glucose reabsorption.
Lower glucose reabsorption / Glycosuria and increased urine output CV benefits – lowers BP, ↑HDL, weight loss
|
|
• ↑LDL and ↑HDLs
• UTI risk and bacterial vaginosis – good hygiene, hydrate • Risk of euglycemic DKA • increased urine output – Risk of volume depletion/ hypotension • Ketoacidosis espec if unwell or sick. Monitor ketones and se glucose Monitor renal fcn and LDL – baseline and periodically Client teaching: drink 1-2 extra glasses of H2O each day, monitor for dehydration, monitor for yeast infections, stop med if ill or can’t drink |
| Semaglutides
Ozempic, Rybelsus
“Incretin mimics”
|
MOA: Activates GLP-1 receptors in intestine, pancreas and hypothalamus
· In intestine, slows gastric emptying · Stimulates insulin production (enhances beta cells) and release, lowers prod of glucagon from liver, · in hypothalamus to decrease cravings and increase satiety. Used for: T2 DM, CV risk management, weight loss. Long term management |
· Ozempic: SQ weekly, doses titrated up each week until goal dose reached.
· Rybelsus: oral once a day, doses titrated up each week until goal dose reached. · Lowers BP, improves myocardial contractility, mild diuretic effect, lowers lipids. · Improves glycemic control, weight loss |
• GI: nausea, diarrhea, flatulence
• Lowers blood glucose Adverse effects: gastroparesis, pancreatitis, retinopathy, thyroid tumours, vision changes Longterm management. If med d/c’d: weight gain |
Critical Thinking and Decision-Making Learning Activities
A client with diabetes mellitus type 2 is admitted to the hospital for hip replacement surgery. The nurse reviews the following orders:
Bedside blood glucose testing before meals and at bedtime with sliding scale Humalog insulin
Sliding scale Humalog insulin based on preprandial glucose level:
- 0 – 8.0 mmol/L: No coverage
- 8.1 – 10.0 mmol/L: 2 units
- 10.1 – 11.0 mmol/L: 4 units
- 11.1 – 12.5 mmol/L: 6 units
- 12.6 – 14.0 mmol/L: 8 units
- Over 14.0 mmol/L: call the provider
Metformin 1000 mg twice daily
Humulin-N 20 units at breakfast and at bedtime
Hypoglycemia protocol
- Explain the difference between type 1 and type 2 diabetes.
- The client states that he usually does not take insulin at home. What is the likely rationale for insulin therapy while hospitalized?
- The client’s blood sugar before breakfast is 12.4 mmol/L. What types and amounts of insulin will the nurse administer?
- The nurse reviews the client’s morning lab results and finds a creatinine of 160 μmol/L. She plans to call the provider to discuss the impact of the results on the medications ordered. Which medication may require a dosage adjustment based on these results?
- When the nurse enters the room around 4 p.m., she discovers that the client has become irritable and is shaky. The nurse performs a bedside blood glucose and obtains a value of 3.1 mmol/L. What is the nurse’s best response?
- What is the likely cause of the client’s condition? Explain using the onset and peak actions of the insulin orders.
- On admission, the client’s A1C level was 10%. What does this lab value indicate?
- The provider states the discharge plan is to initiate Lantus insulin therapy at home, based on the admitting A1C level. What client teaching should the nurse plan to provide before discharge?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 11: Endocrine System Medications: anti-diabetic medications answer key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
References
Akmal, M., Patel, P. & Wadhwa, R. (2024). Alpha Glucosidase Inhibitors. National Library of Medicine. Alpha Glucosidase Inhibitors – StatPearls – NCBI Bookshelf
Ganesan, K., Rana, M. & Sultan, S. (2023). Oral hypoglycemic medications. National Library of Medicine. StatPearls [Internet]. Treasure Island (Fl). StatPearls Publishing.
Kasina, S. & Baradhi, K. (2023). Dipeptidyl Peptidase IV (DPP IV) Inhibitors. National Library of Medicine. StatPearls. Dipeptidyl Peptidase IV (DPP IV) Inhibitors – StatPearls – NCBI Bookshelf
Lipsombe L, Booth G, Butalia S, Dasgupta K, et al. (2018). Diabetes Canada 2018 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada: Pharmacologic Glycemic Management of Type 2 Diabetes in Adults. Canadian Journal of Diabetes, 42 (Suppl 1): S88-S103. https://guidelines.diabetes.ca/cpg/chapter13
Padda, I., Mahtani, A. & Parmar, M. (2025). Sodium-Glucose Transport 2 (SGLT2) Inhibitors. National Library of Medicine. StatPearls [Internet]. Sodium-Glucose Transport 2 (SGLT2) Inhibitors – StatPearls – NCBI Bookshelf
Rosenjack Burchum, J., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
Senior, P., Houlden, R., Kim, J., MacKay, D., Nagpal, S., et al. (2020). Pharmacological glycemic management of type 2 diabetes in adults: 2020 update – the user’s guide. Canadian Journal of Diabetes, 44, 592-596.
Vallerand, A. & Sanoski, C. (2024). Davis’s Canadian drug guide for nurses (19th ed.). F.A. Davis Company: Canada
Media Attributions
- Figure 11.5a Metformin tablets. File:Metformin 500mg Tablets.jpg File:Metformin 500mg Tablets.jpg – Wikimedia Commons
- Figure 11.5b Mechanism of Action of DPP-4 Inhibitors. Incretins_and_DPP_4_inhibitors.jpg (488 × 427 pixels, file size: 26 KB, MIME type: image/jpeg. Retrieved from File:Incretins and DPP 4 inhibitors.jpg – Wikipedia

{kind=link}
{kind=link}
{kind=link}