10.3 Corticosteroids V2
The adrenal cortex produces three types of hormones that have a role in the normal homeostasis or functioning of our bodies. These include androgens (regulation of sexual function), mineralocorticoids (regulation of water and electrolytes) and glucocorticoids.
Defining terms: corticosteroids is the umbrella term for both glucocorticoids and mineralocorticoids. In practice, corticosteroids generally refer to the glucocorticoid effect.
Glucocorticoids + mineralocorticoids = Corticosteroids
To fully understand how the corticosteroid medications work as well as important nursing considerations, nurses need a solid understanding of the physiological effects of each of these hormones. Refer to unit 10.1 or other references. In this unit, we will do a brief physiology overview. Following that, we will examine corticosteroids, namely glucocorticoids.
The focus of this unit will not include mineralocorticoids, such as aldosterone, which is for water and electrolyte regulation.
Endogenous corticosteroids (glucocorticoids) are involved in a range of metabolic, immunosuppressant, anti-inflammatory and central nervous system effects. They are regulated by a negative feedback mechanism.
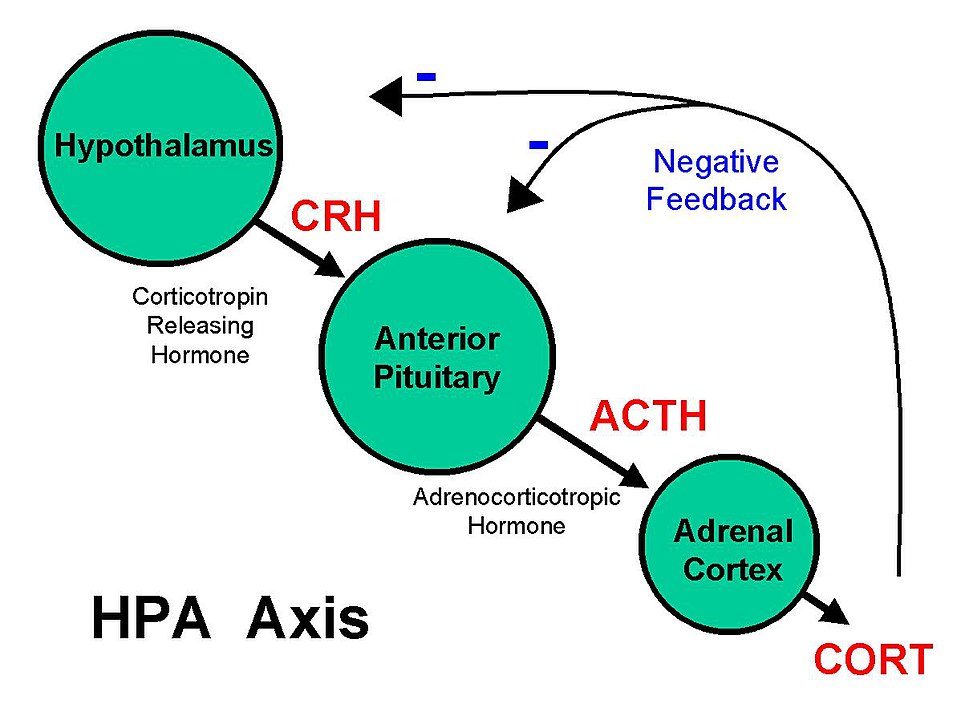
Regulation and synthesis of glucocorticoids:
The endogenous storage of glucocorticoids is minimal, so whatever is needed is produced. When cortisol levels are low, such as in the evening, the hypothalamus releases cortico-tropin releasing hormone (CRH) into the bloodstream, which travels to the anterior pituitary gland. This triggers the release of adrenocorticotropin hormone (ACTH). ACTH then travels via the blood to the adrenal cortex which stimulates the production of cortisol. When cortisol levels peak, it signals negative feedback to the hypothalamus and HPA, which is then inhibited, until cortisol levels are low enough to start over again. Basal levels follow the circadian rhythm. Cortisol levels are lowest at bedtime, rise during sleep and reach a peak just before waking.
If there is stress, such as surgery, emotional stress, infection, or pain, the amount of cortisol released goes up. Cortisol regulates many functions including our immune system and inflammatory mediators. When we are stressed, cortisol will then stimulate physiological functions and then act on the hypothalamus and pituitary gland to suppress further release. If there is acute or chronic stress, which leads to higher cortisol levels, this can lead to higher blood pressure, weight gain, poor sleep among other responses.
Physiological effect vs pharmacological effect:
Corticosteroid medications can be prescribed for two purposes. These distinctions are important to know. The first is for physiological (maintenance, replacement) effect, which are the to maintain cortisol levels produced by healthy adrenal glands. If the adrenals are not able to produce enough cortisol, the levels will get too low, and the result is adrenal insufficiency. An example is Addison’s Disease. In this case, the treatment is to mimic the normal cortisol production and secretion. Hydrocortisone is one option that may be given to correct this deficiency.
Pharmacological effect is when high levels of corticosteroids are given to treat disorders unrelated to adrenocortical function. Examples of conditions include lupus, allergies, or asthma. In these cases, the treatment is for anti-inflammatory or immunosuppressant effects. Many conditions require short term treatment with corticosteroids such as exacerbation of ulcerative colitis, but other conditions may require long term therapy (Sealock & Seneviratne, 2021).
Endogenous corticosteroids regulate whole-body homeostasis with widespread effects:
- Metabolism: carbohydrate, protein and fat metabolism
- Supports skeletal muscle function
- Maintains vascular system
- Support neurological function: affects mood, sleep, behaviour
- Immunity and anti-inflammation
Corticosteroids
Corticosteroids are one of the most widely used medications. There is over 20 different formulations. They are used for numerous conditions and are available to administer in every route. All glucocorticoids do the same thing but differ in their onset of action, their potency, duration of action and amount of mineralocorticoid. They are often prescribed for their anti-inflammatory or immunosuppressive effects. Due to the fact that glucocorticoids are involved in almost every body system and impact the immune system, as well as carbohydrate, fat, and protein metabolism, adverse effects that are experienced when taking these medications, will affect every body system.
Indications of use
Corticosteroids are used for the management of various dermatologic, ophthalmologic, rheumatologic, pulmonary, hematologic, autoimmune diseases, shock, infectious and gastrointestinal (GI) disorders.
Exogenous corticosteroids are used for a variety of disorders such as:
- Endocrine disorders such as adrenocortical insufficiency
- Rheumatic disorders such as rheumatoid arthritis
- Collagen diseases such as systemic lupus erythematosus
- Dermatologic diseases such as severe psoriasis
- Allergic states such as contact dermatitis or drug hypersensitivity reactions
- Ophthalmic diseases such as optic neuritis
- Respiratory diseases such as asthma or COPD
- Neoplastic diseases such as leukemia
- Gastrointestinal diseases such as ulcerative colitis
- Nervous system diseases such as multiple sclerosis (Hodgens & Sharman, 2023).
In respiratory conditions, inhaled corticosteroids (ICS) are used as part of the general asthma management. But in acute exacerbations of chronic obstructive pulmonary disease (COPD) and severe asthma, oral or intravenous corticosteroids are used.
Prednisone is perhaps the most widely used of the systemic oral corticosteroids. It is generally used as an anti-inflammatory and immunosuppressive agent. Methylprednisolone is a commonly used injectable corticosteroid and similar in potency as prednisone.
Hydrocortisone is a commonly used topical cream for itching or eczema. It is obtained OTC in low doses or by prescription in higher doses. Hydrocortisone, given orally, is used to treat Addison’s disease or adrenal insufficiency (Daily Med, 2025). Of the corticosteroids, hydrocortisone has the highest mineralocorticoid content and the lowest glucocorticoid content. Along with hydrocortisone, fludrocortisone is sometimes also ordered. Fludrocortisone is a potent mineralocorticoid and is used for salt and water balance (Lui et al, 2013).
Example in Practice:
30-year-old client has asthma that is well-controlled with an inhaled corticosteroid, fluticasone, and a beta-2 adrenergic inhaler, salbutamol. Recently, she is experiencing more shortness of breath, dyspnea and fatigue. Due to the severity of her symptoms, she is prescribed prednisone for 10 days to help decrease the inflammation and overall improve her breathing.

Mechanism of Action
Glucocorticoids cause profound and varied metabolic effects as described in unit 10.2 Endocrine Disorders. They produce anti-inflammatory, immunosuppressive, protein and carbohydrate metabolic effects, skeletal muscle and central nervous system effects (Hodgens & Sharman, 2023).
Glucocorticoids exert their anti-inflammatory and immunosuppressive effects by binding to intracellular glucocorticoid receptors, which then modulates gene expression. This has an effect on anti-inflammatory proteins and also inhibits pro-inflammatory transcription factors resulting in a decrease in most inflammatory cytokine production. The gene inhibition also reduces inflammation by inhibiting the production of COX-2, thereby inhibiting prostaglandins and leukotrienes. The effects on protein, fat and glucose metabolism have the same effect by modulating enzyme synthesis (Chourpiliadis & Aeddula, 2023).

Nursing Considerations
Administration: Dosages are variable and tailored to the disease process and the individual. The lowest possible dose of corticosteroid should always be used. If taking low doses and for short period of time, then low risk of adverse effects.
Routes: parenteral, oral, inhaled, topical, injected (intramuscular, intra-articular, intradermal).
Highly protein bound, metabolized in the liver and renally excreted.
When discontinuing the med, orders will often be tapered down to avoid adrenal suppression.
Oral route: given before 0900 to closely mimic cortisol release from adrenals.
- Prednisone is the most frequently used oral formula, with dosages 5-60 mg/day. Usually ordered for short term basis, i.e. 2-4 weeks to avoid adverse effects.
- Usually taken with food or milk to decrease GI upset (Puckett, Patel, & Bokhari., 2025)
Topical route: Hydrocortisone is the most similar to naturally occurring cortisol. It is used topically for minor skin conditions OTC (0.5-1%) to more severe skin conditions, prescription (2% ointment). When applying topical ointment, use an applicator and spread on thinly. Do not cover the area. Low risk of systemic effects with localized topical route.
IV: methylprednisolone is given in emergent situations or if they are unable to tolerate prednisone by mouth (Hodgens & Sharman, 2023).
Refer to the table below for the differences between the differ glucocorticoid medications.
| Least potent to most potent | Uses | Comments |
| Hydrocortisone | Topical, oral, ophthalmic, ear
Adrenal insufficiency, skin conditions (i.e. psoriasis) |
Natural, short-acting. Most mineralocorticoid and least amount of glucocorticoid.
Sodium and water retention |
| Prednisone | Oral, medium potency. Onset one hour.
Wide variety of uses: COPD exacerbation, allergic conditions |
Synthetic, 4x stronger than cortisol (hydrocortisone).
|
| Methylprednisolone
Po, IV, IM |
Intravenous, higher potency.
Wide variety of uses: sepsis, anti-inflammatory, acute illness, etc |
Similar to prednisone in potency |
| Dexamethasone
po, IM, IV |
Oral, IV, highest potency
Used for rheumatoid arthritis, chemo nausea, palliative pain control, severe allergic rxns. Premature labor to promote fetal lung development. |
Most potent, ideally short-term use, long duration of action.
6x the potency of prednisone. |
Pediatrics:
Can be used with children, but risk of growth suppression if long term use (Lui et al, 2013). Growth will resume after prednisone therapy. Prior to therapy assess weight, height and nutritional assessment, reassess periodically.
Pregnancy:
There is a modest risk of cleft lip with systemic corticosteroid use. Other previous concerns such as low birth weight, preterm birth, preeclampsia has not been substantiated. For pregnant women, who need corticosteroid therapy for autoimmune diseases, for example, then the lowest dose for the shortest duration is advised (Bandoli et al, 2017).
Drug Interactions:
Corticosteroids interact with many drugs including macrolides, amphotericin B, bupropion, NSAIDs and estrogens. For example, corticosteroids taken with:
- NSAIDs, there is an increased risk of peptic ulcers.
- Warfarin, anticipate an increased anticoagulant effect 3 to 7 days following start of treatment. Check INRs more closely (Puckett, Patel, & Bokhari., 2025).
- Diuretics, risk of hypocalcaemia and hypokalemia.
Long term therapy: Despite their beneficial effects, long-term systemic use of corticosteroids is associated with well-known adverse events. The lowest possible dose is always ordered. Alternate day therapy is a corticosteroid dosing regimen in which twice the usual daily dose of corticoid is administered every other morning. The purpose of this mode of therapy is to minimize undesirable effects that can occur during long-term administration (Lui et al, 2013). Long-term corticosteroid therapy should never be stopped abruptly due to its effect on the hypothalamic-pituitary-adrenal (HPA) axis and potential adrenal suppression. Instead, the dose should be tapered to allow the body to resume natural production of adrenal hormone levels.
High doses with prolonged treatment avoided, unless condition is life-threatening or the potential to cause permanent disability.
Contraindicated with the following conditions, such as masked infections, fungal infections, myopathy, and glaucoma. May contribute to fluid retention, hypertension and hypokalemia (Puckett, Patel, & Bokhari, 2025).
Assessment prior to therapy:
Before initiating long-term systemic corticosteroid therapy, a thorough history and physical examination should be performed to assess for risk factors or pre-existing conditions that may potentially be exacerbated by glucocorticoid therapy, such as diabetes, dyslipidemia, cerebrovascular disease (CVD), GI disorders, affective disorders, or osteoporosis.
- Complete medication profile due to significant drug interactions with glucocorticoids.
- Vital signs, especially blood pressure
- Skin integrity: assess for any wounds to monitor wound healing
- Weight (due to risk of weight gain and fluid retention)
- Labs: complete blood count (CBC), blood glucose values, renal panel, lipid profile.
- Bone mineral density
- Assess for untreated infections, as corticosteroids are contraindicated in clients with untreated systemic infections.
Monitor:
Close monitoring for adverse effects is important especially for long term therapy.
- Blood glucose due to risk of hyperglycemia
- Adherence to medications
- Signs of infection due to immunosuppression
- Risk of myopathy. Assess for muscle weakness and atrophy which can develop over weeks to months. Muscle strength will resolve 3-4 weeks after therapy discontinued.
- Skin integrity: risk of abdominal striae which may be permanent. Thinning of the skin leading to skin tears. Delayed wound healing, assess any wounds.
- Cushingoid features: weight gain and redistribution of adipose tissue. Assess for facial fat (moon face), dorsocervical fat pad (buffalo hump) or truncal obesity.
- Electrolytes (hypokalemia, hyperglycemia)
- Risk of osteoporosis and fractures. Corticosteroids can impair bone mineralization and impair calcium absorption.
- Monitor for GI effects: will decrease mucous production and predispose for peptic ulcers. Assess for GI upset and black tarry stools.
Adverse/side effects
Adverse effects appear with both an average dose and cumulative duration, but most often with chronic use. If used more than 60 days, most clients have some adverse effects. Recall that corticosteroids have an effect on all body systems, so adverse effects are varied. Most common:
- Osteoporosis and fractures
- Cushingoid features: moon face, adipose fat deposit on upper back (buffalo hump)
- Diabetes and hyperglycemia
- Myopathy
- Glaucoma and cataracts
- Psychiatric conditions: psychosis, sleep disturbances, euphoria, mood swings, depression
- Poor wound healing
- Mask signs of infection
- Fragile skin that bruises and tears easily
- Peptic ulcers
(Hodgens & Sharman, 2023).
To avoid adverse effects, the lowest effective dose should be used for treatment. Monitor regularly all parameters described under ‘assessment’. Watch for adrenal suppression in clients who have been on therapy for greater than 2 weeks or in multiple short courses of high-dose therapy.
Risk of fractures: to avoid the risk of fractures, concurrent treatment with Alendronate, a bisphosphonates class of medication, is often used in addition to other osteoporosis preventative measures such as weight-bearing exercise and calcium/Vitamin D supplementation (Lui et al, 2013).
Adrenal insufficiency: Symptoms of adrenal insufficiency include weakness/fatigue, malaise, nausea, vomiting, diarrhea, abdominal pain, headache (usually in the morning), poor weight gain and/or growth in children, myalgia, arthralgia, psychiatric symptoms, hypotension, and hypoglycemia. If these symptoms occur, further lab work, such as an early morning cortisol test, should be performed (Lui et al, 2013).
Client Teaching
- Teach clients taking long-term prednisone therapy to never abruptly stop taking the medication and to report any adverse/side effects or new signs of infection.
- Glucocorticoid medication can cause immunosuppression, which makes it more difficult to detect signs of infection. Clients should seek advice from healthcare providers regarding vaccination administration while on glucocorticoids. Clients should report unusual swelling, weight gain, fatigue, bone pain, bruising, non-healing sores, visual and behavioral disturbances to the provider.
- Use of glucocorticoid therapy may cause an increase in blood glucose levels. If diabetic, anticipate an increase in anti-diabetic medications.
- Advise clients to consume diets that are high in protein, calcium, and potassium.
- Take oral corticosteroids with food to avoid GI upset.
(Adams et al, 2018; Puckett, Patel, & Bokhari., 2025)
Example in Practice 2:
A 25-year-old client has occasional eczema that flares up from time to time. She currently has a large reddened, scaley patch on both her elbows. She uses hydrocortisone ointment 0.5% that she has picked up OTC from the pharmacy. After a few days, the patches are getting itchier and reddened. She returns to the pharmacy, and they assess the areas. They prescribe Hydrocortisone 2.5% ointment. The pharmacist provides health teaching that includes to apply sparingly with an applicator and do not cover with a band-aid. Do not use more than 7 days and if it still persists, see their health care prescriber for further care.
Example in Practice 3:
A 70-year-old client has been diagnosed with a pancreatic tumour with metastasis to his bones. He is palliative. He has considerable pain and has been on hydromorphone. The physician has recently ordered dexamethasone as an adjunct analgesic. The nurse questions the use of dexamethasone for pain. What he learns is that it is ordered to decrease pain by decreasing inflammation (inhibits prostaglandin synthesis), reduces vascular permeability (prevents edema) and reduces nerve conduction (decreases neuropathic pain). Depending on how the client is doing with fluid overload, dexamethasone has the least amount of mineralocorticoid than the other options, so it will not cause more fluid retention. Dexamethasone can be given oral or SQ so a good option for a palliative client who can’t tolerate swallowing.

Glucocorticoid: Prednisone, Methylprednisolone, Hydrocortisone Medication Card
Now let’s take a closer look at the medication card for glucocorticoid medications. These example cards are intended to assist students to learn key points about each medication. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication. Basic information is outlined below.
Refer to the Comparing Corticosteroids table that provides further information of the different formulations of corticosteroids (AHFS, 2019; Bornstein et al, 2016; Hodgens & Sharman, 2023; Lui et al, 2019; Nieman et al, 2013).

Comparing Corticosteroid Medication Table
To help with comparing the medications and to learn important considerations for each medication, refer to the medication tables Chapter 10 Comparing Corticosteroid Medications table. This file is downloadable and editable, therefore easy to add information as needed. This table is not intended to replace current drug manuals or monographs prior to administration in the practice setting.
Clinical Reasoning and Decision-Making Activity
Case study 1: A client in a long-term care facility who has COPD receives prednisone 10 mg daily to help manage her respiratory status. Upon reviewing the client’s chart, the nurse notices that the client was diagnosed with osteoporosis in the past but is not currently receiving medications indicated for osteoporosis. Other health issues are type 2 diabetes mellitus and dementia. The nurse is concerned because the client requires assistance for mobility and is a high fall risk. The nurse plans to call the provider.
- What cues in the client’s medical history cause the nurse to be concerned about the risk for a fracture?
- What medication(s) may be prescribed concurrently with prednisone to reduce the risk for a fracture?
- What other client teaching can the nurse provide to help reduce the client’s risk for a fracture?
- Bedside glucose testing with sliding scale insulin is ordered for this client. Why is insulin ordered when the client has type 2 diabetes? What is the rationale for these orders?
- What cues would cause the nurse to contact the provider with the hypothesis that adrenal suppression is occurring?
Case study 2: A 54-year-old client has had bowel surgery and has become septic post-operatively. The nurse sees a new order for prednisone for this client. The nurse is concerned with giving prednisone to a client with a large abdominal wound.
- What is the nurse concerned about?
- The nurse prepares to give the prednisone in the morning. Why is the morning the best time to give prednisone? To avoid gastric irritation from prednisone, what additional med may be ordered for this client?
Case Study 3: A client with lymphoma is wondering why they are also ordered dexamethasone. Why are corticosteroids ordered to treat lymphoma?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 10: Endocrine System Medications: Part 1 Answer Key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
References
Adams, M., Urban, C., El-Hussein, M., Osuji, J. & King, S. (2018). Pharmacology for Nurses. A pathophysiological approach (2nd Canadian ed.). Pearson Canada Inc: Ontario.
American Society of Health-System Pharmacists (2018). Neomycin, Polymyxin, Bacitracin, and Hydrocortisone Topical. AHFS Patient Medication Information [Internet]. Bethesda (MD): American Society of Health-System Pharmacists, Inc.; c2019. https://medlineplus.gov/druginfo/meds/a601061.html ↵
Bandoli, G., Palmsten, K., Forbess Smith, C. & Chambers, C. (2017). A review of systemic corticosteroid use in pregnancy and the risk of select pregnancy and birth outcomes. Rheumatoid Disorders Clinic North America, Aug, 43(3), 489-502. doi: 10.1016/j.rdc.2017.04.013
Bornstein, S., Allolio, B., Arlt., W., Barthel., A., Don-Wauchope, A., Hammer, G., Husebye, E., Merke, D., Murad, M., Stratakis, C., & Tropy, D. (2016, February 1). Diagnosis and treatment of primary adrenal insufficiency: an endocrine society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 101(2). pp. 364-389. https://doi.org/10.1210/jc.2015-1710 ↵
Chourpiliadis, C. & Aeddula, N. (2023). Physiology, glucocorticoids. National Library of Medicine. StatPearls [Internet].Physiology, Glucocorticoids – StatPearls – NCBI Bookshelf
Hodgens, A. & Sharman, T. (2023). Corticosteroids. National Library of Medicine. StatPearls [Internet].
Liu, D., Ahmet, A., Ward, L., Krishnamoorthy, P., Mandelcorn, E., Leigh, R., Brown, J., Cohen, A., & Kim, H. (2013, August 15). A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy, Asthma & Clinical Immunology, 9(30). https://doi.org/10.1186/1710-1492-9-30 ↵
Nieman, L., Biller, B., Findling, J., Murad, M., Newell-Price, J., Savage, M, & Tabarin, A. (2015, August 1). Treatment of Cushing’s Syndrome: an endocrine clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 100(8). pp. 2807-2831. https://academic.oup.com/jcem/article/100/8/2807/2836065 ↵
Puckett, Y., Patel, P. & Bokhari, A. (2025). Prednisone. National Library of Medicine. StatPearls [Internet]. Prednisone – StatPearls – NCBI Bookshelf
Sealock, K. & Seneviratne, C. (2021). Lilley’s Pharmacology for Canadian Health Care Practice (4th ed.). Elsevier: Canada
Media Attributions
- Figure 10.3a Hypothalamus Pituitary Adrenal Axis. File: Basic HPA Axis.jpeg File:Basic HPA Axis.jpeg – Wikimedia Commons
- Figure 10.3b “Fluticasone.JPG” by James Heilman, MD is licensed under CC BY-SA 3.0 ↵
- Figure 10.3c “006035339lg Prednisone 20 MG Oral Tablet.jpg” by NLM is licensed under CC0 ↵
- Figure 10.3d “Methylprednisolone vial.jpg” by Intropin is licensed under CC BY 3.0 ↵

{kind=link}
{kind=link}
{kind=link}
{kind=link}