11.4 Insulin Therapy
Since the discovery of insulin in 1921-1922 by the Canadian researchers Frederick Banting and Charles Best, and with ongoing improvement in insulin therapies and overall diabetic management, type 1 diabetics can effectively manage their blood sugars and glycemic control.
Anti-Diabetic Medication Classes: Insulins
Because the hallmark of type 1 diabetes is absent or near-absent β-cell function, insulin treatment is essential for individuals with type 1 diabetes. Current evidence-based recommendations regarding pharmacological treatment of type 1 diabetes include:
- Most people with type 1 diabetes should be treated with multiple daily injections of prandial and basal insulin or continuous subcutaneous insulin infusion.
- Most individuals with type 1 diabetes should use rapid-acting insulin analogs to reduce hypoglycemia risk.
- Individuals with type 1 diabetes on prandial insulin doses should be educated on carbohydrate intake, premeal blood glucose levels, and anticipated physical activity.
- Individuals with type 1 diabetes who have been successfully using continuous subcutaneous insulin infusion should have continued access to this therapy after they turn 65 years of age.
Mechanism of Action
Insulin is an essential hormone that has a number of functions. It restores a client’s ability to metabolize fats and carbohydrates, it increases protein synthesis, it allows glucose transport into most cells (the brain and liver are exceptions) and promotes the conversion of glucose into glycogen in the liver and muscle.

Insulin acts directly by binding to the receptors on the plasma membranes of all cells. Once the insulin binds to the beta subunit of a cell, this initiates other actions. The glucose transporter in the cell allows the influx of glucose from the blood into the cell, thus reducing blood glucose levels. It also initiates other events such as glycogen synthesis, inhibits glucagon release, promotes lipogenesis, among other actions. Insulin acts like a key, helping glucose enter cells. If the pancreas does not produce insulin, such as with type 1 diabetics, the cellular uptake of glucose does not occur (Thota & Akbar, 2023).
In type 2 diabetes, the cells are resistant to the action of insulin. The pancreas will secrete more insulin to try to get the glucose into cells but eventually there is progressive beta-cell dysfunction, leading to a buildup of glucose in the blood.
All insulins have the same mechanism of action, that is, they lower blood glucose by stimulating peripheral glucose uptake by skeletal muscle and fat and by inhibiting hepatic glucose production.
Types of Insulin
Initially, insulin was prepared from cow or pig pancreas. Since the 1980s, insulin is genetically engineered to produce a synthetic human insulin. Normally, the pancreas secretes a steady stream of insulin called basal. This provides the background insulin needed to supply cells with glucose around the clock while preventing the release of excess glucose from the liver and excess fat from the adipose cells. When we eat, we need more insulin so a bolus amount of insulin is produced over the next few hours. Once carbohydrate absorption is complete, insulin levels decline. When we give insulin, we are mimicking this effect.
Insulins fall into different categories, based on their source, onset, and duration of action:
- Bolus (prandial) insulin: used with meals
- rapid-acting (insulin lispro, insulin aspart, or insulin glulisine)
- short-acting (regular insulin)
- Basal insulins:
- Intermediate-acting (insulin isophane suspension [NPH])
- Long-acting (insulin glargine or insulin detemir)
There are also pre-mixed insulins, such as premixed regular insulin Humulin 30/70 and Novolin 30/70 or 40/60.

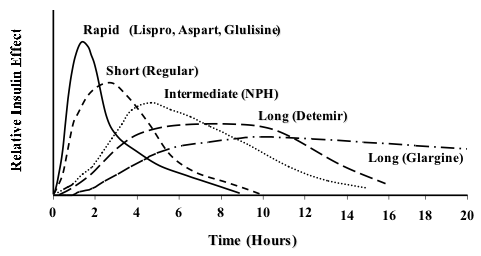
Figure 11.4b Types of insulin and duration of action (M Komorniczak/Wikimedia Commons) CC BY-SA 3.0
Insulin Facts
- The goal of insulin therapy is to mimic both the normal transient insulin secretion following food intake and the basal between-meal insulin levels as close as possible (Diabetes Canada, 2026).
- Insulin can be used alone or in combination with other types of insulin to stimulate normal insulin secretion.
- All type 1 diabetic clients will be on a basal insulin and a bolus insulin. Type 2 diabetics may also be on insulin if they have significant risk factors such as coronary artery disease or other vascular conditions or become more resistant to insulin (Thota & Akbar, 2023).
Therapeutic Effects:
- Regulates the movement of glucose from blood into cells
- Insulin lowers blood glucose by stimulating peripheral glucose uptake primarily by skeletal muscle cells and fat, and by inhibiting glucose production and release by the liver
- Maintain serum blood glucose in normal range and achieve individualized target level of A1C (often 7%)
Adverse effects:
- All insulins have risk of hypoglycemia or hyperglycemia
- Ensure correct injection technique to avoid lipodystrophy, bruising and pain at the site.
Depending on the duration of action, insulin is categorized as rapid acting, short-acting, intermediate-acting, and long-acting. In the table below is a comparison of the different insulins.
Comparing Insulins
| Class | Prototypes | Onset/Peak/Duration | Administration Considerations | Other |
| Rapid-Acting Insulin
(Prandial) |
insulin lispro (Humalog)
insulin aspart (Novolog) inhaled insulin (Afrezza) |
Onset: 15-30 minutes
Peak effect: 1-3 hours Duration: 3 – 5 hours |
· Administer within 15 minutes before a meal or immediately after a meal.
· Afrezza is contraindicated in patients with asthma or COPD
Ensure the client plans to eat their meal |
Afreeza can cause bronchospasm in COPD
|
| Short-Acting Insulin
(Prandial) |
Humulin R | Onset: 30 minutes
Peak effect: 3 hours Duration: 8 hours |
· Administer 30 minutes before a meal | |
| Intermediate-Acting Insulin
(Basal) |
Humulin N
Novolin N |
Onset: 1-2 hours
Peak effect: 6 hours (range 2.8-13 hours) Duration: up to 24 hours |
· Administer once or twice daily
· SQ only · Gently roll or invert vial/pen several times to re-suspend the insulin before administration · Do not mix with other insulin |
|
| Combination: Intermediate-Acting/Rapid-Acting
|
Humalog Mix 50/50
Humalog Mix 75/25 Novolog Mix 70/30 *First number is % intermediate-acting insulin, second number is % rapid-acting |
Onset: 15-30 minutes
Peak effect: 50/50: 1-5 hours Duration: 11-22 hours |
· Administer twice daily, 15 minutes before a meal or immediately after a meal
· Only administer subcutaneously · Gently roll or invert vial/pen several times to re-suspend the insulin before administration |
|
| Combination: Intermediate-Acting/Short-Acting
|
Humulin 70/30
Novolin 70/30 |
Onset: 30-90 minutes
Peak effect: 1.5-6.5 hours Duration: 18-24 hours |
· Administer twice daily, 30-45 minutes before a meal
· SQ only · Gently roll or invert vial/pen several times to re-suspend the insulin before administration · Do not mix with other insulins |
|
| Long-Acting Insulin
(basal) |
insulin glargine (Lantus)
insulin detemir (Levemir) |
Onset: 3-4 hours
Peak effect: none Duration: >24 hours |
· Administer once daily (sometimes dose is split and administered twice daily)
· SQ only · Do not mix with other insulins |
|
| Hyperglycemic agent
Treats severe hypoglycemia |
Glucagon | SQ, IM, IV or inhaled
IVP: onset is 5-30 minutes IM: 30 min for peak glucose response Duration of action 90 minutes GlucPen SQ |
· Supplementary carbohydrate should be given as soon as possible, especially to a pediatric patient
· Used to reverse hypoglycemic episode if oral administration of sugar is not appropriate or effective. safe with peds SE: nausea, nasal congestion, headache, abd pain, dizziness |
Risk of hyperglycemia
For severe hypoglycemia not responsive to administration of simple CHOs or if oral administration of CHOs is not possible. |
Note: All onset, peak and duration times are approximate and may differ depending on reference (Diabetes Canada, 2026)
Comparing Insulins
Rapid-Acting Insulin
Rapid-acting insulins include insulin lispro (Humalog) and insulin aspart (Novolog) and are also available via inhalation (Afrezza). See Figure 11.4c for an image of Novolog insulin

Indications: Rapid-acting insulins are also called prandial insulins because they are administered with meals to mimic the effects of endogenous insulin release when food is eaten. Dosages of rapid-acting insulin are individualized based on carbohydrate intake, premeal glucose levels, and anticipated activity.
Administration Considerations
Concentration differences: Lispro Humalog-100 (100 units per ml) and Humalog-200 (200 units per ml) are both rapid-acting insulins.
- Humalog-100:
- SQ or IV continuous injection.
- can be mixed with NPH insulin. It is available in vials, KwikPens and cartridges.
- Humalog-200:
- should not be mixed with other insulins.
- SQ, only available in KwikPens.
- twice as concentrated as Humalog-100, used for clients who require high levels of insulin.
Inspect insulin visually before use. It should appear clear and colorless; do not use if particulate matter or coloration is seen.
Administer subcutaneously into the abdominal area, thigh, or deltoid, and rotate injection sites within the same region from one injection to the next to reduce the risk of lipodystrophy.
Because of the rapid onset of insulin lispro and insulin aspart and the potential for hypoglycemia, these insulins should be administered within 15 minutes before or right after eating a meal. Peak serum levels are seen 30 to 90 minutes after dosing.
Inhaled insulin enters the bloodstream within 1-15 minutes and peaks in 30-60 minutes. Inhaled insulin is contraindicated in clients with chronic lung disease such as asthma or COPD. May cause acute bronchoconstriction.
Adverse effects of all insulins include hypoglycemia and hypokalemia.
Short-Acting Insulin
Short-acting insulins include regular insulin with a brand name of Humulin R or Novolin R. A concentrated formulation of Humulin R u-500 is also available.
Indications
Short-acting insulins are given with meals to mimic the effects of endogenous insulin release when food is eaten. Dosages of short-acting insulin are individualized based on carbohydrate intake, premeal glucose levels, and anticipated activity levels.
Administration Considerations
Administer: SQ or IV.
- Regular insulin is generally administered subcutaneously. It can be given intravenously, either intermittent or continuous infusion, under close supervision of blood glucose and potassium levels.
- It is available in vials and insulin pens.
Inspect insulin visually before use. It should appear clear and colorless; do not use if particulate matter or coloration is seen.
Administer subcutaneously into the abdominal area, thigh, or deltoid, and rotate injection sites within the same region from one injection to the next to reduce the risk of lipodystrophy. Subcutaneous doses should be administered approximately 30 minutes before meals because this is the typical onset of action. Peak effects occur in 3 hours with a duration of 8 hours. Do not mix with insulin preparations other than NPH.
Humulin R u-500 should only be administered in u-500 insulin syringes to avoid dosage calculation errors.
Intermediate-Acting Insulin
NPH insulin, also known as isophane insulin, is an intermediate–acting insulin. Brand names include Humulin-N or Novolin-N. Mixtures of short- and intermediate-acting insulin include Humulin 70/30 or Novolin 70/30.
Indications
Intermediate insulins are administered once or twice daily to mimic endogenous basal insulin levels.
Administration
NPH insulin is a white and cloudy suspension. Gently roll or invert vial/pen several times to re-suspend the insulin before administration. It should only be administered subcutaneously. It may be mixed with rapid-acting or short-acting insulins, but those insulins should be drawn into the syringe before the NPH is added.
Administer subcutaneously into the abdominal area, thigh, or deltoid, and rotate injection sites within the same region from one injection to the next to reduce the risk of lipodystrophy.
The onset of action and peak are affected by the site of injection, physical activity level, and other variables but the median peak level occurs in 4 hours. See Figure 11.4e for an image of Novolin-N (a cloudy insulin) that can be mixed with Novolin R (a clear insulin).

Mixed medications such as Humulin 70/30 should be administered subcutaneously approximately 30 minutes before a meal. They are typically dosed twice daily (with each dose intended to cover 2 meals or a meal and a snack).
Unopened vials should be stored in the refrigerator until the expiration date. Opened vials should be labelled with the open date and stored in the refrigerator for up to 28-42 days (depending on the formulation/insulin type) and then discarded. Unopened pens should be stored in the refrigerator until the expiration date. Used pens should be stored at room temperature, but kept away from heat and light, for up to 10-28 days (depending on the formulation/insulin type) and then discarded.
Long-Acting Insulin
Insulin glargine (Lantus) and insulin detemir (Levemir) are long-acting insulins given once or twice daily. See Figure 11.4f for an image of a levemir insulin pen.

Figure 11.4e Vial used for Levemir insulin pen. (Wesalius/Insulin analog 100 IU-1ml penfill levemir yellow background.jpg/Wikimedia Commons). CC BY 4.0 ↵
Indications
Long-acting insulins are given once or twice daily. In type 1 diabetics, long-acting insulin should be used concomitantly with rapid- or short-acting insulin at mealtimes.
Administration
Long-acting insulin has a relatively constant concentration/time profile over 24 hours with no pronounced peak in comparison to NPH insulin. It should only be administered subcutaneously and is available in vials and insulin pens.
Inspect insulin visually before use. It should appear clear and colorless; do not use if particulate matter or coloration is seen. Administer subcutaneously into the abdominal area, thigh, or deltoid, and rotate injection sites within the same region from one injection to the next to reduce the risk of lipodystrophy.
Dosing and Administration
Dosing is highly individualized for each client. Insulin requirements can be estimated based on weight, with typical doses ranging from 0.4 to 1.0 units/kg/day. Higher amounts are required during puberty, pregnancy, and medical illness. Physiologic insulin secretion varies with glycemia, meal size, and tissue demands for glucose. To approach this variability in people using insulin treatment, strategies have evolved to adjust meal-time doses based on predicted needs. Thus, education of clients on how to adjust insulin to account for carbohydrate intake, premeal glucose levels, and anticipated activity is important. Ensuring that clients and/or caregivers understand correct insulin injection technique is also important to optimize glucose control and insulin use safety (American Diabetes Association, 2019).
Insulin administration is typically given by subcutaneous route. It is the preferred route, easy to administer and can be given by insulin syringes, pens and pumps (See figure 11.4f). it can be injected into almost any fatty area under the skin, but typically the back of the upper arm, abdomen, or thigh. The insulin absorbs the fastest when given in the abdomen. It is important to rotate injection sites to avoid complications such lipodystrophy.
Intravenous route: It can be given intravenous which may be seen in clients who are in the hospital and who need a very tight glycemic control. For example, clients with sepsis, diabetic ketoacidosis, severe hyperkalemia, or beta-blocker toxicity (Thota & Akbar, 2023).
Other routes: It can also be given intramuscular, although rarely used. Recently, an inhalable insulin has been developed, where it passes through the lungs into the bloodstream and provides a rapid onset of 12 minutes (Thota & Akbar, 2023). Insulin is never given orally due to low bioavailability from the acidic stomach environment and the various proteolytic enzymes in the gastrointestinal tract that break down the insulin peptide structure, making it inactive. It is also a large molecule, unable to be absorbed in the intestinal lumen (Limenh, 2024).
Insulin Delivery

Insulin is delivered subcutaneously to respond precisely to blood glucose levels. The ideal device for a client should be economically feasible and easy to use to promote long-term adherence.
Insulin Syringe
Insulin syringes require clients to manually fill insulin from a vial and subcutaneously inject the required dose. Insulin syringes are the lowest cost of the available devices. Only specific insulin syringes can be used for insulin and are typically identified with an orange cap.
Insulin Pens
Insulin pens are often used in inpatient settings, as well as for self-administration at home, to facilitate safe and accurate self-administration of insulin. See Figure 11.4g for an image of an insulin pen. According to the ISMP, insulin pens offer several advantages over vials beyond dosing accuracy, convenience, and ease of use:
- Each pen is already labeled by the manufacturer with the product name and product barcode (whereas syringes of insulin prepared on the client care unit from vials run the risk of being unlabeled).
- Each pen can be individually labeled with the client’s name (and ideally with a client-specific barcode).
- The pen provides the client’s insulin in a form ready for administration.
- The pen lessens nursing time needed to prepare and administer insulin.
- Insulin pens reduce medication waste that can occur when dispensing 10 mL-sized insulin vials for each client.
However, improper sharing of insulin pens among multiple clients has exposed clients to bloodborne pathogens. Insulin pens should never be reused for multiple clients; even if the needle is changed between clients, there can still be body fluid exposure (Institute for Safe Medication Practices, 2017).
.jpg\" by Wesalius is licensed under CC BY 4.0")
Insulin Jet Injectors
Jet injectors are needle-less devices that produce high-pressure air jets which deliver a stream of vaporized insulin through the skin. With a jet injector, the insulin is delivered by pressing a button on the device. It is a beneficial option as it minimizes skin trauma or bruising and may enhance early insulin absorption and glycemic control. It is also beneficial for clients with severe insulin induced lipoatrophy or those with needle phobias. Drawbacks to the jet injector is cost and is larger in size (Wang et al, 2021).
Insulin Pumps
Insulin pumps are small, computerized devices about the size of a pager that continuously infuses insulin from a reservoir in the device to a subcutaneous catheter that is inserted into the client’s abdomen, hip, arm or leg (Wang et al, 2021). Similar to a combined basal-bolus regimen that is attained by injecting long and rapid acting insulin, the pump is designed to mimic the human pancreas. The delivery of insulin continuously and in response to meal times, promotes normoglycemic levels.
Continuous Glucose Monitors: The arrival of continuous glucose monitors to clinical practice has been proven to reduce nocturnal hypoglycemia in people using insulin pumps with glucose sensors due to automatic suspension of insulin delivery at a preset glucose level. Health Canada has also approved the first hybrid closed-loop pump system (BC Diabetes Association, 2020. A hybrid closed-loop pump system automatically adjusts basal insulin delivery every 5 minutes based on sensor glucose to maintain blood glucose levels as close to a specific target as possible (Weaver & Hirsch, 2018).
Other devices
To further promote client adherence, improve efficacy and glycemic outcomes, as well as being affordable, researchers continue to explore new delivery systems. Ongoing research to expand delivery routes include inhaled, buccal, nasal and transdermal delivery devices. These under-developing routes and the associated devices have been shown to be convenient to use with high patient compliance, but so far lack in the ability to be glucose-responsive (Wang et al, 2021).
The cost of insulin and insulin delivery devices can be a barrier to many clients. Further, the cost of blood glucose monitoring kits and lancets can all add up to thousands of dollars per year. Canada now covers the cost of insulin and insulin pens in most provinces, and it also covers many oral anti-diabetic medications (Health Canada, 2024). There are individual differences between provinces with exact coverage.
High-Alert Medication and Prevention of Errors
Insulin is a high-alert medication that can be associated with significant client harm when used in error. A variety of error types have been associated with insulin therapy, including administration of the wrong insulin product, improper dosing (underdosing and overdosing), dose omissions, incorrect use of insulin delivery devices, wrong route (intramuscular versus subcutaneous), and improper monitoring.
Many errors result in serious hypoglycemia or hyperglycemia. Hypoglycemia is often caused by a failure to adjust insulin therapy in response to a reduction in nutritional intake or an excessive insulin dose stemming from a prescribing or dose measurement error.
Other factors that contribute to serious hypoglycemia include inappropriate timing of insulin doses with food intake, creatinine clearance, body weight, changes in medications that affect blood glucose levels, poor communication during client transfer to different care teams, and poor coordination of blood glucose testing with insulin administration at meal time.
TALL MAN lettering to reduce med errors: One strategy for look-alike medications such as Humalog and Humalin is tall man lettering on the label. Tall man lettering describes a method for differentiating the unique letter characters of similar drug names known to be confused with one another, such as HumaLOG and HumaLIN.
ISMP recommends the following safe practice guidelines for the administration of insulin by the nurse:
- A coordinated process is developed to ensure timely blood glucose checks and administration of prandial insulin in conjunction with meal delivery.
- Verbal communication of point-of-care blood glucose value results are avoided as much as possible and are NEVER routinely used as the only source of information when determining insulin doses.
- Appropriately label all clinician-prepared syringes of subcutaneous insulin, unless the medication is prepared at the client’s bedside and is immediately administered to the client without any break in the process.
- Prior to subcutaneous insulin administration, the practitioner:
- Confirms that there is an appropriate indication
- Assesses the client’s most current blood glucose value
- Assesses the client for symptoms of hypoglycemia
- Informs the client of their most current blood glucose level
- Informs the client of their dose, the full name of the product, and the insulin’s intended action
- Insulin pens:
- An individual insulin pen is never used for more than one client.
- Barcode scanning is used to verify that a client-specific pen is used to administer the correct insulin to the correct client.
- Client-specific insulin pens are stored on clinical units in a manner that prevents their inadvertent use on more than one client.
There are several different types of insulins that vary in terms of onset, peak, and duration. It is critical for the nurse to be knowledgeable of these differences to help prevent episodes of hypoglycemia due to mismatched administration of insulin with food intake.
Transitions of care and discharging client to home:
Prior to transitions of care, a process is in place to ensure that clients will have the necessary prescriptions, supplies, a follow-up care plan, and printed instructions for all prescribed insulin and blood glucose monitoring.
Clients discharged on insulin are assessed for understanding of their self-management, including:
-
- Demonstration of proper dose measurement and self-administration using the same administration device that will be used at home (e.g., vial and syringe, pen, pump)
- Correct monitoring of blood glucose values
- The signs and symptoms of hyper- and hypoglycemia and how to respond if these symptoms occur
- Common types of errors possible with their insulin therapy and how to prevent or detect these errors
- The importance of regular follow-up with their primary care provider/specialist, including the date of their next appointment
- Clients who self-administer concentrated U-500 insulin using a vial and syringe are taught to use only a U-500 syringe and communicate their doses in terms of the name and concentration of the insulin and the actual dose in units using only the U-500 syringe[1]
Client education that includes lifestyle modifications that improve health should be emphasized, along with any pharmacologic therapy. Lifestyle modifications include healthy food choices to stabilize blood glucose levels, as well as daily exercise (Diabetes Canada, 2026).
General Considerations for Insulin therapy:
- Review orders closely because they may include more than one type of insulin, such as basal and bolus insulins.
- Always read drug labelling closely as there are several types of dosages and formulations.
- See agency policies and ISMP guidelines for safe administration of insulin.
- Closely monitor blood glucose levels before each meal and before insulin administration
- Ensure client is ready to eat if giving rapid or short acting insulin. If blood sugar is low or if client not eating, consider holding short acting or rapid acting insulin.
- Assess for signs of hypoglycemia and intervene appropriately. See unit 11.3 for more information on managing hypoglycemia. Hypoglycemia is defined as a blood glucose level below 4.0 mmol/L; severe hypoglycemia refers to a blood glucose level below 2.8 mmol/L.
- Ensure proper technique when giving insulin. When administering, after inserting the pen count to 5 before removing the needle.
- Rotate sights to avoid lipodystrophy
- Refrigerate insulin unopened vials. Keep out of fridge one month. Cold insulin can be irritating to tissues.
- General therapeutic effects: Maintain serum blood glucose in normal range and achieve individualized target level of A1C (often 7%)
Adverse/Side Effects of Insulin
Hypoglycemia is a common side effect. Closely monitor for signs of hypoglycemia, such as sweating, tachycardia, nausea, tremor and confusion. Clients who have been type 1 diabetic for a long time, may have only subtle symptoms.
Lipodystrophy is a disorder of adipose tissue due to repeated injections into the same site, leading to damage to the subcutaneous tissue. It is one of the most common complications. It is reported to be as high as 45% with type 1 diabetics (Gentile et al, 2016). It can present as lipohypertrophy or lipoatrophy.
- Lipohypertrophy is a thickened rubbery tissue swelling which is often firm or lumpy. It is caused by repeated injections to the same site with insulin. The insulin molecule has strong growth-promoting capabilities and injecting into the same area repeatedly can cause the lump.
- Lipoatrophy is a retracted scar on the skin that often large and deep.
- Lipodystrophy can be avoided with proper injection technique such as rotating sites. Injecting into these sites leads to poor glycemic control as the insulin is not properly absorbed (Gentile et al, 2016).
Pain at the injection site and bruising are also commonly seen (Thota & Akbar, 2023).
Drug Interactions
Some medications can cause lower blood glucose readings, while others can increase blood sugar levels. For clients who are started on new medications, ensure to check drug information or contact the pharmacist if closer blood glucose monitoring is required or if insulin or oral anti-diabetic med adjustments are required.
Drugs that cause hypoglycemia: sulfa antibiotics, alcohol, monoamine oxidase inhibitor antidepressants, and some herbal remedies such as ginseng and garlic.
Drug that cause hyperglycemia: corticosteroids block the entry of glucose into the muscle and fat tissues by preventing the glucose-transport proteins in the cells of those tissues from reaching the cell membrane. They also stimulate the production of glucose and increase insulin resistance. As such, clients on corticosteroids, like prednisone or dexamethasone, will require closer glucose monitoring and higher insulin needs.
Sympathomimetics (i.e. epinephrine) may increase insulin requirements by stimulating glycogenolysis, lipolysis, and inhibiting insulin secretion. Beta blockers, such as propranolol, can reduce insulin secretion, and can impair insulin-stimulated glucose uptake, leading to possible hyperglycemia in some clients. Beta-blockers can also mask the signs of hypoglycemia, such as tachycardia, which is an early cue of low blood sugar levels (May & Schindler, 2016).
Glucagon
Glucagon is indicated as a treatment for severe hypoglycemia (low blood sugar), which may occur in clients with diabetes mellitus. Glucagon injection is used for clients who are unable to safely swallow carbohydrates to treat hypoglycemia due to the effects of hypoglycemia or other medical conditions.
Mechanism of Action
Glucagon increases blood glucose concentration during an episode of hypoglycemia. Glucagon acts only on liver glycogen, converting it to glucose. Glucagon administered through a parenteral route relaxes smooth muscle of the stomach, duodenum, small bowel, and colon (Daily Med, 2021). Glucagon is not effective in treating hypoglycemia if there is insufficient liver glycogen available, such as with starvation, adrenal insufficiency or chronic hypoglycemia. In these cases, treat the hypoglycemia with glucose.
Indications
Glucagon is indicated as a treatment for severe hypoglycemia (low blood sugar), which may occur in clients with diabetes mellitus. Glucagon injection is used for clients who are unable to safely swallow carbohydrates to treat hypoglycemia due to the effects of hypoglycemia or other medical conditions.

Administration Considerations
Glucagon may be administered subcutaneously, intramuscularly, or intravenously. Peak glucose levels occur within 13-20 minutes of SQ or IM injection. It may cause nausea or vomiting.
Client Teaching
Clients with type 1 diabetes may have less of an increase in blood glucose levels compared with a stable type 2 client, so a supplementary carbohydrate should be given as soon as possible, especially to a pediatric client (Daily Med, 2021).
Comparing Insulin Medications Table
Now let’s take a closer look at the Comparing Insulins Medications table (Daily Med, 2023). This table is intended to consolidate the information about each insulin but it is also editable for you to add information that helps you with learning about each medication. As information with medications is always changing, refer to a drug reference or monograph.
Click on the link for the downloadable and editable copy: Comparing Insulin Table 2026
Media Attributions
- Figure 11.4a Effect of insulin on glucose uptake and metabolism by Meiquer on Wikimedia Commons is used under the CC BY-SA 3.0 license.
- Figure 11.4b Types of Insulin and their duration of action. Insulin_short-intermediate-long_acting.png https://upload.wikimedia.org/wikipedia/commons/c/cd/Insulin_short-intermediate-long_acting.png
- Figure 11.4c for an image of Novolog insulin. Free Images : medicine, glass bottle, medical 4504×3001 – – 197979 – Free stock photos – PxHere Alan Levine/PXHere) CC BY-SA 2.0
- Figure 11.4d Comparison of Novolin-N (a cloudy insulin) that can be mixed with Novolin-R (a clear insulin). The Gift of Life | These insulins are what give me the Gift … | Flickr “The Gift of Life” by Melissa Johnson is licensed under CC BY 2.0 ↵
- Figure 11.4e Image of a levemir insulin pen. (Wesalius/Insulin analog 100 IU-1ml penfill levemir yellow background.jpg/Wikimedia Commons). CC BY 4.0 ↵
- Figure 11.4f Diagram depicting insulin delivery devices, such as insulin syringe, insulin pen, jet injector and insulin pump. By BruceBlaus – Own work/, http://commons.wikimedia.org/wiki/File:Insulin_Delivery_Devices_(hy).png/Wikimedia Commons). CC BY-SA 4.0,
- Figure 11.4g Insulin Pen Human insulin 100 IU-1ml pen yellow background (02).jpg” by Wesalius is licensed under CC BY 4.0. ↵https://commons.wikimedia.org/wiki/File:Human_insulin_100_IU-1ml_pen_yellow_background_(02).jpg)
- Figure 11.4h Emergency glucagon kit. “Glucagon emergency rescue kit.JPG” by mbbradford is licensed under CC0 ↵
References
American Diabetes Association (2019). Older adults: Standards of Medical Care in Diabetes—2019. Diabetes Care 42(S1). https://doi.org/10.2337/dc19-S012 ↵
BC Diabetes Association, (2020). Diabetes research, advocacy, education, support – Diabetes Canada
Diabetes Canada (2026). Diabetes research, advocacy, education, support – Diabetes Canada
Daily Med (2023). This work is a derivative of Daily Med by U.S. National Library of Medicine in the public domain. ↵
Daily Med (2021). Glucagon. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=8cc40354-b5ac-45b6-a211-93b44444f2a3
Daily Med (2023). Insulin, Aspart. DailyMed – INSULIN ASPART injection, solution
Gentile, S., Strollo, F. & Ceriello, A. (2016). Lipodystrophy in Insulin-Treated Subjects and Other Injection-Site Skin Reactions: Are We Sure Everything is Clear? Diabetes Therapy, 7(3), 401-409. doi: 10.1007/s13300-016-0187-6PMCID: PMC5014793 PMID: 27456528
Health Canada (2024). Universal access to diabetes medications, and diabetes device fund for devices and supplies. Government of Canada. https://www.canada.ca/en/health-canada/news/2024/02/universal-access-to-diabetes-medications-and-diabetes-device-fund-for-devices-and-supplies.html
Institute for Safe Medication Practices. (2017). ISMP Guidelines for Optimizing Safe Subcutaneous Insulin Use in Adults. https://www.ismp.org/sites/default/files/attachments/2017-11/ISMP138-Insulin%20Guideline-051517-2-WEB.pdf ↵
Limenh, L. (2024). A review on oral novel delivery systems of insulin through the novel delivery system formulations: A review. SAGE Open Medicine. Jan 18;12:20503121231225319. doi: 10.1177/20503121231225319
May, M. & Schindler, C. (2016). Clinically and pharmacologically relevant interactions of antidiabetic drugs. Therapeutic Advances in Endocrine Metabolism. Apr; 7 (2):69-83. doi: 10.1177/2042018816638050. Epub PMID: 27092232; PMCID: PMC4821002.
Thota, S. & Akbar, A. (2023). Insulin. National Library of Medicine. StatPearls [Internet]. Treasure island (Fl). StatPearls Publishing.
Wang, Z., Wang, J., Kahkoska, A., & Buse, J. (2021). Developing Insulin Delivery Devices with Glucose Responsiveness. Trends Pharmacology Science, 42(1): 31–44. doi:10.1016/j.tips.2020.11.002.
Weaver, H., Hirsch, I (2018, June 6). The Hybrid Closed Loop System: Evolution and Practical Applications. Diabetes Technology & Therapeutics 20(S2). https://www.liebertpub.com/doi/10.1089/dia.2018.0091. ↵
- Institute for Safe Medication Practices. (2017). ISMP Guidelines for Optimizing Safe Subcutaneous Insulin Use in Adults. https://www.ismp.org/sites/default/files/attachments/2017-11/ISMP138-Insulin%20Guideline-051517-2-WEB.pdf ↵

{kind=link}
.png){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}