7.7 Antianginal Drugs
Antianginal drugs are used to treat angina pectoris. Angina is chest pain caused by an imbalance between the oxygen needs of the myocardium and the ability to deliver oxygen supply from inadequate blood flow. This can lead to hypoxia of the cardiac tissue. Angina can be chronic ischemic pain caused by atherosclerosis in coronary artery disease or acute ischemic pain caused by a myocardial infarction.
The overall goal is to reduce the intensity and frequency of attacks. Antianginals increase blood flow to the heart or decrease oxygen demand by the heart. Recall that there are three types of angina: stable, unstable and variant. Treatment looks a bit different for each type of angina. All drugs primarily only provide symptom relief; they do not fix the underlying issue (Burchum Rosenjack & Rosenthal, 2019).
Stable angina: exertional angina
- Nitrates: vasodilate coronary arteries and veins, decrease oxygen demand
- Beta blockers: decrease heart rate and contractility, decrease oxygen demand
- Calcium channel blockers: dilate arterioles, decrease afterload. Non-diphenhydramine’s also decrease heart rate and contractility.
Unstable angina: medical emergency from severe coronary artery disease
- Anti-ischemic therapy consists of nitroglycerin, beta blockers, oxygen if hypoxia or respiratory distress, morphine IV, and ACE inhibitors.
- Anti-platelet therapy consists of aspirin, clopidogrel and ticagrelor.
- Abciximab if angioplasty planned
- Eptifibatide or tirofiban if no angioplasty. Both meds are antiplatelet glycoprotein IIb/IIIa inhibitors
- Anticoagulant therapy – LMWH or direct thrombin inhibitors or unfractionated heparin IV
Variant angina (vasospastic or Prinzmetal)
- Calcium channel blockers and nitrates. Both increase coronary oxygen supply by relaxing the coronary artery spasm.
In this unit, we will be focusing on Organic Nitrates.
Nitrates
Nitroglycerin is the drug of choice for relieving acute angina. Since it was discovered in 1857, it has been the main drug for angina due to being fast, effective and inexpensive. It causes vasodilation of blood vessels and causes the dilation of coronary vessels. Nitroglycerin is the most common nitrate, but there is also isosorbide dinitrate and nitroprusside. Medications in this class can be used for acute anginal attacks or for long term therapy (Adams et al, 2018). It comes in various forms from oral, sublingual, intravenous, topical and transdermal.
Mechanism of Action
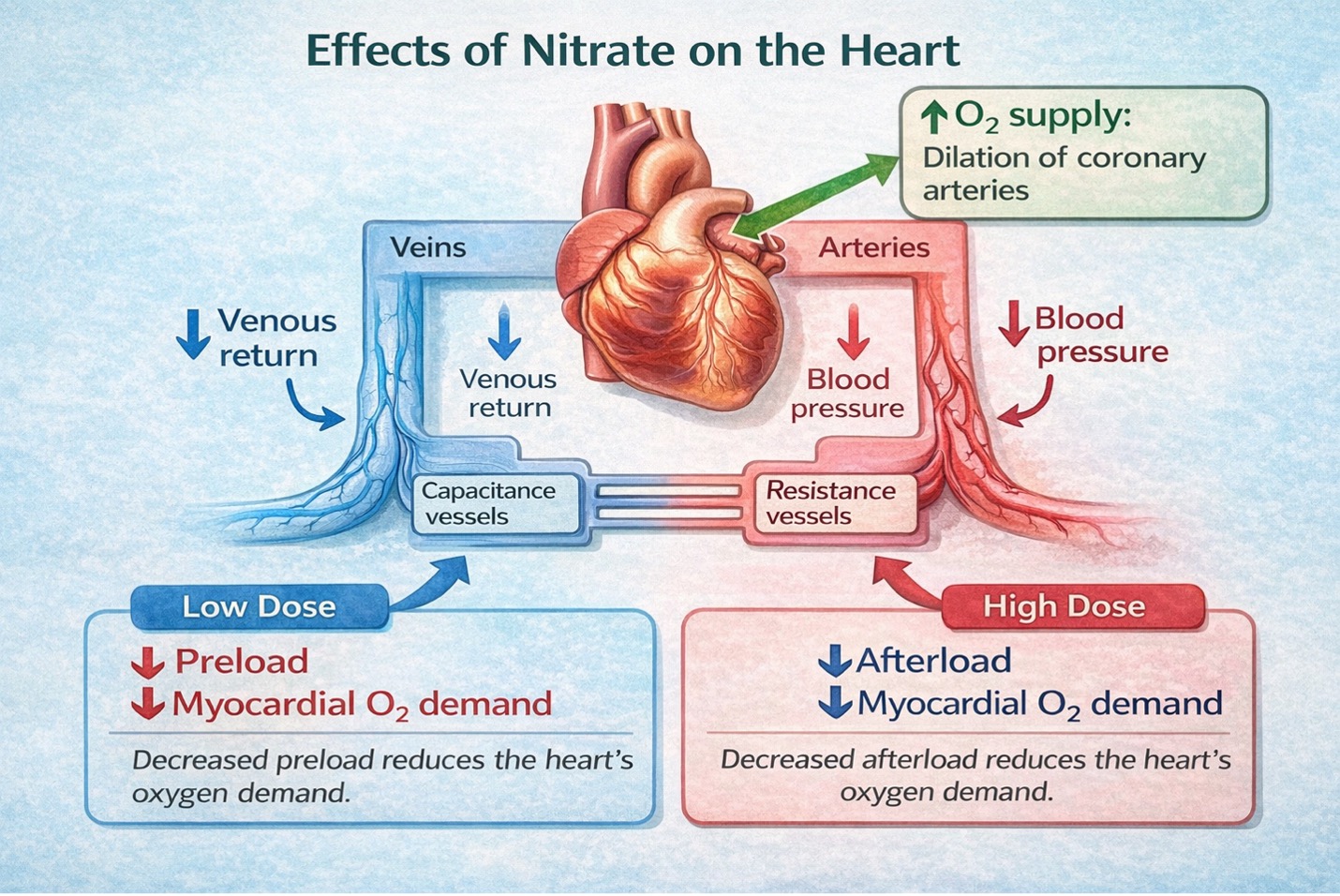
Nitrates work by increasing the release of nitric oxide, which then activates a series of chemical events resulting in the relaxation of the vascular smooth muscle, leading to vasodilation and angina relief. It acts primarily on the veins with minimal dilation of arterioles. With venous dilation, the amount of blood returning to the heart (preload) is reduced. With a lower volume of blood in the chambers, cardiac output is decreased and the workload of the heart is reduced. This leads to a lower myocardial oxygen demand. To a lesser extent, nitro also dilates coronary arteries allowing more blood flow to the myocardium (Adams et al, 2018).
Indications for Use
Nitroglycerin is used to relieve angina due to coronary artery disease, during times of an acute attack, or prophylactically. They are also used for arterial hypertension and heart failure. Off label, it is used topically for anal fissures to increase blood flow to the area and promote healing.
Note: Nitroprusside is a nitric oxide donor and used for hypertensive crisis or cardiogenic shock to rapidly lower BP, afterload and preload. It is given intravenously.
Isosorbide is used prophylactically to prevent angina pain or for heart failure with a low ejection fraction. It works more slowly than nitroglycerin so not ideal for acute anginal pain.
In this unit, our prototype drug will be nitroglycerin.
Pharmacokinetics:
Nitroglycerin is highly lipid soluble which makes it ideal for routes such as sublingual and transdermal. It undergoes rapid inactivation by hepatic enzymes so oral doses are mostly reduced to being ineffective for acute use. For acute angina, only sublingual or buccal dosing is administered due to the fast onset of action and ease of administration. The half life is 1-4 minutes (Vallerand & Sanoski, 2024).
Nursing Considerations
Administration: sublingual, extended-release tablets, creams, transdermal patches, and intravenously. All produce the same effects with differences in onset and duration of action.
- Rapid acting: sublingual tablets or spray with onset 1-3 minutes and duration 30-60 minutes. Used for acute angina attack or for anticipated angina from exertion. PRN basis. Given as soon as the pain appears for best effect.
- Long acting: SR oral capsules, transdermal patches or topical ointment. Onset is 30-60 minutes with a long duration of action. Oral route duration of action is 3-8 hours and transdermal route has a duration of 24 hours. Transdermal patch is used for sustained protection from angina.
- Transdermal patch: constant release of nitro, with a range of patch sizes from 0.1-0.8 mg/hr. Apply daily and rotate sites. To avoid tolerance, must have a patch-free interval of 10-12 hours, usually at night. Ensure previous patch is removed before applying. Apply the patch to a hairless area, usually the upper chest.
For stable angina – long-acting nitrate for prophylaxis
- NTG Transdermal patch – 0.2 – 0.8 mg/h, one patch a day (remove at night for 10-12h)
- NTG Ointment – 7.5 – 40 mg a day
- NTG Oral capsules, SR 10-40mg TID
- Isosorbide: oral
For acute anginal pain – short acting nitrate for acute chest pain
- NTG Sublingual tablet – ie. 1 tab q 5 min x 3 rounds every 15 min (do not exceed 3 doses/per episode of chest pain)
- NTG Spray – (0.4 to 0.8 mg), 1 spray q 5 min to max of 3 sprays in 15 min. (do not exceed 3 doses/day)
For Heart Failure with acute MI, preop Hypertension++, hypertensive emergencies
- NTG IV – range from 10 to 120 micrograms/min.
Potential for tolerance to the effects of nitrates
- Allow for wash out period. For a transdermal patch – keep patch off 10-12 hours out of each day (usu overnight). prescriber will order patch-free period.
Prior to treatment, take blood pressure and heart rate. For NTG given for stable angina, reassess in one hour post-oral dose. A 10 mmHg drop is within normal limits.
Drug interactions:
- Cautious use with antihypertensives and CNS depressants due to hypotensive effects
- Clients taking sildenafil (Viagra) or similar medications for erectile dysfunction or PDE inhibitors in the previous 24 hours may not take nitroglycerin as this may result in a dangerous drop in blood pressure.
Nitroglycerin should not be used in pregnant women or those who are breastfeeding. If used, benefits should outweigh risks.
Contraindicated with severe anemia, increased intracranial pressure, hypersensitivity, or circulatory failure.
Cautious use with older adult due to fall risk from hypotension.
Adverse/Side Effects
Nitroglycerin is generally well tolerated.
Common side effects: headache, orthostatic hypotension, reflex tachycardia
- Orthostatic hypotension is due to blood pooling in the veins when sitting up. May experience light-headedness and dizziness.
- Reflex tachycardia results from a lower BP triggers baroreceptors and stimulating sympathetic stimulation of the heart. If this occurs, pretreatment with a beta blocker or CCB (verapamil) may be required (Burchum Rosenjack & Rosenthal, 2019).
Other side effects include palpitations, weakness, sweating, flushing, nausea, vomiting, or dizziness.
Client Teaching
- Instruct client to avoid eating or smoking during administration as this may alter absorption.
- Clients should sit during administration to decrease the risk for injury due to the possibility of hypotension, dizziness, and weakness.
- Refrain from alcohol as may experience flushing and weakness.
- Ensure client is informed of correct application and removal of transdermal patch
- Ensure client is informed of correct use of nitro spray or sublingual tablets for acute anginal attacks. Do not spray more than once every 5 minutes to a maximum of 3 sprays in 15 minutes to relieve chest pain. If chest pain is not relieved after the first dose, 911 should be called.
- Nitroglycerin may also be used prophylactically 5 to 10 minutes prior to engaging in activities that might precipitate an acute attack.
- Inform prescriber if there is any change to the pattern or severity of their chest pain.
- Nitroglycerin decomposes when exposed to heat or light, so it should be stored in the original, airtight glass container. See Figure 7.7b for an image of nitroglycerin containers.
(Kim, Adnan & Schaller, 2023; Vallerand & Sanoski, 2024)

Example in Practice:
This case study is to show the sequence of assessment and nitro administration for acute anginal pain.
A 63-year-old client has come into the emergency department with complaints of mid-sternal chest pain 7/10, non-radiating. It started 30 minutes ago when he was doing yard work and it has not subsided. He is visibly diaphoretic with slight shortness of breath. BP 148/82 HR 86 bpm, resp rate 22 breaths/min, oxygen sats 95%. He has no cardiac history and only has acid reflux that he takes the OTC antacid. He tells the nurse his partner had him chew an aspirin on the drive to ED.
After completing the assessment, the triage nurse brings him into the department. A 12 lead ECG is done and blood work for a troponin level and lytes are taken. While those orders are occurring, the nurse prepares to give nitroglycerin to relieve the chest pain.
The order reads:
Nitroglycerin 1 spray q 5 minutes for chest pain. Give up to 3 doses, 5 minutes apart.
The sequence of assessment and medication is the same each time.
Assess: chest pain (PQRST), BP, HR, RR and oxygen sats
- Chest pain 8/10 HR 93 bpm BP 148/90 RR 22 ) Oxygen sats 96%
Give: nitroglycerin 1 spray under the tongue
Wait 5 minutes
Reassess chest pain and vital signs. Still has chest pain?
- Chest pain 7/10 HR 82 bpm, BP 138/88 RR 20
Give (2nd dose): nitroglycerin 1 spray under the tongue
Wait 5 minutes.
Reassess chest pain and vital signs. Still has chest pain?
- Chest pain 4/10. HR 78 bpm BP 132/77 RR 18 O2 sats 94%
Give (3rd dose): nitroglycerin 1 spray under the tongue
Wait 5 minutes.
Reassess chest pain and vital signs. Still has chest pain?
- Chest pain 4/10. HR 75 bpm BP 130/75 RR 18 O2 sats 96%
At this point, no more nitro can be given. The goal is no chest pain. The nurse checks the orders and she can give Morphine 1-5 mg IV q 5 minutes to a maximum of 20 mg in 1 hour.
Morphine 2 mg IVP is given (Pain is 4/10 and client opioid naïve. Start with a low dose)
The nurse stays with the client, reassesses chest pain and vital signs in 5 minutes.
5 minutes: At this point, the client states his chest pain has gone away.HR 80 bpm BP 128/70 RR 14 with O2 sats of 95%. In some critical care areas, nitroglycerin infusion could be initiated instead of morphine.
Other care that is occurring during this time include:
- Bedrest
- NPO
- Intravenous access – 2 peripheral IVs, saline lock
- Complete a physical assessment (especially lung sounds, skin colour, edema)
- Provide supplemental oxygen if oxygen sats are less than 94% or per your agency policy.
Nitroglycerine Medication Card
Now let’s take a closer look at the medication card for nitroglycerin. Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.

Downloadable file (.docx): Nitroglycerine Medication Card
Clinical Reasoning and Decision-Making Activity
- A client was administered the first dose of nitroglycerin at 1305hrs for acute angina. What should the nurse evaluate after administration?
- A client has been experiencing occasional mild substernal chest pain when he exercises. They go to the clinic and a cardiac assessment is completed. They are currently pain free. The client is prescribed Nitro spray 1 spray for chest pain. Repeat 2x if unrelieved.
- How does this med work to relieve chest pain?
- What teaching will the client need to administer this med safely? Include in your answer common side effects and correct administration of the med.
- A 70-year-old client has a history of stable angina. He is ordered: Nitro patch 0.4mg/hr. Apply at 0900h and remove at 2000hr.
- What is the purpose of this type of order?
- Prior to applying the patch in the morning, what should the nurse assess?
Note: Answers to the Clinical Reasoning Activities and Critical Thinking questions can be found in the Chapter 7: Cardiovascular Medications Answer key – Fundamentals of Nursing Pharmacology – 2nd Canadian Edition section at the end of the book.
References
Adams, M., Urban, C., El-Hussein, M., Osuji, J. & King, S. (2018). Pharmacology for Nurses. A pathophysiological approach (2nd Canadian ed.). Chapter 3: Pharmacokinetics. Pearson Canada Inc: Ontario.
Kim, K., Adnan, G. & Schaller, D. (2023). Nitroglycerin. National Library of Medicine. Nitroglycerin – StatPearls – NCBI Bookshelf
O’Gara, P., Kushner, F. , Ascheim, D. , Casey, D., Chung, M., de Lemos, J., Ettinger, S., Fang, J, Fesmire, F., Franklin, B., Granger, C., Krumholz, H., Linderbaum, J., Morrow, D., Newby, L., Ornato, J., Ou, N., Radford, M., Tamis-Holland, J., Tommaso, C., Tracy, C., Woo, Y., & Zhao, D. (2013). ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation, 127(4). https://www.ahajournals.org/doi/full/10.1161/CIR.0b013e3182742cf6?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub%3Dpubmed ↵
Rosenjack Burchum, J., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
Vallerand, A. & Sanoski, C. (2024). Davis’s Canadian drug guide for nurses (19th ed.). F.A. Davis Company: Canada
Media Attributions
- 7.7a The mechanism of action of nitrates on the heart is by Sheila Odubote/TRU Open Press.
- 7.7b Sublingual nitroglycerin [Nitroglycerin (1).JPG] by Intropin on Wikimedia Commons is licensed under CC BY 3.0 license.

.JPG){kind=link}