9.3 Conditions and Diseases of the Gastrointestinal System
Proper functioning of the gastrointestinal system is essential in providing the necessary nutrients to other body systems and vital organs. The ability to take in nutrients, convert them to a usable form to support body functions and then eliminate waste involves numerous processes and any alteration can significantly impact a clients physical, social and psychological functioning. For example, a client with chronic diarrhea can impact the ability to enjoy social events or work. Persistent nausea can lead to a decrease in food and fluid intake leading to dehydration and nutritional deficiencies. There are many GI disorders and it is beyond the scope of this book to explore them all. In this section, we will review common conditions and diseases related to the gastrointestinal system including conditions related to hyperacidity (Gastroesophageal reflux disease, peptic ulcer disorder and stress ulcers), alterations in the lower GI system (diarrhea, constipation), and nausea and vomiting.
Conditions related to Hyperacidity
Gastroesophageal Reflux Disease
Jessica -Nov 12, 2025: The hyperlink below it takes us to version 1 of the book instead of the current version (this book which is version 2)
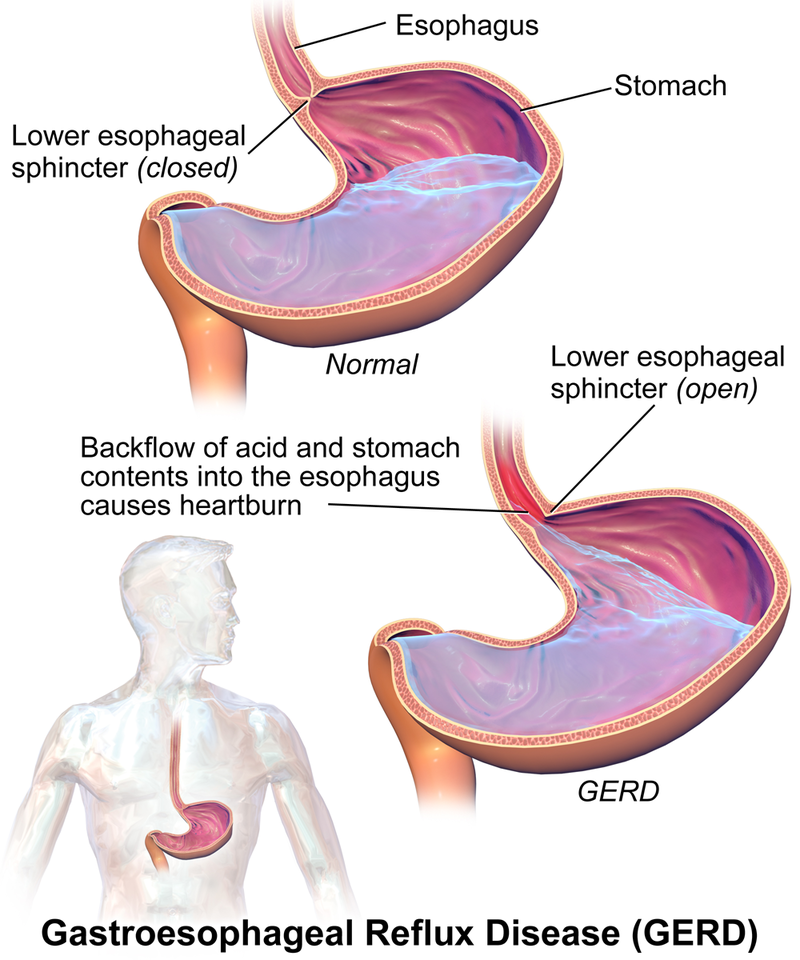
One of the most common problems associated with the gastrointestinal system is hypersecretion of gastric acid (hyperacidity). Gastroesophageal reflux disease (GERD) is often referred to by clients as heartburn, indigestion, or sour stomach. GERD is caused by excessive hydrochloric acid that tends to back up, or reflux, into the lower esophagus. See Figure 9.3a for an illustration of GERD (Blaus, 2015).
Andrea’s note: From the current OER. Figure 9.3a for an illustration of GERD.[1]
GERD is often a benign condition, easily treated with over-the-counter remedies such as antacids or other anti-ulcer medications. Many clients have persistent or chronic GERD, with daily troublesome symptoms that impact quality of life. It is estimated approximately 15% of the Canadian population has GERD (Canadian Digestive Health Foundation, 2025). The incidence of GERD is increasing globally, with precipitating factors of dietary choices, increasing obesity rates and genetic predispositions (Tanvir, Nijjar, Aulakh, et al., 2024).
For some clients, GERD is not easy to treat and can lead to inflammation in the gastric mucosa, esophagitis, and an erosion of mucosa leading to an ulcer. Rarely, clients could develop Barrett’s esophagus which is the primary risk factor for cancer of the esophagus (Canadian Digestive Health Foundation, 2025). Due to the impact of abdominal discomfort and the risk of more serious complications, the early treatment of hyperacidity is important.
Risk factors for developing gastroesophageal reflux disease
The likelihood of experiencing GERD include both modifiable and non-modifiable risk factors. Some clients are more predisposed due to other underlying health conditions, but often there are factors that increase a client’s risk of experiencing symptoms.
Modifiable risk factors:
- obesity,
- smoking,
- dietary choices. Many foods can trigger symptoms and include high fat/high cholesterol foods, spicy foods, citrus fruits or juices, alcohol consumption, coffee and spicey foods. Even chocolate can be a trigger.
- emotional stress and anxiety.
To alleviate or prevent GERD, clients should know the triggers that can precipitate their symptoms.
Non-modifiable risk factors:
- Parental or family history of GERD, such as muscular or structural issues with the esophagus or stomach.
- Age is also a factor with increasing prevalence from mid-adulthood onwards. There are exceptions though, with some children and adolescents presenting with symptoms.
- Physiological conditions such as lower esophageal sphincter relaxation or abnormalities, delayed gastric emptying or impaired salivary functioning (Tanvir, Nijjar, Aulakh, et al., 2024). For example, clients with a hiatus hernia, a defect in the diaphragm that allows the stomach to pass through the diaphragmatic opening into the thorax, can experience heartburn, dysphagia and chest pain (Copstead & Banasik, 2010, p. 836).
- Many pregnant women also experience GERD, with an estimated 25% experience heartburn daily. Symptomatic GERD usually presents in the first trimester and progresses throughout pregnancy (Altuwaijri, 2022). The occurrence of GERD in pregnancy is related to both hormonal and structural changes and often is alleviated following birth.
- Some clients with other health conditions such as lung transplantation or cystic fibrosis are also predisposed.
Balancing Act between Defensive and Aggravating Factors
Acid-related disorders can also occur when there is an imbalance between defensive factors that protect the mucosa and aggravating factors that can lead to a reflux of acid secretions by the surface epithelium cells in the stomach.
Defensive Factors:
Our bodies have a unique way to protect the mucosa lining of the stomach.
- A thick mucous layer is secreted continuously from the epithelial cells that line the stomach. The mucous forms a protective barrier.
- Bicarbonate, secreted by the epithelial cells of the stomach and duodenum buffers acidic properties of HCL and neutralizes H ions that penetrate the mucus.
- Prostaglandins stimulate the production of mucus and bicarbonate, as well as promotes vasodilation.
A healthy blood flow to the tissues also provides a defensive mechanism, by bringing nutrients to the tissues (Sealock & Seneviratne, 2021).
Aggravating Factors:
These defensive factors can be overwhelmed by aggravating factors which can be episodic or chronic.
- Hyperacidity – some clients have hyperacidity that is either increased with food or fluid choices, or more rarely, due to hyperacidity conditions.
- Pepsin, an enzyme in our digestive juices, can inflame the mucosa.
- Smoking blocks prostaglandins and impairs blood flow to the mucosa.
- Nonsteroidal Anti-inflammatory medications (NSAIDs), such as Ibuprofen, if taken on a regular basis also lead to a drop in prostaglandin production thereby decreasing mucous and bicarbonate production.
- Heliobacterium Pylori (H. Pylori) is a gram-negative bacterium that can colonize in our stomach. If the bacteria numbers are elevated, due to a decrease in our normal flora, H. Pylori will lead to an erosion of the gastric mucosa (National Collaborating Center for Infectious Diseases, 2023). To learn more about H. Pylori, go to https://nccid.ca/debrief/helicobacter-pylori/
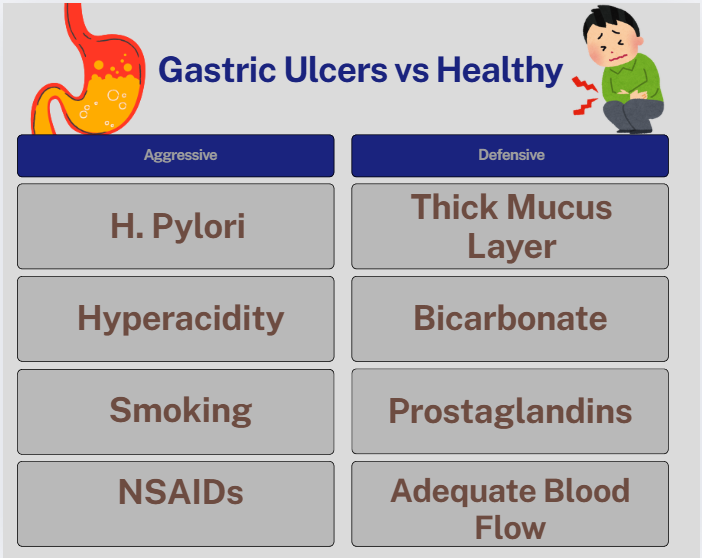
Figure 9.3b Gastroesophageal Reflux Disease: aggressive factors can overwhelm defensive factors (Sheila Odubote/TRU Open Press)
Peptic Ulcer Disease
Jessica -Nov 12, 2025: The hyperlink below it takes us to version 1 of the book
Peptic ulcer disease (PUD) occurs when gastric or duodenal ulcers are caused by the breakdown of GI mucosa by pepsin, in combination with the caustic effects of hydrochloric acid. The injury to the mucosa can occur in the esophagus, stomach or duodenum and can range from irritation to severe ulceration. Hyperacidity can contribute to PUD, but major precipitating factors are NSAID use and the organism H. Pylori (Copstead & Banasik, 2010, p.839). Other factors include genetic predisposition. For example persons of African American/Hispanic ethnicity or a first degree relative with PUD have a higher incidence (Malik, Gnanapandithan & Singh, 2022).
Helicobacter Pylori-Associated PUD
- pylorusis a gram-negative bacillus that is found within the gastric epithelial cells. This bacterium is responsible for 90% of duodenal ulcers and 70% to 90% of gastric ulcers. Although H. pyloriinfection can occur in anyone, it is more prevalent among those with lower socioeconomic status and is commonly acquired during childhood (Malik, Gnanapandithan & Singh, 2022). The organism has a wide spectrum of virulence factors, allowing it to adhere to and inflame the gastric mucosa, leading to gastric ulceration. Diagnosis of H. Pylori can include a urea breath test, serologic testing or stool antigen test.
The treatment for H. Pylori is triple therapy with the prescription of two antimicrobials and a proton pump inhibitor. Pantoprazole, clarithromycin, and metronidazole, or amoxicillin are used for 7 to 14 days. Sometimes, the addition of bismuth salicylate is also prescribed.
Nonsteroidal anti-inflammatory drug (NSAID) associated PUD
NSAID use is the second most common cause of PUD after H. pylori infection (Malik, Gnanapandithan & Singh, 2022). The secretion of prostaglandin normally protects the gastric mucosa. NSAIDs block prostaglandin synthesis by inhibiting the COX-1 enzyme, resulting in decreased gastric mucus and bicarbonate production and a decrease in mucosal blood flow. Avoiding or minimizing the use of NSAIDs is an important step in treatment. Other medications also contribute to PUD and include corticosteroids and potassium chloride.
PUD is the most harmful disease related to hyperacidity because it can result in bleeding ulcers, a life-threatening condition. As such, prompt diagnosis and treatment is essential.
Stress Ulcers
Jessica -Nov 13, 2025: The hyperlinks below it takes us to version 1 of the book
Stress-related mucosal damage is another common condition that can occur in hospitalized clients leading to PUD. Thus, many post-operative or critically ill clients receive medication to prevent the formation of a stress ulcer, which is also called stress ulcer prophylaxis (Sealock & Seneviratne, 2021) . See an image of a duodenal ulcer in Figure 9.3b.(Blausen Medical, 2015).

The following video link provides a basic understanding illustrating heartburn. Heartburn[4]
Alterations in Bowel Patterns
There is a wide variation in bowel patterns and what may be considered normal for one individual may be considered an issue for someone else. Completing a comprehensive history of a client’s bowel patterns (frequency, consistency, history of bowel patterns and conditions) along with a GI assessment and diet history will assist in determining a treatment plan.
Diarrhea
Diarrhea itself is not a disease but is a sign and symptom of other conditions and disease processes in the body.
Jessica -Nov 13, 2025: The hyperlink below takes us to version 1 of the book
Diarrhea is defined as the passage of three or more loose or liquid stools per day (or more frequent passage than is normal for the individual). Frequent passing of formed stools is not considered diarrhea. Using a tool such as the Bristol Stool chart can help in identifying stool characteristics.
Diarrhea has multiple causes such as bacteria from contaminated food or water; viruses such as influenza, norovirus, or rotavirus; parasites found in contaminated food or water; medicines such as antibiotics, cancer drugs, and antacids that contain magnesium; food intolerances and sensitivities; and diseases that affect the colon, such as Crohn’s disease or irritable bowel syndrome (National Institute of Diabetes and Digestive and Kidney Diseases, 2018). Diarrhea can also occur as a result of emotional stress or from leakage of stool around impacted feces. If diarrhea is acute in nature, it may be attributed to food sensitivities or medications, stress or ingestion of an irritant such as caffeine. Chronic diarrhea is defined as symptoms greater than 4 weeks, and can be related to many issues such as GI or endocrine disorders.
The most severe threat posed by diarrhea is dehydration caused by the loss of water and electrolytes. This can occur with either acute or chronic diarrhea and will depend on the severity of symptoms. Diarrheal disease is a leading cause of child mortality and morbidity throughout the world due to dehydration; frail elderly are also at risk. When severe diarrhea occurs, assessment for dehydration and electrolyte imbalances receive top priority and rehydration with oral rehydration solutions or IV fluids may be required (World Heath Organization, 2017).
Constipation
Jessica -Nov 13, 2025: The hyperlinks below take us to version 1 of the book
Constipation is defined as “three or fewer bowel movements in a week; stools that are hard, dry or lumpy; stools that are difficult or painful to pass; or the feeling that not all stool has passed.” (National Institute of Diabetes and Digestive and Kidney Diseases, 2018). If defecation is delayed for an extended time, additional water is absorbed, thus making the feces firmer and potentially leading to constipation.
There are several causes of constipation, such as lack of proper fluids or fiber in the diet, lack of ambulation, various disease processes, recovery from surgical anesthesia and opiates, and side effects of many medications. A list of these potential causes can be found in Table 9.3a (National Institute of Diabetes and Digestive and Kidney Diseases, 2018).
Because there are several potential causes of constipation, treatment should always be individualized to the client. Many times, constipation can be treated with simple changes in diet, exercise, or routine. However, when medications are also needed to resolve constipation, there are several categories of laxative medications that work in different ways. Classes of laxative medications are described below.
| Cause | Examples |
| Medications |
|
| Health and Nutrition Problems |
|
| Daily Routine Changes |
|
Nausea and Vomiting
Similar to diarrhea and constipation, nausea and vomiting are common conditions that are most often signs and symptoms of other conditions or side effects of medication.
Nausea is a commonly encountered symptom that can be described as an unpleasant sensation of having the urge to vomit. Nausea often precedes vomiting but not always. Vomiting (emesis) is the forceful expulsion of gastric contents. Nausea and vomiting are considered a protective mechanism, against the potential of toxic ingestion. Nausea can also be attributed to many other situations including medications (ie. Post-op nausea, chemotherapy) and motion sickness. It can also be attributed to many other conditions such as gastrointestinal, cardiac, labyrinthine, metabolic or endocrine disorders (Singh, Yoon, & Kuo, 2016).
Causes of Nausea
There are many causes of nausea. Some examples include:
Medications:
- analgesics,
- cardiac meds (beta blockers, digoxin),
- hormone meds (oral anti-diabetic, oral contraceptives),
- antibiotics (erythromycin, tetracycline),
- anti-Parkinson meds
Disorders or conditions:
- GI disorders (obstruction, irritable bowel syndrome, gastroenteritis),
- neuro disorders (migraines, increased intracranial pressure),
- psychiatric conditions (depression, pian, anxiety),
- pregnancy (morning sickness due to hormonal changes)
- endocrine (diabetic ketoacidosis),
- cardiac (myocardial infarction, congestive heart failure).
Toxins:
- food poisoning
- exposure to toxic substances
Nausea is triggered by a diverse emetic stimulus through central and/or peripheral nervous systems. It is a complex process activating the Vomiting Center either directly or indirectly.
Vomiting Center
The vomiting center, located in the medulla is like a coordination center that receives input from four areas before initiating the vomiting reflex. The four principal areas are:
- chemoreceptor trigger zone (CTZ)
- gastrointestinal tract,
- cerebral cortex and thalamus,
- vestibular region
See Figure 9.3c for an illustration of the pathophysiology of nausea and vomiting.[11]
Jessica -Nov 13, 2025: The hyperlinks below take us to version 1 of the book
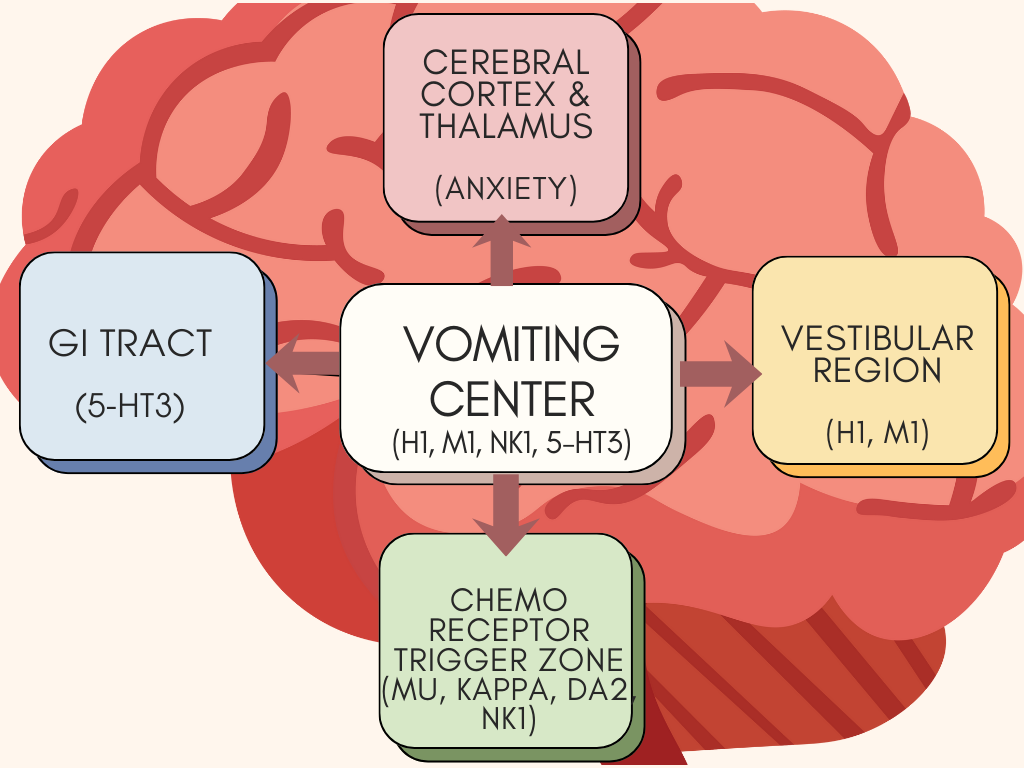
Figure 9.3c Pathophysiology of nausea and vomiting [Image Description]
Chemoreceptor Trigger Zone
<p”>An important part of the emesis circuit is the chemoreceptor trigger zone (CTZ), located in the area postrema in the brain. The CTZ is not restricted by the blood–brain barrier, which allows it to respond directly to toxins in the bloodstream such as anesthesia and opioids. The CTZ also receives stimuli from several other locations in the body including the vestibular center; visceral organs such as the GI tract, kidneys, and liver; the thalamus; and the cerebral cortex. The CTZ contains receptors for dopamine, serotonin (5-HT3), opioids, and substance P, which, when activated, send signals to the vomiting center.
Vestibular Center
The vestibular center can stimulate the vomiting center directly or indirectly through the CTZ. The vestibular system is located within the inner ear and gives a sense of balance and spatial orientation for the purpose of coordinating movement with balance. The feeling of nausea associated with motion sickness often arises from stimuli from the vestibular center.
Cerebral Cortex
The cerebral cortex and other parts of the brain can also stimulate the vomiting center directly. The stimuli are often related to our senses: odors, tastes, images or sights. All these signals then can send stimuli to the CTZ, which then go to the vomiting center. Pain can also directly stimulate the vomiting center.
Gastrointestinal Tract
In the GI tract, sensory nerves via the vagus and sympathetic nerves send signals to the vomiting center. These afferent nerves are stimulated by mucosal irritation such as infection or chemotherapy, or overdistension of the stomach.
The gastrointestinal tract sends stimuli to the CTZ via cranial nerves IX and X related to obstruction, distension, inflammation, and infection.
These signals to the vomiting center initiates vomiting by inhibiting peristalsis and producing retro-peristaltic contractions beginning in the small bowel and ascending into the stomach. It also produces simultaneous contractions in the abdominal muscles and diaphragm that generate high pressures to propel the stomach contents upwards. Additionally, autonomic stimulation of the heart, airways, salivary glands, and skin cause other symptoms associated with vomiting such as salivation, pallor, sweating, and tachycardia.
Physiology of Vomiting
The following video reviews the vomiting reflex, with attention to the neurotransmitters involved in the nausea and vomiting process. Anti-emetic medications target the receptors of specific neurotransmitters, blocking their action and alleviating nausea (Becker, 2010).
Andrea’s note: Jessica – I would like to use the following video. It is from youtube. Not sure if it is available to use freely.
@Copyeditor can we use the YouTube video below ? – Jessica / Nov 13, 2025
Hasudungan, A. (2007). Physiology of Vomiting – Vomiting reflex
https://www.youtube.com/watch?v=GSHTLWbwKgo https://youtu.be/GSHTLWbwKgo
Example in Practice
A client is on a cruise and begins to feel nauseated. Her mouth begins to water, she begins to feel sweaty and her heart rate increases.
Motion sickness is a common occurrence and is initiated by signals from the vestibular system in the inner ear.
Along with the sensation of nausea, other physiological responses also occur. Autonomic stimulation leads to increased salivation. Sympathetic stimulation can lead to other sensations such as diaphoresis, dizziness and tachycardia.
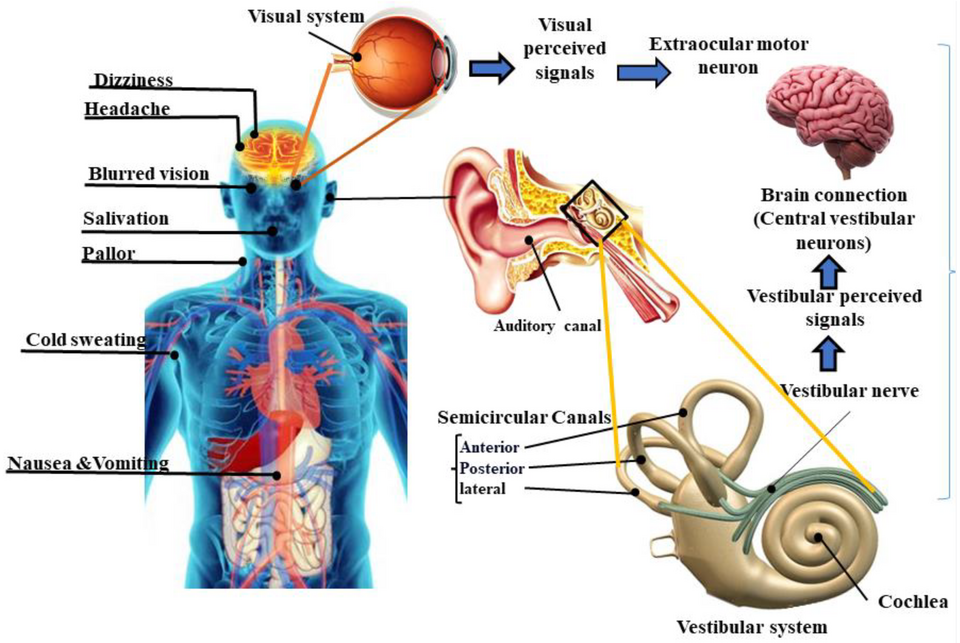
https://commons.wikimedia.org/wiki/File:Motion_sickness.png
Jessica – Nov 13, 2025: The hyperlinks below take us to version 1 of the book
Most clients can treat their symptoms of nausea or vomiting with OTC anti-emetics. A health care provider should be contacted immediately if the following conditions occur:
- Vomiting for longer than 24 hours
- Blood in the vomit (also called hematemesis)
- Severe abdominal pain
- Severe headache and stiff neck
- Signs of dehydration, such as dry mouth, infrequent urination, or dark urine
Image Descriptions
Figure 9.3a image description: Illustration of GERD.
The stomach is located in the upper left quadrant of the abdomen and the esophagus comes down from the throat to the stomach.
When it is normal, the lower oesophageal sphincter, which is between the esophagus and stomach, is closed. Stomach acid and stomach contents sit in the stomach.
When a person has GERD, the lower esophageal sphincter is open. This allows a back flow of acid and stomach contents into the esophagus, which causes heartburn. [Return to figure 9.3a]
Figure 9.3c image description: The pathophysiology of nausea and vomiting.
The Vomiting Center sits in the centre. The receptors illustrated in the vomiting center are:
- H1 histamine
- M1 acetylcholine
- NK1 (neurokinin), and 5-HT3 serotonin.
Four principal areas can activate the vomiting center:
- GI Tract (5-HT3 serotonin)
- Cortex Thalamus (Anxiety, Pain)
- Vestibular (H1 histamine, M1 acetylcholine)
- Chemoreceptor trigger zone (mu/kappa opioids, DA2 dopamine, and NK1 (neurokinin)) [Return to figure 9.3c]
References
Jessica – Nov 13, 2025: The hyperlinks below ↵ of take us to version 1 of the book
A.D.A.M. Medical Encyclopedia [Internet]. Atlanta (GA): A.D.A.M., Inc.; ©2019. Heartburn; [reviewed 2019 May 10; cited 2019 October 27]. https://medlineplus.gov/ency/anatomyvideos/000068.htm ↵
Altuwaijri, M. (2022, Sept 2). Evidence-based treatment recommendations for gastroesophageal reflux disease during pregnancy: A review. Medicine (Baltimore), 101(35):e30487. doi: 10.1097/MD.0000000000030487 . Evidence-based treatment recommendations for gastroesophageal reflux disease during pregnancy: A review – PMC
Bashashati, M. & McCallum, R. (2014). Neurochemical mechanisms and pharmacologic strategies in managing nausea and vomiting related to cyclic vomiting syndrome and other gastrointestinal disorders. European Journal of Pharmacology, 772, p 79. ↵
Becker D. E. (2010). Nausea, vomiting, and hiccups: a review of mechanisms and treatment. Anesthesia Progress, 57(4), 150–157. doi:10.2344/0003-3006-57.4.150 ↵ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3006663/ ↵
Blausen Medical. (2015, November 17). Gastric Ulcers [Video].https://blausen.com/en/video/gastric-ulcers/# ↵
Canadian Digestive Health Foundation (2025). Gastroesophageal reflux disease. Retrieved from https://cdhf.ca/en/digestive-conditions/gerd/
Copstead, L. & Banasik, J. (2010). Esophageal disorders. Pathophysiology (4th ed.). St Louis, Missouri: Saunders Elsevier.
“Duodenal ulcer01.jpg” by melvil is licensed under CC BY-SA 4.0
“GERD.png” by BruceBlaus is licensed under CC BY-SA 4.0 ↵
Malik, T., Gnanapandithan, K., Singh, K. (2022, June 5). Peptic Ulcer Disease. National Library of Medicine. StatPearls [internet]. Peptic Ulcer Disease – StatPearls – NCBI Bookshelf
MedlinePlus. Bethesda (MD): National Library of Medicine (US); [updated 2019 October 23]. Heartburn; [updated 2019 October 2; cited 2019 October 27] https://medlineplus.gov/ency/anatomyvideos/000068.htm ↵
National Collaborating Center for Infectious Diseases (2023, June 15). Helicobacter Pylori. University of Manitoba. Retrieved from https://nccid.ca/debrief/helicobacter-pylori/
National Institute of Diabetes and Digestive and Kidney Diseases, National Institute of Health. (2018). Symptoms and causes of constipation.https://www.niddk.nih.gov/health-information/digestive-diseases/constipation/symptoms-causes ↵
Sealock, K. & Seneviratne, C. (2021). Lilley’s Pharmacology for Canadian health care practice (4th Ed). Elsevier. ↵
Singh, P., Yoon, S., & Kuo, B. (2016). Nausea: a review of pathophysiology and therapeutics. Therapeutic Advances in Gastroenterology, 9(1):98–112. doi: 10.1177/1756283X15618131
PMCID: PMC4699282 PMID: 26770271
Tanvir F, Nijjar G, Aulakh S, et al. (August 24, 2024) Gastroesophageal Reflux Disease: New Insights and Treatment Approaches. Cureus 16(8): e67654. doi:10.7759/cureus.67654
Gastroesophageal Reflux Disease: New Insights and Treatment Approaches | Cureus
World Health Organization. (2017, May 2). Diarrhoeal disease.https://www.who.int/en/news-room/fact-sheets/detail/diarrhoeal-disease. ↵
Occurs when gastric or duodenal ulcers are caused by the breakdown of GI mucosa by pepsin in combination with the caustic effects of hydrochloric acid.
A common condition in hospitalized patients that can lead to PUD.
Medication to prevent the formation of stress ulcers.
The passage of three or more loose or liquid stools per day (or more frequent passage than is normal for the individual).
Three or fewer bowel movements in a week; stools that are hard, dry or lumpy; stools that are difficult or painful to pass; or the feeling that not all stool has passed.
Area in the brain that responds directly to toxins in the bloodstream and stimulates the vomiting center. The CTZ receives stimuli from several other locations in the body.
A structure in the medulla oblongata in the brainstem that controls vomiting. Its location in the brain also allows it to play a vital role in the control of autonomic functions by the central nervous system.
An area located within the inner ear that gives a sense of balance and spatial orientation for the purpose of coordinating movement with balance.
Blood in the vomit.

{kind=link}
{kind=link}