5.2 Diseases and Disorders of the CNS, Mood, and Cognition V2
Now that we have reviewed basic concepts of neurotransmitters and their function, let’s review common conditions and disorders related to the central nervous system. Conditions that affect the central nervous system can be categorized into neurological or cognitive and mood disorders.
Although neurological disorders are more prevalent in Canadians over the age of 65, many conditions are not exclusive to the older population. Some conditions impact clients in their 20s or 30s such as brain or spinal tumours, dystonia, epilepsy, multiple sclerosis, or migraines. Some disorders first appear more in childhood, such as muscular dystrophy. Other conditions only appear in the mid to older adult, such as amyotrophic lateral sclerosis (Lou Gehrig’s disease), Alzheimer’s disease and other dementias (Government of Canada, 2025).
Mood disorders involve dysfunction in the areas of behaviour and personality and can have a significant impact on the person’s ability to function. The causative factors of many conditions are multifaceted including biochemical, structural, genetic or traumatic events and stressors. Mood disorders are an umbrella term that includes anxiety and panic disorders, psychoses and depressive disorders, all of which have subsets of conditions that can be mildly disruptive to debilitating (Varcarolis, E. M., 2017). Mood disorders such as depression and anxiety are prevalent among our young adult population but can occur at any age.
Due to the extensive list of neurological disorders and mental health conditions, only the more common conditions will be reviewed.
- Mental health conditions: anxiety, depression, bipolar, schizophrenia and attention deficit hyperactivity disorder (ADHD).
- Seizure disorders,
- Neurodegenerative diseases:
- Parkinson’s disease
- Alzheimer’s disease and dementia
Additional supplementary videos about CNS disorders are available at Khan Academy
Cognition and Mood Disorders
Mental health challenges are common for most people at some point in their lives. Some people experience more persistent or severe symptoms that last longer and have an impact on their daily lives. Mood disorders are characterized by a disruption in thinking, mood, or behaviour and are associated with distress and impaired functioning (World Health Organization, 2026).
In 2022, the Mental Health and Access to Care Survey was conducted to learn about the prevalence of mental health disorders in Canada and access to mental health services (Statistics Canada, 2025). Mental health disorders, particularly mood or anxiety disorders, have been increasing over the last 10 years in Canada. In 2022, more than 5 million people in Canada have been diagnosed with a mood, anxiety or substance use disorder (Statistics Canada, 2025). Generalized anxiety disorder for Canadians over 15 years of age has doubled from 2012 to 2022 to 5.2%, with similar increases in those diagnosed with major depressive episodes and bipolar disorders. Globally, there is a general decline in mental health, with an increase in depression and anxiety particularly more prevalent with the onset of COVID-19 pandemic in 2020 (Stephenson, 2023). In Canada, women are more effected with mood or anxiety disorders than men. From 2012 to 2022, there was an increase from 9.0% to 18.4% in women experiencing a major depressive episode. Substantive increases were also shown for other conditions such as generalized anxiety disorder and social phobias (Stephenson, 2023). These statistics help health care providers understand the health care needs of the population and to help ensure supports and access to treatment are in place such as community mental health counselling.
Psychiatric and mental health disorders are often due to an imbalance of neurotransmitters. There are many reasons for this imbalance, but can have genetic, environmental, hormonal changes, and exposure to toxins as some factors. The overall goal of treatment is to relieve or reduce dysfunctional thoughts and improve overall functioning. This is accomplished with modulating neurotransmitters, which is the basis of CNS drugs.
This unit will provide only a general overview on the more common mental health disorders as a precursor to understanding medications to treat some of these conditions.
Anxiety
Anxiety disorders are a group of conditions marked by pathological or extreme anxiety or dread. Types of anxiety include separation anxiety, generalized anxiety, social phobias, social anxiety, panic disorders and selective mutism. People with anxiety experience disturbances of mood, behavior, and most systems in the body, making them unable to continue with everyday activities. Many feel anxious most of the time for no apparent reason (Melrose, n.d.).
Anxiety is different from fear. Fear is a person’s response to an event or object. The psychiatric disorder of anxiety occurs when the intensity and duration of anxiety do not match the potential for harm or threat to the affected person. Anxiety can be expressed with physical symptoms or behaviorally (Melrose, n.d.). This list is not exhaustive but demonstrates the wide range of symptoms the client may experience and that the nurse needs to consider as part of their assessment (Chand, Marwaha, & Bender, 2023).
Signs and Symptoms of Anxiety
Cognitive symptoms: fear of losing control, fear of negative evaluation by others; frightening thoughts, mental images, or memories; perception of unreality or detachment; poor concentration, confusion, narrowing of attention, hypervigilance for threat; poor memory; and difficulty speaking.
Physiological symptoms: headache, increased heart rate, palpitations; shortness of breath, rapid breathing; chest pain or pressure; light-headed; sweaty, hot flashes, nausea, upset stomach, diarrhea; trembling, unsteadiness.
Behavioral symptoms: avoidance of threat cues or situations; escape, flight; pursuit of safety, reassurance; restlessness, agitation, pacing; hyperventilation; freezing, and difficulty speaking.
Affective symptoms: nervous, tense, fearful, edgy, and impatient.

Treatment consists of psychotherapy, pharmacotherapy, or a combination of both. Medications to treat the anxiety can include anti-depressants, anxiolytics, and even beta blockers (propranolol for social phobias). These medications will be explored later on in this chapter.
Psychotherapy is almost always recommended. Cognitive-behavioural therapy is one of the most effective therapies that focuses on the client identifying and modifying characteristic maladaptive thinking patterns and beliefs that trigger and maintain symptoms (Chand, Marwaha, & Bender, 2023). The client learns better ways to react and adapt to anxiety-producing situations. Other non-pharmacological interventions to decrease anxiety include relaxation techniques such as deep breathing, exercise, and support groups.
Learn more about anxiety from the Canadian Mental Health Association.
Attention-Deficit/Hyperactivity Disorder
Attention-deficit/hyperactivity disorder (ADHD) is one of the most common neurodevelopmental disorders. It is characterized by hyperactivity, lack of impulse control, and/or lack of attention that interferes with how a person functions. ADHD is often diagnosed during childhood, and affects about 5% of the school age population. Boys are three times more likely to develop ADHD than girls. Symptoms develop in childhood and these traits can lead to poor performance in school (difficult with focusing, sitting still), difficulty with peer and family relationships and increased motor activity that may be inappropriate (Statistics Canada, 2015; Varcarolis, 2017). Approximately 50% of cases continue into adulthood, and can impact work performance and personal relationships.
Presenting Symptoms of ADHD
- Hyperactivity (fidgets, talks excessively, can’t sit still)
- Impulsivity (interrupts, difficulty waiting for turn, impatience)
- Lack of attention (difficulty paying attention, easily distracted, does not pay attention to social cues)
For a diagnosis of ADHD or ADD, symptoms must be present in at least two settings, such as at home and at school. ADHD in adults may present with an associated symptom such as procrastination, lack of motivation, labile moods or disorganization (Halter, Pollard & Jakubec, 2019).
Treatment includes medication such as CNS stimulants and non-stimulants, behaviour management, psychotherapy and family support.

Depression
Depression is defined as a persistent feeling of sadness and loss of interest (Chand & Arif, 2023). It can be characterized by episodes of depressed mood, that includes reduction in energy, lower mood, and decrease in activity. Furthermore, the capacity for enjoyment, interest and concentration is reduced, as well as sleep disturbances, fatigue and appetite issues (World Health Organization, 2021). A depressive disorder is diagnosed when the symptoms reach a threshold and lasts at least two weeks. If these problems become chronic or recurrent it can lead to impairment in an individual’s ability to care for themselves and in severe cases, it can lead to suicide.
Depression is a broad term to identify a number of depressive disorders such as seasonal affective disorder, major depressive disorder, persistent depressive disorder (dysthymia), premenstrual dysphoric disorder, and depressive disorder due to another medical condition.
In Canada, 1% of men and 2% of Canadian women are clinically depressed at any point in time and about 5% of men and 10% of women will experience clinical depression at some point in their life (Canadian Psychological Association, 2021). It is anticipated that major depressive disorders will be the second leading cause of disability globally (World Health Organization, 2021). Regardless of where a nurse works, they will care for someone with depression or the primary condition is complicated by depression (Halter, Pollard & Jacubec, 2019, pg. 245). The causative factors include both genetic and environmental factors (traumatic events, life events).
To be diagnosed with Major Depressive Disorder (MDD), the most severe form of depression, five of the following symptoms must be present within a two-week period (Chand & Arif, 2023; Mayo Clinic, 2018).
Signs and Symptoms of Depression
- Depressed mood
- Diminished interest in activities or social withdrawal
- Weight loss when not dieting or weight gain
- Insomnia or hypersomnia
- Agitation
- Fatigue or loss of energy
- Feeling of worthlessness
- Inappropriate guilt
- Diminished ability to concentrate
- Recurrent thoughts of death, suicidal ideation, or suicide attempt
Symptoms can vary in severity and duration. All clients should be asked about suicidal thoughts or attempts and risk of harm to others. Clients who are depressed may not report symptoms unless specifically asked, so using appropriate assessment techniques is important.
At the time of initial assessment, a thorough health history that includes:
- past and current medical history,
- family history,
- social history with emphasis on stressors or triggering events.
- support system
Physical examination and lab work may also be required to rule out medical causes of symptoms (Varcarolis, 2017).
Treatment of depression typically includes some form of therapy such as psychotherapy, cognitive therapy, electroconvulsive therapy (ECT), or group therapy. Non-pharmacological interventions may be used alone or along with medications. There are a number of anti-depressants which can be prescribed which will be explored in the Anti-depressant Medication unit.
Although only 35% of individuals receive treatment for depression, it is estimated that nearly 40% of those treated for depression with antidepressants achieve full remission, while up to 30% achieve at least a 50% reduction in symptom severity (Rosenjack Burchum & Rosenthal, 2019).
Learn more about depression from the Canadian Mental Health Association.
Bipolar Disorder
Bipolar affective disorder (formerly manic-depressive disorder) is a mood disorder marked by clear shifts in energy, mood, activity levels and concentration. Typically, clients experience extreme highs (called mania or hypomania) alternating with extreme lows (depression). See the “Depression” section for signs and symptoms of depression. People feel normal only in the periods between the highs and lows. For some people, the cycles occur so rapidly that they hardly ever feel a sense of control over their mood swings (Melrose, n.d.). It is a lifelong condition that the person needs to learn how to manage it with effective strategies and medications.
Signs and Symptoms of a Manic Episode
- Rapid speech
- Hyperactivity
- Reduced need for sleep
- Flight of ideas
- Grandiosity
- Poor judgment
- Aggression/hostility
- Risky sexual behavior
- Neglect basic self-care
- Decreased impulse control
Treatment for a client diagnosed with bipolar may include medications, safety initiatives during acute mania, electroconvulsive therapy (ECT), psychotherapy, and support groups. The severity of manic and depressive episodes varies for each client. Assessing if a client is a danger to others or themselves is the priority. People with bipolar may need assistance with impulse control during times when they are in a manic state (Varcarolis, 2017).
Learn more about bipolar disorder from the Canadian Mental Health Association
Watch the video Mental Health Minute: bipolar disorder [1:00] by National Institute of Mental Health (NIMH) (2021).
Schizophrenia
Severe mental health illnesses such as schizophrenia can be very debilitating and can impact the persons ability to function in society. Schizophrenia refers to a group of severe, disabling psychiatric disorders marked by hallucinations, delusions, disorganized speech, grossly disorganized behavior, and negative signs and symptoms such as reduced emotional expression, avolition (significant lack of motivation), and cognitive impairment (Haney & Risvi, 2024). Schizophrenia affects people from all walks of life and usually first appears in between the ages of 15 and 30 and is more common in men. Not everyone will experience the same psychotic symptoms. Psychoses are defined as a loss of reality characterized by:
- Delusions (fixed false beliefs that cannot be changed through reasoning),
- Hallucinations (hearing, seeing, smelling, tasting, or feeling touched by things that are not there)
- Lack of insight and judgment (withdrawal from reality, illogical thinking)
- Mood and affect (lack of observable expressions of emotions, monotone voice, expressionless face, immobile body)
(Adams et al, 2019; Melrose, n.d.)
The cause of schizophrenia is multifaceted, with both genetic, neurobiological and environmental factors considered. It is a polygenic disorder thereby there is not one gene responsible, but many genetic mutations contributing to the condition. Structural and functional brain abnormalities are also a factor, with less gray matter in the frontal, temporal and hippocampus regions. Another possible factor is environmental such as complications at birth and early life challenges. Lastly, cannabis or its psychoactive ingredient, tetrahydrocannabinol (THC) can be a contributing factor to psychoses, especially for those using cannabis at an early age and in large amounts. Cannabis can induce psychotic episodes or may exacerbate preexisting psychotic conditions. There is a 6 times greater risk of schizophrenia for people who begin using large amounts of cannabis at an early age, compared to nonusers (Casadio et al, 2011). As such, cannabis use during adolescence can pose a risk for those more vulnerable. In summary, the mix of genetic and environmental factors during early brain development increases the potential for schizophrenia.
Diagnosing Schizophrenia
A comprehensive health history, a mental status examination (MSE), and a physical examination must be completed to rule out other conditions and to make a diagnosis (Hany & Rizvi, 2024).
Health history: presenting symptoms, past psychiatric history, substance use, medical conditions, medications (current and past, adherence), family history, personal and social factors and developmental history (childbirth complications, early development).
Mental Status Examination – the MSE is a standard tool to assess the client’s current cognitive, affective and behavioural functioning. MSE will be done as part of initial assessment, and then repeated at different times to evaluate clinical progress. There are 10 components to the exam: appearance, behaviour, motor activity, speech, mood and affect, thought process, thought content, perception, cognition, insight and judgment.
Click on the link to watch a clinician completing a MSE on a client: Psychosis (Schizophrenia) Mental Status Examination (MSE) [12:02] by Geeky Medics (2023).
There is no lab work that can help diagnose schizophrenia, but the addition of blood work can help rule out co-concurrent conditions.
Signs and Symptoms of Schizophrenia
There are three types of symptoms related to schizophrenia: positive, negative, and cognitive.
Positive Symptoms
Note that in this context, the word positive is not the same as good. Rather, positive symptoms are psychotic and demonstrate how the individual has lost touch with reality. Positive symptoms include:
- Delusions
- Hallucinations
- Disorganized thinking and behavior
Delusions fall into several categories. Individuals with a persecutory delusion may believe they are being tormented, followed, tricked, or spied on. Individuals with a grandiose delusion may believe they have special powers. Individuals with a reference delusion may believe that passages in books, newspapers, television shows, song lyrics, or other environmental cues are directed toward them. In delusions of thought withdrawal or thought insertion, individuals believe others are reading their mind, their thoughts are being transmitted to others, or outside forces are imposing their thoughts or impulses on them (Melrose, n.d.).
Hallucinations may include hearing, seeing, smelling, tasting, or feeling as if they have been touched by things that are not there (Melrose, n.d.).
Negative Symptoms
Negative symptoms are those characteristics that should be there but are lacking. Negative symptoms include:
- Apathy (lack of interest in people, things, activities)
- Lack of motivation
- Blunted affect
- Poverty of speech (brief replies)
- Anhedonia (lack of interest in activities once enjoyed)
- Avoidance of relationships
Keep in mind that the inability to show emotion associated with a blunted affect does not reflect an inability to feel emotion. Similarly, it is helpful to understand that withdrawing from others is a coping mechanism for an individual with schizophrenia and not a rejection of those who initiate contact (Melrose, n.d.).
Cognitive
Cognitive symptoms are a change in thought pattern and include:
- Poor decision making
- Loss of memory
- Distracted
- Difficulty focusing
Treatment for a client diagnosed with schizophrenia is lifelong and is aimed at relieving symptoms and enhancing client functioning. Treatment adherence is a challenge as once the client begins to feel better, they stop taking their medications, and symptoms resume. Also, many of the medications have undesirable side effects which can make adhering to the meds difficult. Non-pharmacological interventions include limit setting, addressing barriers to adherence, supported employment services, therapeutic communication, ECT, and psychotherapy. Antipsychotic medications are prescribed to control positive and/or negative signs and symptoms and require close monitoring for effect and client adherence.
Key assessments for a client with schizophrenia include examination for hallucinations and delusions, use of additional substances (alcohol or drugs), safety, their support system, and a medication review with a focus on compliance with their therapeutic regimen (Mayo Clinic, 2018; Varcarolis, 2017).
Learn more about schizophrenia from the Canadian Mental Health Association.
Seizures
The official definition of a seizure is “a transient occurrence of signs and/or symptoms due to an abnormal excessive or synchronous neuronal activity in the brain.” This means that during a seizure, large numbers of brain cells are activated abnormally at the same time. It is like an electrical storm in the brain. They may alter consciousness, alter sensation and produce abnormal motor activity.
Seizures are considered a symptom rather than a disorder in itself. Some causes of seizures can be from acute conditions such as infections, electrolyte disturbances, tumours, or trauma. Seizures that also occur on a chronic or ongoing basis, such as epilepsy. In some circumstances, the cause of seizures cannot be found. Seizures can have an impact of a person’s life, such as risk of injury, restrictions on the type of activities or work, and driving restrictions (Epilepsy Foundation, 2017). There are different classifications of seizures based on severity of symptoms.
Signs and Symptoms of Seizures
Motor Symptoms
- Jerking (clonic)
- Muscles becoming limp or weak (atonic)
- Tense or rigid muscles (tonic)
- Brief muscle twitching (myoclonus)
- Epileptic spasms
Non-motor Symptoms
- Changes in sensation, emotions, thinking, or autonomic functions
- Lack of movement
Classification of Seizures
Seizures are classified in many ways, beginning with whether they are focal or generalized seizures.
Focal Seizures (focal onset or partial seizures)
Focal onset seizures have focal onset on one side of the brain. They are further classified into simple, complex, or secondarily generalized:
- Simple partial seizures are most common. They may also affect sensory and autonomic systems.
- Complex partial seizures include impairment of consciousness, with or without motor activity or other signs.
- Simple or complex partial seizures may become secondarily generalized, producing a tonic-clonic seizure. Tonic-clonic seizures are usually preceded by an aura and are the most common type.
Generalized Seizures
Generalized seizures have bilateral onset on both sides of the brain and are typified by absence (formerly petit mal) seizures, atonic seizures (short, lasting minutes), or tonic-clonic seizures. Most often there is a loss of awareness (Epilepsy Foundation, 2019; Mayo Clinic Staff, 2019; Velarde, 2019).
Common terms to describe a seizure:
These muscular changes are often associated with generalized seizures, but can occur with partial seizures as well.
- Tonic: muscles become stiff
- Atonic: sudden unexpected loss of muscle strength or tone
- Myoclonic: short, lightening-quick, jerk movements
- Clonic: periods of rhythmic or jerking movements
Canadian Epilepsy Alliance, n.d.
Status Epilepticus
Status epilepticus is a state of repeated or continuous seizures. It is often defined operationally as a single seizure lasting more than 30 minutes or repeated seizures without recovery of consciousness. Prolonged status epilepticus impacts breathing due to prolonged muscle contractions, resulting in hypoxia, hypoglycemia, hypothermia due to increased metabolic needs and lactic acid production. If left untreated, can lead to irreversible brain injury and has a very high rate of mortality. The goal of therapy should be to achieve control of a seizure within 60 minutes or less. Pharmacological treatment of seizures is very successful in the majority of cases, but it requires accurate diagnosis and classification of seizures. Medication management of seizures may include CNS depressants, benzodiazepines or barbiturates, or anticonvulsants such as phenytoin (Velarde, 2019).
Learn more about seizures: Canadian Epilepsy Alliance https://www.canadianepilepsyalliance.org/about-epilepsy/types-of-seizures/
Neurodegenerative Diseases
Neurodegenerative diseases involve the progressive destruction of nerve cells. This includes Parkinson’s disease, Alzheimer’s disease and other dementias, and amyotrophic lateral sclerosis. These diseases typically begin in mid to late life and are progressive in nature. Each disease presents differently with a range of symptoms that could lead to cognitive, physical, emotional and behavioural decline.
The causes of neurodegenerative diseases are considered multifactorial, with genetic, environmental and lifestyle factors having a role. For example, toxin or chemical exposure, traumatic brain injury, poor diet, and aging may all contribute to the onset of disease. Unfortunately, there is much we do not know about many of these diseases. There is considerable research currently underway for Parkinson’s and other neurodegenerative diseases to find not only causative factors but improved treatments.
Exciting Research to change the future of neurodegenerative diseases
Current research is exploring how prions (misfolded proteins) contribute to some of these diseases such as Alzheimer’s disease, Parkinson’s disease, and amyotrophic lateral sclerosis. The prions can alter the normal structure of proteins in the brain, so it no longer functions properly. It also causes proteins to clump that leads to further damage to cells and eventual cell death (Society of Neuroscience, 2018).
Research by Zhittya Genesis Medicine exploring the use of angiogenesis to treat ALS and Parkinson’s. Currently in the human trial stage with Parkinson’s clients, this treatment uses fibroblast growth factor 1 (FGF-1) to grow new blood vessels in ischemic tissue in the brain, resulting in the reestablishment of blood flow in dopamine-producing parts of the brain. Early trials show improved motor function and cognition.
ALS Disease: Is Angiogenesis a Possible Treatment or Even a Cure?
Zhittya Genesis Medicine ALS Disease: Is Angiogenesis a Possible Treatment or Even a Cure?
Parkinson’s Disease
Parkinson’s disease (PD) is a chronic progressive disease of the nervous system that impairs one’s ability to move. The incidence increases with age, with the average age of onset around 60. Men are more susceptible than women. In 2022-2023, 110,000 people are living with the disease, and with the aging population in Canada, the incidence of Parkinsons is expected to increase (Government of Canada, 2025).
Parkinson’s results from a combination of genetic, environmental, lifestyle and other factors, contributing to a loss of dopamine-producing cells in the substantia nigra which is part of the midbrain. This brain region affects movement, reward, and addiction (Society of Neuroscience, 2018). Non-motor symptoms are attributed to loss of serotonergic, norepinephrine and cholinergic neurons in the cerebral cortex, brainstem, spinal cord and peripheral autonomic nervous system (Parkinson Canada, n.d.). The disease worsens over time and has no cure.
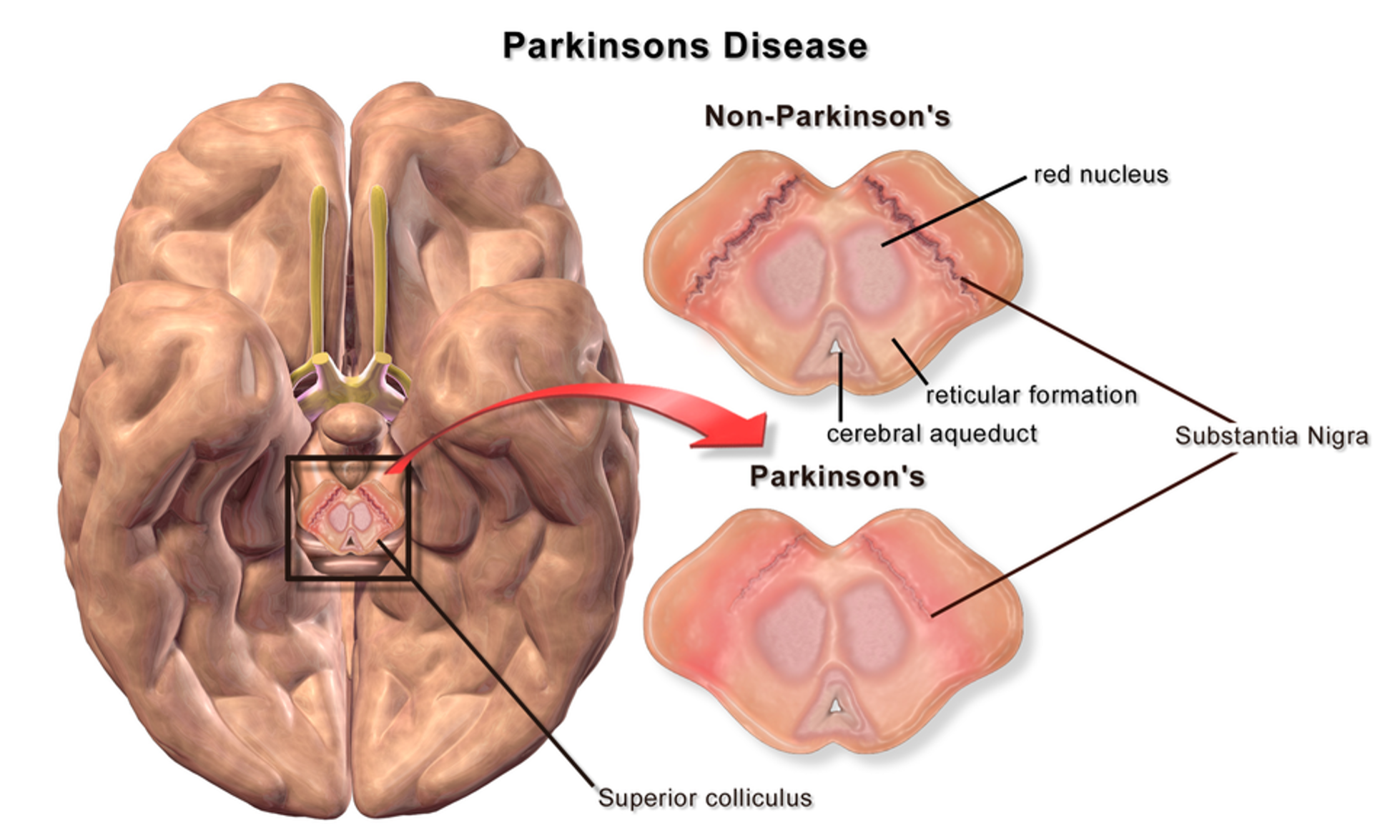
The early stage of the disease is characterized by motor problems, such as bradykinesia (slow movement), muscular rigidity, and unilateral or asymmetric resting tremor. A client who presents with two of the three symptoms likely has PD (Parkinson Canada, n.d.). Poor coordination and instability are also early symptoms. These symptoms progressively worsen. Along with motor issues, hyposmia, fatigue, depression, constipation and rapid eye movement sleep behaviour can also be present and may occur before motor symptoms develop. Cognitive decline often occurs in the later stages, with some people developing depression, memory loss and dementia. Other issues include problems with chewing and swallowing, constipation, urinary dysfunction and sleeping problems. The rate and extent of symptoms vary with some persons severely disabled and others with only minor symptoms (Government of Canada, 2025; Society of Neuroscience, 2018).
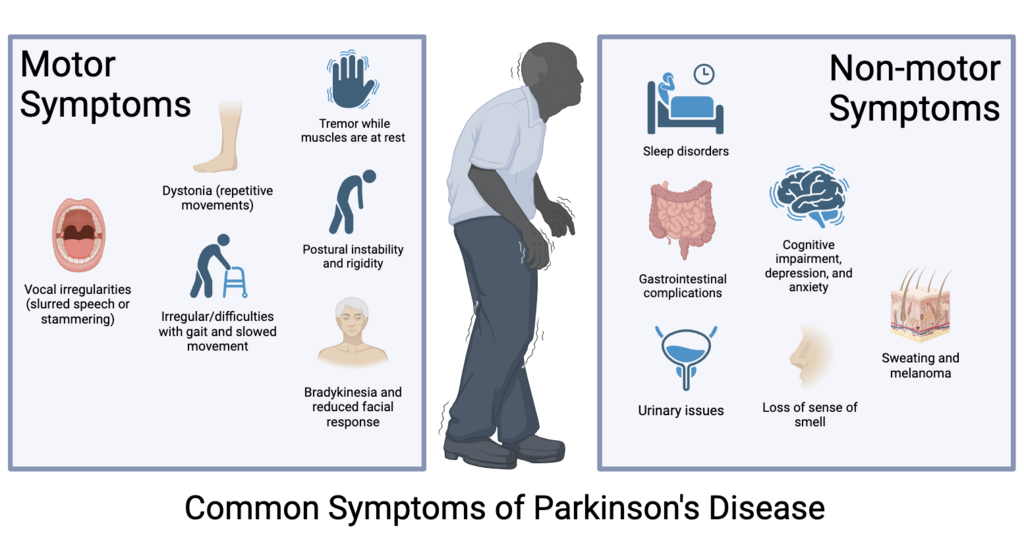
File:PD Symptoms.png File:PD Symptoms.png – Wikimedia Commons Creative Commons Attribution-Share Alike 4.0 International licens
Treatment
Treatment for a client with Parkinson’s disease will include medications to increase dopamine in the brain to slow the progression of the disease. Levodopa is typically prescribed to temporarily relieve motor symptoms but it does not slow the disease progression. Other medications that can be tried include dopamine agonists, MAO-B inhibitors, anticholinergics and NMDA antagonists. Other strategies include gene therapy and deep brain stimulation to treat clients who are not responsive to medications. Medications for Parkinson’s will be explored further in unit 5.10.
Watch the following video to learn more about the impact of Parkinson’s Disease
Michael J. Fox emerges from the darkness of Parkinson’s
YouTube·CBC News: The National·May 25, 2023
Alzheimer’s Disease
Alzheimer’s disease (AD) is a progressive, irreversible brain disorder that develops over years. It begins with memory loss and confusion, and progresses to a decline in cognitive abilities, behaviour and personality changes, and a loss of ability to recognize family or friends. In the very late stages, some Alzheimer’s clients lose the ability to speak, walk and have difficulty eating. Alzheimer’s disease is the leading cause of dementia in the older population (National Institute of Neurological Disorders and Stroke, 2026).
Early onset AD can begin as early as the 30s or 40s and is attributed to an inherited gene mutation. Most AD is not genetic and begins with people older than 65. For late onset cases, genetic, environmental and lifestyle may be factors. Besides age of onset, the physiological changes and disease progression are the same.
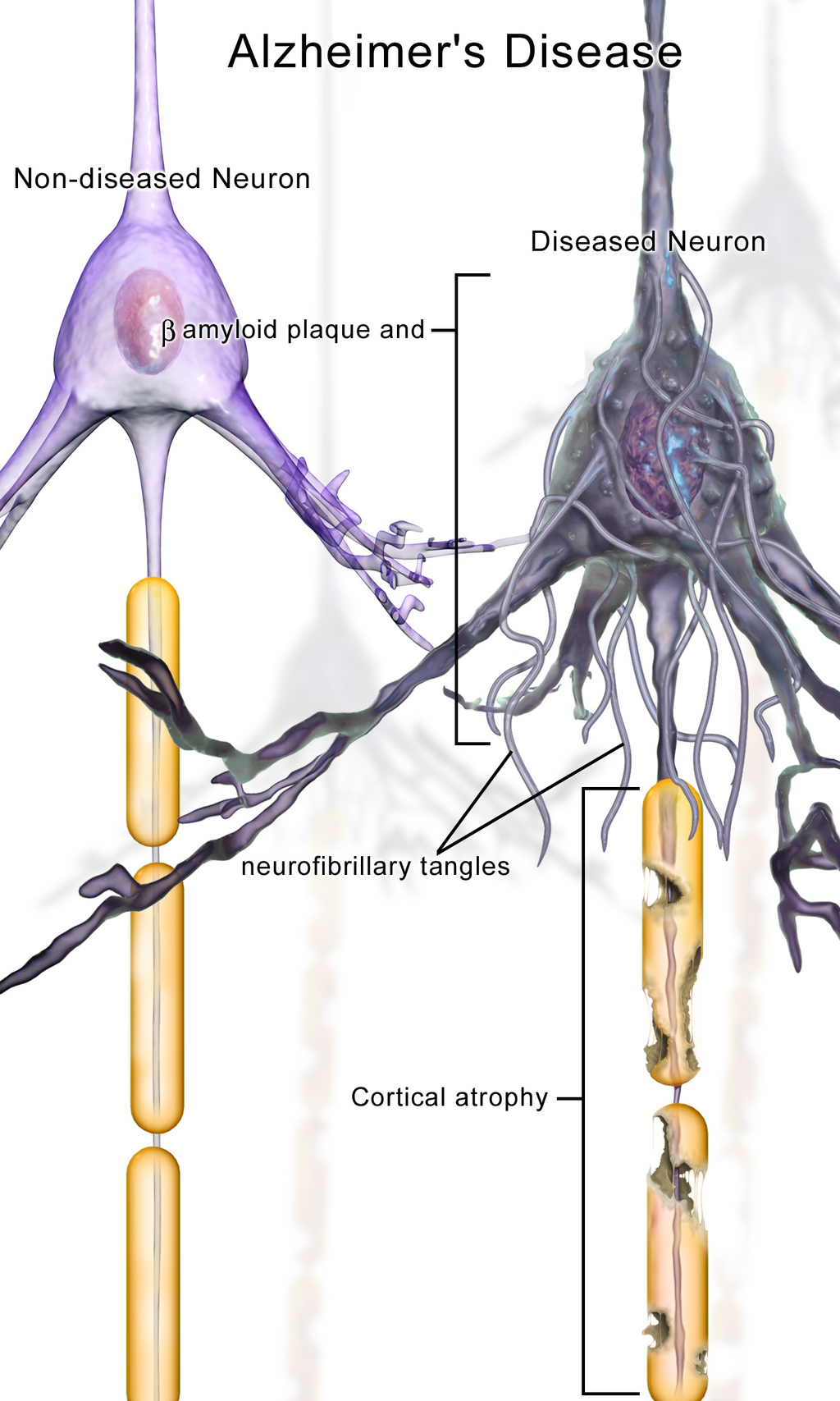
AD is characterized by the accumulation of abnormal protein aggregates in the brain. These comprise beta-amyloid plaques and tau tangles. Amyloid plaques, which are made up of fragments of a protein called beta-amyloid peptide mixed with a collection of additional proteins, remnants of neurons, and bits and pieces of other nerve cells. Tau, which is required for healthy neurons, clump together in the neuron becoming neurofibrillary tangles (NFTs).
These deposits hinder the normal passage of impulses among nerve cells, leading to a loss of connections between neurons which are responsible for memory and learning. Without the connections, neurons die throughout the brain, and the affected regions atrophy. In the latter stages of the disease, the damage is widespread, leading to cell death and gradual deterioration of brain tissue (Gadhave et al, 2024).
Treatment
There is no treatment to prevent Alzheimer’s disease, only medications to slow the progression. These meds are only effective for a few years, but can help improve the ability to carry out activities of daily living, memory and behavioural changes.
For mild to moderate AD symptoms, cholinesterase inhibitors: donepezil (Aricept), rivastigmine (Exelon), and galantamine are prescribed to boost brain acetylcholine levels, leading to improved memory and thinking. Immunotherapy has also been prescribed for early-stage clients that work to remove amyloid plaques. Lecanemab and donanemab are two immunotherapy drugs.
For moderate-severe AD symptoms, memantine, a N-methyl-D-aspartate (NMDA) antagonist, helps regulate glutamate and can improve functioning for a short time (National Institute of Aging, 2023). There is currently considerable research on preventing the onset or treating the symptoms of Alzheimer’s Disease.
Potential new treatment of proteins in Alzheimer’s and Parkinson’s disease
For proteins to function correctly, they are dependent on their three-dimensional shape. The linear sequence of amino acids folds into a three-dimensional shape that is based on the interactions between and among those amino acids. When the folding is disturbed and proteins take on a different shape, they stop functioning correctly. But the disease is not necessarily the result of functional loss of these proteins; rather, these altered proteins start to accumulate and may become toxic. For example, in Alzheimer’s the hallmark of the disease is the accumulation of these amyloid plaques in the cerebral cortex. The term coined to describe this sort of disease is “proteopathy” and it includes other diseases. Creutzfeld-Jacob disease, the human variant of the disease known as mad cow disease, also involves the accumulation of amyloid plaques, similar to Alzheimer’s. Diseases of other organ systems can fall into this group as well, such as cystic fibrosis or type 2 diabetes. Recognizing the relationship between these diseases has suggested new therapeutic possibilities. Interfering with the accumulation of the proteins, and possibly as early as their original production within the cell, may unlock new ways to alleviate these devastating diseases (OpenStax, 2025).
References:
- Canadian Psychological Association (2021). Psychology works fact sheet: depression. https://cpa.ca/psychology-works-fact-sheet-depression/
- Casadio P., Fernandes, C., Murray, RM, Di Forti, M. (2011). Cannabis use in young people: the risk for schizophrenia. Neuroscience Biobehavioural Review, 35(8), 1779-87. doi: 10.1016/j.neubiorev.2011.04.007. PMID: 21530584.
- Chand; S. & Arif, H. (2023). Depression. National Library of Medicine. StatPearls. Retrieved at: https://www.ncbi.nlm.nih.gov/books/NBK430847/
- Chand, A., Marwaha, R., Bender, R. (2023). Anxiety (Nursing). National Library of Medicine. StatPearls. Treasure Island, Fl). Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK568761/
- Epilepsy Foundation. (2016, December 22). 2017 Revised classification of seizures. https://www.epilepsy.com/article/2016/12/2017-revised-classification-seizures ↵
- Gadhave, D., Sugandhi, V., Kumar, S., Nangare, S., Gupta, G. et al. (2024). Neurodegenerative disorders: Mechanisms of degeneration and therapeutic approaches with their clinical relevance. Aging Research Reviews, 99, 102357.
- Government of Canada (2025). Parkinsonism in Canada, including Parkinson Disease. Health Infobase. Retrieved from https://health-infobase.canada.ca/datalab/parkinson-blog.html
- Haney, M. & Risvi, A. (2024). Schizophrenia. National Library of Medicine. StatPearls [internet]. https://www.ncbi.nlm.nih.gov/books/NBK539864/
- Khan Academy (n.d.). Introduction to Mental Disorders. Licensed under CC BY-NC-SA 3.0. ↵
- Mayo Clinic Staff. (2018, May 4). Anxiety disorders. https://www.mayoclinic.org/diseases-conditions/anxiety/symptoms-causes/syc-20350961 ↵
- Mayo Clinic Staff. (2019, June 25). Attention-deficit/hyperactivity disorder (ADHD) in children. https://www.mayoclinic.org/diseases-conditions/adhd/symptoms-causes/syc-20350889
- Mayo Clinic Staff. (2018, January 31)) Bipolar disorder. https://www.mayoclinic.org/diseases-conditions/bipolar-disorder/symptoms-causes/syc-20355955 ↵
- Mayo Clinic Staff. (2018, February 3). Depression. https://www.mayoclinic.org/diseases-conditions/depression/symptoms-causes/syc-20356007 ↵
- Mayo Clinic (2025, June 21). Lewy body dementia. https://www.mayoclinic.org/diseases-conditions/lewy-body-dementia/symptoms-causes/syc-20352025
- Mayo Clinic Staff. (2020, January 7) Schizophrenia. https://www.mayoclinic.org/diseases-conditions/schizophrenia/diagnosis-treatment/drc-20354449 ↵
- Mayo Clinic Staff. (2019, June 18). Seizures. https://www.mayoclinic.org/diseases-conditions/seizure/symptoms-causes/syc-20365711 ↵
- Mayo Clinic Staff. (2018, June 30). Parkinson’s disease. https://www.mayoclinic.org/diseases-conditions/parkinsons-disease/symptoms-causes/syc-20376055
- McCuistion, L., Vuljoin-DiMaggio, K., Winton, M, & Yeager, J. (2018). Pharmacology: A patient-centered nursing process approach. pp. 227-305. Elsevier. ↵
- Melrose, S. (n.d.). An overview of mental illness. Supporting Individuals with Intellectual Disability & Mental illness. Licensed under CC BY 4.0. ↵
- National Institute of Aging (2023). How is Alzheimer’s disease treated? How Is Alzheimer’s Disease Treated? | National Institute on Aging
- OpenStax (2025). Anatomy and Physiology. Licensed under CC BY 4.0.
- https://openstax.org/books/anatomy-and-physiology/pages/1-introduction ↵
- Rosow, C., Standeart, D. & Strichartz, G. (n.d.). Principles of Pharmacology. LibreTexts. CC BY-NC-SA 4.0. ↵
- Society of Neuroscience (2018). Brain Facts (8th ed.). Washington, DC. https://www.brainfacts.org/the-brain-facts-book
- Statistics Canada (2015). Childhood conditions. Part 1: attention-deficit/hyperactivity disorder. https://www150.statcan.gc.ca/n1/pub/82-619-m/2012004/sections/sectionc-eng.htm#a1
- Statistics Canada (2025). Mental disorders and access to mental health care. https://www150.statcan.gc.ca/n1/daily-quotidien/230922/dq230922b-eng.htm
- Stephenson, E. (2023). Mental health disorders and access to mental health care. Insights on Canadian Society. Statistics Canada, 75-006-X. https://www150.statcan.gc.ca/n1/pub/75-006-x/2023001/article/00011-eng.htm
- Varcarolis, E. M. (2017). Essentials of psychiatric mental health nursing: a communication approach to evidence-based care. pp. 255-324. Elsevier. ↵
- Velarde, G. (2019, May 20). Pharmacology Notes: Nursing Implications for Clinical Practice. OER Commons. Retrieved January 14, 2026, from https://oercommons.org/authoring/54330-pharmacology-notes-nursing-implications-for-clinic.
- World Health Organization (2026). Mental Health. https://www.who.int/health-topics/mental-health#tab=tab_1
Media Attributions:
- “stress-2902537_960_720.jpg” by TheDigitalArtist is licensed under CC0 1.0 ↵
- “RightBrainDominant.jpg” by ElisaRiva is licensed under CC0 ↵
- https://www.rawpixel.com/image/5957375/free-public-domain-cc0-photo by Rawpixel licensed under CC0 1.0 Universal
- 8.3c File:Blausen 0704 ParkinsonsDisease.png Blausen.com staff (2014). “Medical gallery of Blausen Medical 2014“. WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436.
- 8.3d PD Symptoms.png File:PD Symptoms.png – Wikimedia Commons Creative Commons Attribution-Share Alike 4.0 International license
- File:Blausen 0017 AlzheimersDisease.png File:Blausen 0017 AlzheimersDisease.png – Wikimedia Commons
- 8.3e Blausen 0017 AlzheimersDisease.png File:Blausen 0017 AlzheimersDisease.png – Wikimedia Commons

{kind=link}
{kind=link}
{kind=link}