8.2 Conditions and Diseases Related to the Respiratory System V2
The upper respiratory airways involve the nose, mouth and throat. Conditions that affect the upper respiratory system include the common cold, allergic rhinitis, and sinusitis and are usually involve an inflammatory response that affects the mucosal layer of the airways. These conditions are often self-limiting but can result in breathing difficulties and other respiratory symptoms.
The lower respiratory airways the trachea and the lungs, which includes the bronchi, bronchioles, and alveoli. Some of the most common lower respiratory conditions are asthma and chronic obstructive pulmonary disease (COPD), which includes emphysema and chronic bronchitis.
In this unit, we will review conditions that affect the upper respiratory system including allergies and the common cold. We will also review conditions that affect the lower respiratory system including asthma, bronchitis and chronic obstructive respiratory disease (COPD).
To begin, we will discuss anaphylaxis, which is a potentially life-threatening medical emergency.
Anaphylaxis
Some types of allergies, including allergies to foods and insect stings, can trigger a severe reaction known as anaphylaxis. As a life-threatening medical emergency, anaphylaxis can cause a client to go into shock. There are a number of common triggers that can precipitate the IgE-mediated (type 1) hypersensitivity reaction. These include food (shellfish, peanuts, eggs, wheat), latex, and insect stings or bites.
Signs and symptoms of anaphylaxis include:
- Loss of consciousness
- Drop in blood pressure
- Severe shortness of breath
- Skin rash or itching
- Light-headedness
- Rapid, weak pulse
- Nausea and vomiting
Symptoms often begin mildly, with a cough, runny nose, rash or even a lump in the throat. It can then progress quickly to more serious symptoms.
Anaphylaxis involves the release of numerous chemical mediators from the degranulation of basophils and mast cells after re-exposure to a specific antigen. IgE crosslinking and resultant aggregation of high-affinity receptors induce the rapid release of stored chemical mediators. These chemical mediators include histamine, tryptase, carboxypeptidase A, and proteoglycans. The resulting inflammatory response includes:
- Histamine release that increases vascular permeability and vasodilation, leading to tissue hypoperfusion. The body responds to these changes by increasing heart rate and cardiac contraction.
- Prostaglandin D functions as a bronchoconstrictor, simultaneously constricting cardiac and pulmonary arteries. It also potentiates peripheral vasodilation, contributing to the hypoperfusion of vital organs.
- Leukotrienes add to bronchoconstriction and vascular permeability and induce airway remodeling.
- The platelet activation factor also acts as a bronchoconstrictor and increases vascular permeability.
- TNF-alpha activates neutrophils (as part of stress response leukocytosis) and increases chemokine synthesis.
(McLendon & Sternard, 2023)
Rapid treatment within the first hour of exposure is crucial. Treatment is with epinephrine intramuscular (IM) and airway management. Often only one dose of epinephrine is needed but it can be repeated. Typical dose is epinephrine 0.3 to 0.5 mL of 1:1,000 concentration intramuscular into the thigh.
Following the initial reaction, anaphylactic reactions can also occur biphasically, meaning there is a reoccurrence of symptoms 8-11 hours after the initial reaction (McLendon & Sternard, 2023). Clients who are treated in the ED are usually observed until the risk of a second reaction has passed.
Upper Respiratory System Disorders Include Allergies and the Common Cold
Allergies
Allergies occur when your immune system reacts to a foreign substance – such as pollen, bee venom, pet dander, or food – that doesn’t cause a reaction in most people.
Your immune system produces substances known as antibodies. When you have allergies, your immune system makes antibodies that identify a particular allergen as harmful, even though it isn’t. When you come into contact with the allergen, your immune system’s reaction can inflame your skin, sinuses, airways, or digestive system.
The severity of allergies varies from person to person and can range from minor irritation to a potentially life-threatening emergency. While most allergies can’t be cured, treatments can help relieve allergy symptoms.
Allergy symptoms, which depend on the substance involved, can affect airways, sinuses, and nasal passages, skin, and the digestive system (Mayo Clinic Staff, 2018a).
Hay fever, also called allergic rhinitis, is an inflammatory disorder, often triggered by an airborne allergen. It is the most common allergic disorder. It can cause:
- Sneezing
- Itching of the nose, eyes, or roof of the mouth
- Runny, stuffy nose
- Watery, red or swollen eyes (conjunctivitis)
A food allergy can cause:
- Tingling in the mouth
- Swelling of the lips, tongue, face, or throat
- Hives
- Anaphylaxis
An insect sting allergy can cause:
- Large area of swelling (edema) at the sting site
- Itching or hives all over the body
- Cough, chest tightness, wheezing, or shortness of breath
- Anaphylaxis
A drug allergy can cause:
- Hives
- Itchy skin
- Rash
- Facial swelling
- Wheezing
- Anaphylaxis
Atopic dermatitis, an allergic skin condition also called eczema, can cause skin to:
- Itch
- Redden
- Flake or peel
Treatment can include intranasal glucocorticoids, antihistamines (oral and nasal) and sympathomimetics (phenylephrine, pseudoephedrine) (Rosenjack Burchum & Rosenthal, 2019).
Common Cold
The common cold is a viral infection of the upper respiratory tract. There are over 100 types of viruses can cause a common cold. Viruses that can cause a cold include rhinoviruses, coronavirus, and enterovirus among many others(Tobin, Thomas & Bomar, 2025).
Children younger than 6 are at greatest risk of colds, but healthy adults can also expect to have two or three colds annually. Most people recover from a common cold in a week or 10 days. Symptoms might last longer in people who smoke due to impaired mucociliary function and impaired immune function.
Symptoms of a common cold usually appear one to three days after exposure to a cold-causing virus. Signs and symptoms, which can vary from person to person, might include:
- Runny or stuffy nose, sore throat, cough, congestion
- Slight body aches or a mild headache, low-grade fever, malaise
- Sneezing
(Mayo Clinic, 2019a).
Symptoms can be mild to moderate, but usually self-limiting. Treatment includes non-steroidal anti-inflammatories to treat general discomfort and fever, antihistamines, anticholinergics, and antitussives, all with the goal of symptom relief (Tobin, Thomas & Bomar, 2025).
Lower respiratory system disorders include asthma, bronchitis and chronic obstructive respiratory disease (COPD).
Asthma
Asthma is a chronic respiratory disorder affecting the lungs of both children and adults. It starts with an immune response to an allergen that leads to inflammation, edema, and bronchospasm of the airways, which inhibits air from entering the lungs. In addition, excessive mucus secretion can occur, which further contributes to airway blockage. Cells of the immune system, such as eosinophils and mononuclear cells, are also involved in infiltrating the walls of the bronchi and bronchioles. Airway inflammation is the primary issue in asthma.
Bronchospasms occur periodically and lead to an “asthma attack.” An attack may be triggered by environmental factors such as dust, pollen, pet hair, or dander; changes in the weather; mold; tobacco smoke; respiratory infections; exercise; and stress (Open Stax, n.d.).
Along with asthma, many people with asthma are more likely to have other chronic diseases or conditions such as diabetes, hypertension, and mood or anxiety disorders. These conditions can make asthma symptoms worse or impede effective treatment (Ontario Health, 2025).
Symptoms of an asthma attack involve coughing, shortness of breath, wheezing, and tightness of the chest. Symptoms of a severe asthma attack that requiring immediate medical attention include difficulty breathing that results in cyanotic lips or face, confusion, drowsiness, a rapid pulse, sweating, and severe anxiety.
The severity of the condition, frequency of attacks, and identified triggers influence the type of medication that an individual may require. Asthma is classified based on the severity of the disease. This includes very mild, mild, moderate, and severe which helps direct medication management.
Good asthma control is crucial. When inflammation is uncontrolled, tissues undergo remodeling which leads to permanent structural changes to the bronchi and thus permanent alteration in lung function.

Figure 8.3b The effects of asthma on airways. This image shows an airway on the left unaffected, and an airway on the right impacted by bronchoconstriction and mucous. https://commons.wikimedia.org/wiki/File:Asthma_(Lungs).png
For more information on diagnosis, treatment and management of asthma: Government of BC (2023). Asthma Diagnosis, Education and Management. BC Guidelines.ca Asthma Diagnosis, Education and Management – Province of British Columbia
Diagnosing Asthma
Management begins with an accurate diagnosis. This includes a thorough clinical history, physical examination and lung function tests that may include spirometry, peak flow meter test (estimates peak expiratory flow rate), assessments of airway hyperresponsiveness, sputum eosinophil levels, blood eosinophil levels, and chest X-rays (Sun, Sun & Wang, 2023).
Peak Flow Monitoring:
Peak flow monitoring is the use of a peak flow monitor to estimate the ability to push air out of the lungs (PEFR).
Peak expiratory flow (PEF): measures the maximum speed of expiration using a peak expiratory flow meter. The peak airflow will decrease during expiration if airways are blocked due to airway inflammation or bronchoconstriction (Asthma Canada, 2026). The device can be used at home and is also often used in the ED as part of a respiratory assessment.
Symptoms that suggest asthma:
- Frequent episodes of breathlessness, chest tightness, wheezing or cough
- Symptoms worse at night and in the early morning
- Symptoms develop with a viral respiratory tract infection, after exercise, or exposure to aero-allergens or irritants.
- Symptoms improve with bronchodilators or corticosteroids
(Canadian Thoracic Society, 2017)
Following a diagnosis, regular reassessment of control and risk of exacerbation is important. Further, all clients with asthma should have a self-management education that includes a written action plan, environmental triggers avoidance, and inhaler technique training (Canadian Thoracic Society, 2021).
Medications are given to increase airflow by:
- Bronchodilation (beta 2 adrenergic, anticholinergics)
- Decrease mucous production (corticosteroids inhaled or oral and anticholinergics)
- Decrease immune response (corticosteroids, antileukotrienes)
Treatment is on a continuum.
If symptoms are controlled, the client will take a controller (daily inhaled corticosteroid) plus a PRN rescue med short acting beta adrenergic.
If symptoms are less controlled, the inhaled corticosteroid dose may be increased and a long acting beta adrenergic med might be added.
View the following video for additional insight into how asthma works.
Bronchitis
Bronchitis is an inflammation of the lining of the bronchial tubes, which carry air to and from the lungs. People who have bronchitis often cough up thickened mucus, which can be discolored. Bronchitis may be either acute or chronic.
Often developing from a cold or other respiratory infection, acute bronchitis is very common. Acute bronchitis, also called a chest cold, usually improves within a week to 10 days without lasting effects, although the cough may linger for weeks.
Chronic bronchitis, a more serious condition, is a constant irritation or inflammation of the lining of the bronchial tubes, often due to smoking. Chronic bronchitis is one of the conditions included in COPD (Mayo Clinic Staff, 2017).
Symptoms for either acute bronchitis or chronic bronchitis may include:
- Cough
- Production of mucus (sputum), which can be clear, white, yellowish-gray, or green in color — rarely, it may be streaked with blood
- Fatigue
- Shortness of breath
- Slight fever and chills
- Chest discomfort
Chronic Obstructive Pulmonary Disease
Chronic Obstructive Pulmonary Disease (COPD) is a slowly progressing, chronic inflammatory lung disease that causes obstructed airflow out of the lungs. It is an umbrella term for progressive respiratory diseases that include emphysema and bronchitis. The primary cause of COPD is tobacco smoking, including second hand smoke or passive exposure (Government of Canada, 2018).
Symptoms include breathing difficulty, cough, mucus (sputum) production, and wheezing. It is often caused by long-term exposure to irritating gases or dust, and most often occurs due to smoking. People with COPD are at increased risk of developing heart disease, lung cancer, and a variety of other conditions.
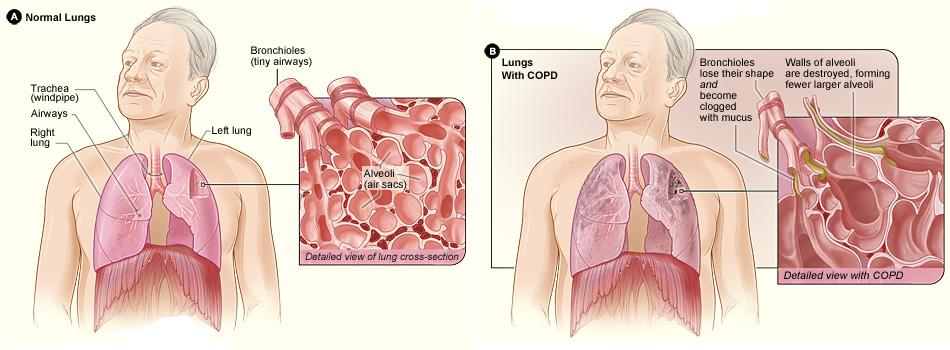
Emphysema and chronic bronchitis are the two types of COPD. Emphysema is a condition in which the alveoli at the end of the smallest air passages (bronchioles) of the lungs are destroyed and hyperinflated. Chronic bronchitis is inflammation of the lining of the bronchial tubes, characterized by daily cough and mucus (sputum) production. See Figure 8.3c for an illustration of normal lungs compared to lungs with COPD.
COPD begins with prolonged exposure to noxious inhaled particles. Overtime, there is a progressive airflow limitation and tissue destruction due to pulmonary inflammation, increased mucous, and decreased muco-ciliary function. Persistent inflammation and chronic infections eventually lead to remodelling, permanent scarring, decreased alveoli elasticity and decreased lung recoil.
COPD is treatable but not curable. COPD symptoms often don’t appear until significant lung damage has occurred, and they usually worsen over time, particularly if smoke exposure continues.
Other signs and symptoms of COPD may include:
- Shortness of breath, especially during physical activities
- Wheezing
- Chest tightness
- Chronic cough that may produce mucus (sputum) that may be clear, white, yellow, or greenish
- Cyanosis
- Frequent respiratory infections
- Lack of energy
- Unintended weight loss (in later stages)
Persons with COPD are at risk for respiratory infections due to chronic inflammation, increased mucous production and impaired ciliary function associated with the disease. Damage to the pulmonary vasculature can also lead to other respiratory conditions including pulmonary hypertension, cor pulmonale, hypoxia and hypercapnia (Sealock & Seneviratne, 2021).
Unlike some diseases, COPD has a clear cause and a clear path of prevention. The majority of cases are directly related to cigarette smoking, and the best way to prevent COPD is to never smoke — or to teach clients to stop smoking now (Mayo Staff Clinic, 2017b).
Everyday Connection: The Effects of Second-Hand Tobacco Smoke
The burning of a tobacco cigarette creates multiple chemical compounds that are released through mainstream smoke, which is inhaled by the smoker, and through sidestream smoke, which is the smoke that is given off by the burning cigarette. Second-hand smoke, which is a combination of side stream smoke and the mainstream smoke that is exhaled by the smoker, has been demonstrated by numerous scientific studies to cause disease. At least 40 chemicals in side stream smoke have been identified that negatively impact human health, leading to the development of cancer or other conditions, such as immune system dysfunction, liver toxicity, cardiac arrhythmias, pulmonary edema, and neurological dysfunction. Furthermore, second-hand smoke has been found to harbor at least 250 compounds that are known to be toxic, carcinogenic, or both. Some major classes of carcinogens in second-hand smoke are polyaromatic hydrocarbons (PAHs), N-nitrosamines, aromatic amines, formaldehyde, and acetaldehyde.
Tobacco and second-hand smoke are considered to be carcinogenic. Exposure to second-hand smoke can cause lung cancer in individuals who are not tobacco users themselves. It is estimated that the risk of developing lung cancer is increased by up to 30 percent in nonsmokers who live with an individual who smokes in the house, as compared to nonsmokers who are not regularly exposed to second-hand smoke. Children are especially affected by second-hand smoke. Children who live with an individual who smokes inside the home have a larger number of lower respiratory infections, which are associated with hospitalizations, and higher risk of sudden infant death syndrome (SIDS). Second-hand smoke in the home has also been linked to a greater number of ear infections in children, as well as worsening symptoms of asthma (Open Stax, n.d.).
Medications for treatment depends on symptoms and respiratory function diagnostic results. As the disease progresses, more medications are added. Medications include:
- maximizing gas exchange. This includes:
- short-acting beta-2 adrenergic (SABA) inhalers
- long-acting beta-2 adrenergic (LABA) inhalers.
- long-acting muscarinic antagonists (LAMA)
- inhaled corticosteroids (ICS)
- expectorants to increase airway patency and to facilitate secretion removal
Example in practice:
A 60-year-old client, Francois, is diagnosed with COPD and is started on a LAMA medication, tiotropium bromide. They are also prescribed a SABA, salbutamol. They take their LAMA daily, and use the SABA for an onset of SOB or wheezes and can use it 1-2 times/week.
After a year, Francois finds he takes salbutamol more than 2 times/week, and has more fatigue. The prescriber will add the LABA, salmeterol, to improve the overall management. He will continue to take his LAMA and SABA as prescribed.
Over time, and as Francois’s condition deteriorates, his dosages of the meds will be increased, and an inhaled corticosteroid may be added to further decrease the inflammation and mucous.
Interactive Activity
Image Descriptions
Figure 8.3a Common triggers of asthma. People have different triggers to asthma that can include smoke, pet dander, pollution, stress, fungal spores, chemical fumes, dust and exercise.
Figure 8.3b How Asthma Affects the Airway – Image Description
A normal airway has relaxed smooth muscles. Asthmatic airway has relaxed smooth muscles with inside wall inflamed and thickened. During an asthma attack, air is trapped in alveoli and the smooth muscles tighten. [Return to Figure 8.3a]
Figure 8.3c Normal lungs compared with lungs in a person with COPD. Figure A shows the location of the lungs and airways in the body. The inset image shows a detailed cross-section of the bronchioles and alveoli. Figure B shows lungs damaged by COPD. The inset image shows a detailed cross-section of the damaged bronchioles and alveolar walls.
Media Attributions
Figure 8.3a Common triggers of asthma File:Asthma triggers 2.PNG – Wikimedia Commons
Figure 8.3b How Asthma Affects the Airways https://commons.wikimedia.org/wiki/File:Asthma_(Lungs).png
Figure 8.3c Normal lungs compared with lungs in a person with COPD. “Copd 2010Side.JPG” by National Heart Lung and Blood Institute is licensed under CC0 ↵
- TED-Ed. (2017, May 11). How does asthma work? – Christopher E. Gaw. [Video]. YouTube. https://youtu.be/PzfLDi-sL3w ↵
- “Asthma and Your Airways” by unknown, is licensed under CC BY-NC-SA 3.0 Access for free at https://humannhealth.com/what-you-need-to-know-about-asthma/341/ ↵
References
- Asthma Canada (2026). How to monitor your asthma. https://asthma.ca/get-help/living-with-asthma/peak-flow-meters/
- Canadian Thoracic Society (2017). Canadian Respiratory Guidelines. Recommendations for the diagnosis and management of asthma. https://cts-sct.ca/wp-content/uploads/2018/07/5156_THOR-Asthma-sj_0318_11.875×9-en-web.pdf
- Government of British Columbia (2026). Asthma Diagnosis, Education and Management. BC guidelines.ca. https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/asthma
- Government of Canada (2018). Chronic obstructive pulmonary disease (COPD). Public Health Agency of Canada. Chronic Obstructive Pulmonary Disease (COPD) – Canada.ca
- Government of BC (2023). Asthma Diagnosis, Education and Management. BC Guidelines.ca Asthma Diagnosis, Education and Management – Province of British Columbia
- Mayo Clinic Staff. (2018, January 6). Allergies. https://www.mayoclinic.org/diseases-conditions/allergies/symptoms-causes/syc-20351497 ↵
- Mayo Clinic Staff. (2017a, April 11). Bronchitis. https://www.mayoclinic.org/diseases-conditions/bronchitis/symptoms-causes/syc-20355566
- Mayo Clinic Staff. (2019, April 20). Common cold. https://www.mayoclinic.org/diseases-conditions/common-cold/symptoms-causes/syc-20351605 ↵
- Mayo Clinic Staff. (2017b, August 11). COPD. https://www.mayoclinic.org/diseases-conditions/copd/symptoms-causes/syc-20353679 ↵
- McLendon, K. & Sternard, B. (2023). Anaphylaxis. National Library of Medicine. StatPearls. Anaphylaxis – StatPearls – NCBI Bookshelf
- Open Stax (n.d.). Anatomy and Physiology. Licensed under CC BY 4.0. Access for free at https://openstax.org/books/anatomy-and-physiology/pages/1-introduction
- Rosenjack Burchum, J., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
- Sealock, K. & Seneviratne, C. (2021). Lilley’s Pharmacology for Canadian Health Care Practice (4th ed.). Elsevier: Canada
- Sun, D., Sun. P. & Wang, Z. (2023). Assessment and therapeutic management of acute asthma: the approaches of nursing staff in patient care. Advances in Clinical and Experimental Medicine, ISSN 1899–5276 (print), ISSN 2451–2680 (online).
- Tobin, E. Thomas, M. & Bomar, P. (2025). Upper respiratory tract infections with focus on the common cold. National Library of Medicine. StatPearls [Internet]. Upper Respiratory Tract Infections With Focus on The Common Cold – StatPearls – NCBI Bookshelf
- Yang, C., Hicks, E., Mitchell, P., Reisman, J., Podgers, D. et al. (2021). Canadian Thoracic Society 2021 Guideline update: Diagnosis and management of asthma in preschoolers, children and adults. Canadian Journal of Respiratory, Critical Care, and Sleep Medicine. 5:6, 348-361, DOI: 10.1080/24745332.2021.1945887
Allergies occur when the immune system reacts to a foreign substance and makes antibodies that identify a particular allergen as harmful, even though it isn't.
A bluish or purplish discoloration (as of skin) due to deficient oxygenation of the blood.

{kind=link}
{kind=link}