7.2 Conditions and Disorders related to Perfusion V2
Perfusion refers to the process in which blood carries oxygen and nutrients to body tissues and organs and transports waste products of cellular metabolism away. Any disruption to the arterial blood supply through compromised cardiac output or a disruption to the vessels can lead to cardiovascular and cerebrovascular diseases. Cardiovascular disease (CVD) is a group of disorders of the heart and blood vessels and includes coronary artery disease (ischemic heart disease), cerebrovascular disease, peripheral vascular disease, deep vein thrombosis and congenital heart disease. Cardiovascular (CV) disease is a major cause of death and disability in Canada. According to 2017-2018 data from the Canadian Chronic Disease Surveillance System, about 8.5 % of Canadian adults are living with ischemic heart disease. It is the second leading cause of death, with 50,000 deaths per year (Government of Canada, 2022). Despite substantial advances in its prevention, diagnosis, and treatment, CVD remains a major cause of morbidity, mortality, and health care expenditure.
Atherosclerosis is the dominant underlying pathophysiology of CVD. There are 9 potentially modifiable risk factors that are attributed to 90% of the risk of the first myocardial infarction in both men and women. These are diabetes, hypertension, abdominal obesity, psychological stress, cigarette smoking, and dyslipidemia (ratio of apolipoprotein (apo) B (apoB) to apoA-I), physical inactivity, diet high in saturated fats or trans fats, and excessive alcohol use (Brunham, Lonn & Mehta, 2022).
In this unit, we will begin our review of some of the risk factors including dyslipidemia, atherosclerosis and hypertension. Common cardiac disorders will then be reviewed including angina pectoris, myocardial infarction, cerebrovascular accidents, thrombi and emboli, arrhythmias and heart failure. This is a brief review, so for more indepth understanding of each of these conditions, please refer to other resources.
Dyslipidemia
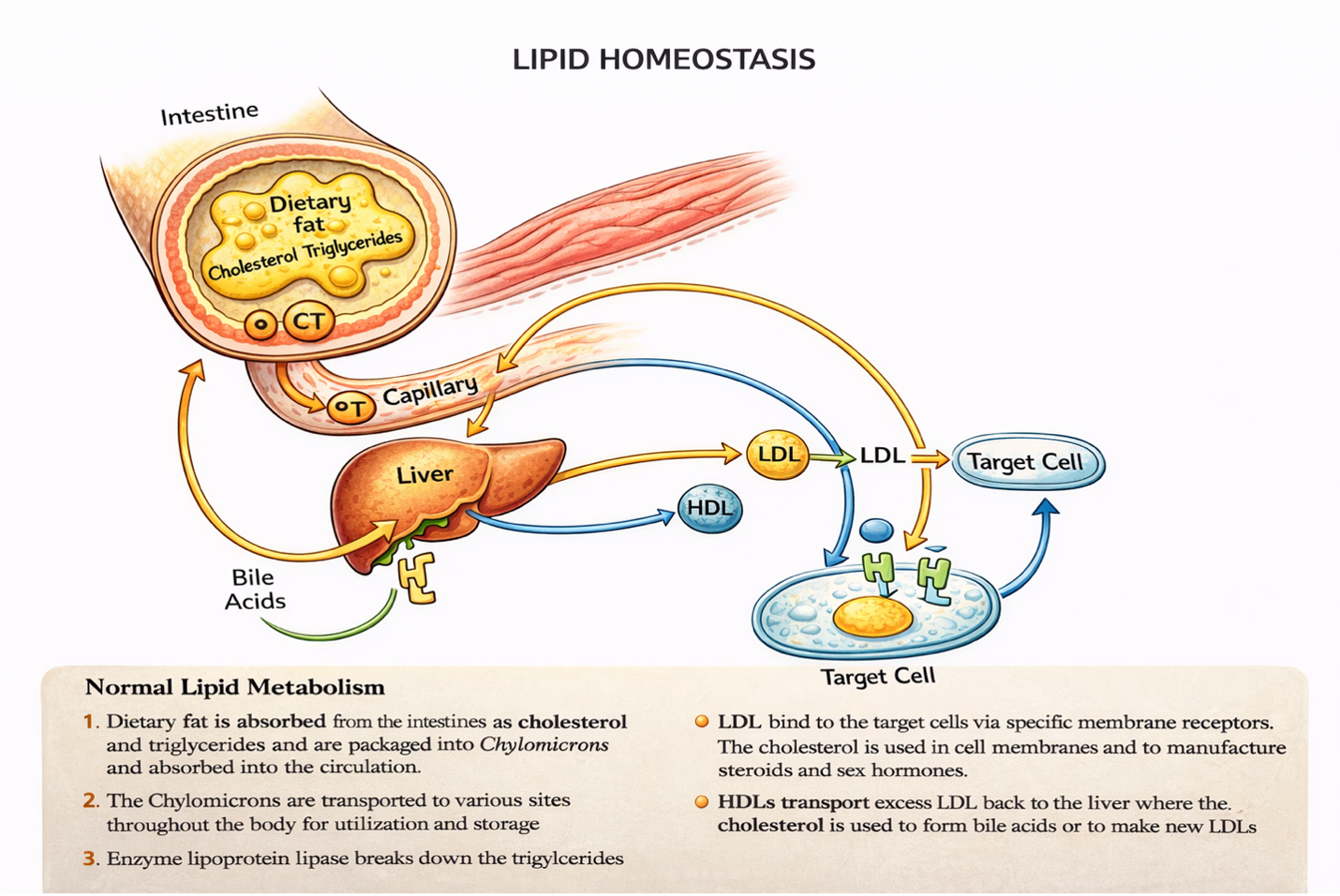
Dyslipidemia is an umbrella term to describe a high level of cholesterol and /or triglycerides or a low level of high-density lipoprotein (HDL). Hyperlipidemia refers to high cholesterol (Davidson & Altenburg, 2025). The two important lipids in the blood are cholesterol and triglycerides.
Triglycerides are a type of fat used for energy. They are produced in the intestine and liver from small fats called fatty acids.
Cholesterol is a fat (also called a lipid) that is an essential component of cell membranes, of brain and nerve cells, and of bile, which helps the body absorb fats and fat-soluble vitamins. It is also used to make vitamin D and many hormones including estrogen, testosterone and cortisol (Davidson & Altenburg, 2025).
Conditions and Disorders Related to Perfusion
Now that we have reviewed the basic anatomical and physiological concepts of the cardiovascular and renal system, let’s discuss some common cardiac disorders.
Cholesterol Facts
Cholesterol is lipophilic, transported through the blood inside lipoproteins. Cholesterol has many important functions:
- Component of cell membranes,
- synthesis of certain hormones,
- synthesis of bile salts used in digestion of dietary fats and to facilitate abs of fat-soluble vitamins,
- reduces water evaporation in skin.
Cholesterol is mostly produced in the liver, & also comes from dietary sources
An increase in dietary cholesterol produces a small increase in blood cholesterol b/c a rise in exogenous cholesterol, inhibits endogenous cholesterol production
Saturated fat intake is important… ↑ saturated fats contribute to an ↑circulating cholesterol b/c the liver uses saturated fats to make cholesterol
Hepatic cholesterol synthesis is catalyzed by 3-hydroxy-3-methylglutaryl coenzyme A reductase (HMG-CaA reductase)
Lipoproteins are round particles that carry fat (lipids) and proteins, and they travel in the bloodstream to cells throughout your body. The different types of lipoproteins are chylomicrons, high-density lipoproteins (HDL), low-density lipoproteins (LDL) and very low density lipoproteins (VLDL).
- High density lipoprotein (HDL) cholesterol: Often called “good” cholesterol because it promotes the excretion of cholesterol. It carries cholesterol from the peripheries back to the liver to be excreted. Exercise helps to increase HDL and remove cholesterol from the bloodstream. ↑HDL = ↓risk of CAD
- Low density lipoprotein (LDL) cholesterol: Often called “bad” cholesterol because it delivers cholesterol to the peripheral tissues, where it can be stored in the bloodstream, which contributes to atherosclerosis. ↑LDL=↑risk of CAD
Lipoproteins or lipids increase for a variety of reasons, and can be due to primary causes such as genetics and secondary causes related to lifestyle and other factors. Lifestyle factors include a diet high in fat, being overweight, and lack of exercise (ADAM, 2018). Low density lipoproteins (LDL) also increase slightly as people age, particularly in women after menopause (Davidson & Altenburg, 2025). Other secondary causes include diabetes mellitus, chronic kidney disease and hypothyroidism.

Pharmacological treatment for managing dyslipidemia for the prevention of cardiovascular disease begins with screening individuals that includes age, health issues, family history, lifestyle factors, and lab work (Canadian Cardiovascular Society, 2021).
Clients over the age of 40 should be automatically screened, that includes a physical exam and lab work for early prevention and to determine risk. This screening should be done every five years after the age of 20. With the client’s lifestyle factors reviewed and any changes implemented to improve their health, and if the lipid profile is still elevated, treatment often begins with the use of a statin medication.
Health behaviour interventions include smoking cessation, healthy eating, managing a healthy weight, exercise, alcohol in moderation and adequate sleep. It is important for the client to adjust lifestyle to minimize their risk factors for CV disease.
Other cholesterol lowering meds will be added, depending on follow up lab work on the response to the statin or if the client’s cholesterol levels dictate the addition of another medication.
To learn more about these interventions go to the 2021 Canadian Society for Managing Dyslipidemia Guidelines, go to the following link: 2021 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in Adults – Canadian Journal of Cardiology
Understanding the lab tests –
Nurses need to understand and interpret typical blood tests for a range of health issues. You do not need to memorize the values as the normal value range will always be provided in the lab reports.
A client is preparing to go for lab work in a few days. Advise the client to not drink alcohol 24 hours before the lab work. Also, do not drink anything except water the morning of the lab work (no food or drink up to 14 hours prior).
HealthLink BC: Cholesterol and Triglyceride Tests
Retrieved from: https://www.healthlinkbc.ca/tests-treatments-medications/medical-tests/cholesterol-and-triglycerides-tests
Ideal cholesterol and triglyceride numbers for adults
| Total cholesterol | Less than 5.2 mmol/L |
| HDL cholesterol | 1.6 mmol/L or higher |
| LDL cholesterol | Less than 2.6 mmol/L (less than 2.0 for people at high risk for an MI) |
| Triglycerides | Less than 1.7 mmol/L |
Atherosclerosis
Arteriosclerosis begins with injury to the endothelium of an artery, which may be caused by irritation from high blood glucose, infection, tobacco use, excessive blood lipids, and other factors. The risk of atherosclerosis increases as the total cholesterol level (LDL, HDL and VLDL) increase, even if the levels are not high enough to be considered dyslipidemia (Davidson & Altenburg, 2025).
Injured artery walls cause inflammation. As inflammation spreads into the artery wall, it weakens and scars it, leaving it stiff. Circulating triglycerides and cholesterol can seep between the damaged lining cells and become trapped within the artery wall, where they are joined by leukocytes, calcium, and cellular debris. Eventually, this buildup, called plaque, can narrow arteries enough to impair blood flow. The term for this condition, atherosclerosis, describes the plaque deposits. Atherosclerosis can affect the arteries that supply the heart and those that supply the brain, potentially leading to a stroke.
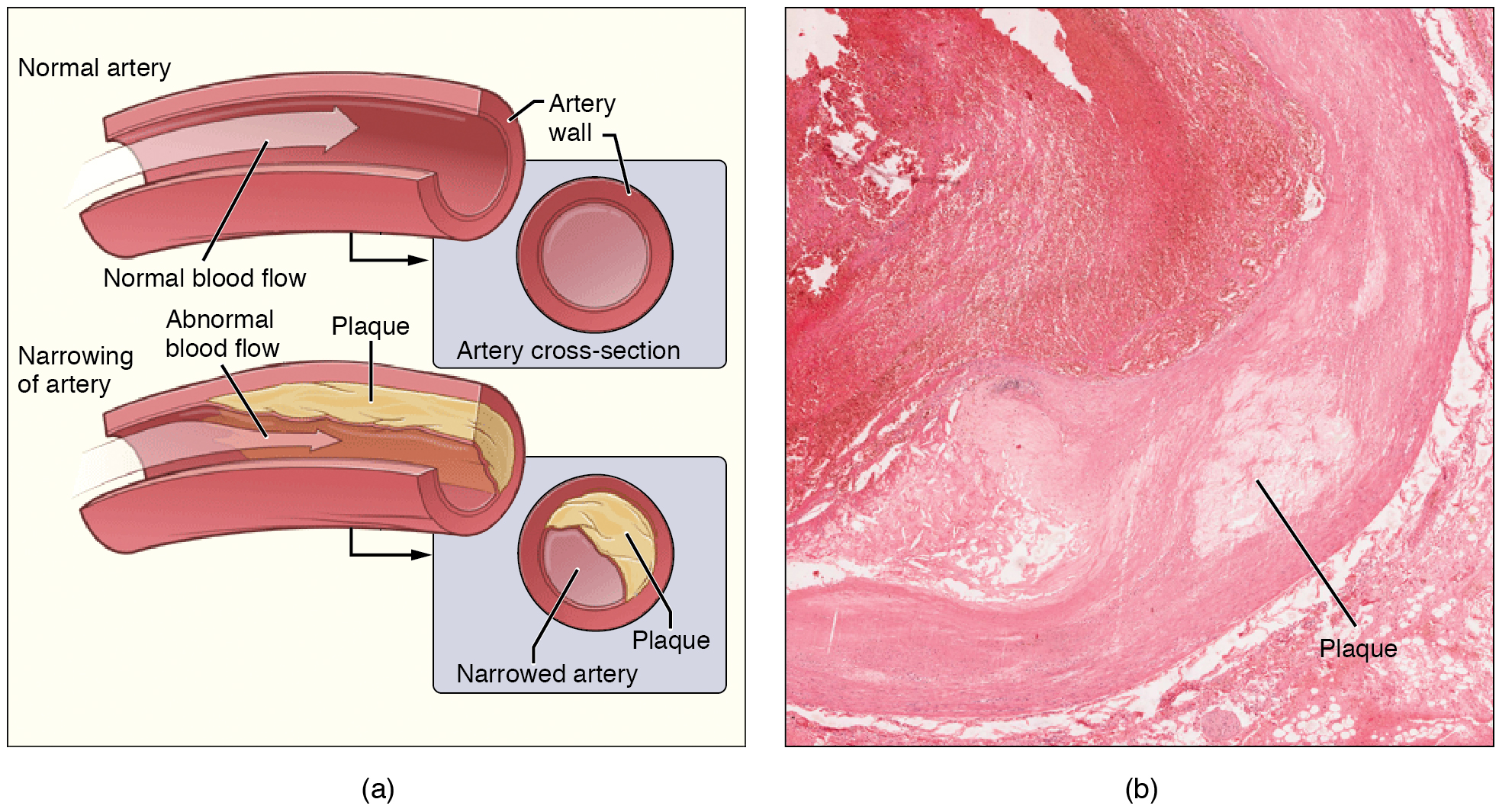
Sometimes plaque can rupture, causing microscopic tears in the artery wall that allow blood to leak into the tissue on the other side. When this happens, platelets rush to the site to clot the blood. This clot can further obstruct the artery and—if it occurs in a coronary or cerebral artery—cause a sudden heart attack or stroke. Alternatively, plaque can also break off and travel through the bloodstream as an embolus until it blocks a more distant, smaller artery.
Even without total blockage, narrowed vessels lead to ischemia (reduced blood flow to the tissue region “downstream” of the narrowed vessel). Ischemia can lead to hypoxia (decreased supply of oxygen to the tissues), causing a myocardial infarction or cerebrovascular accident.
Treatment of atherosclerosis includes lifestyle changes, such as weight loss, smoking cessation, regular exercise, and adoption of a diet low in sodium and saturated fats. Antilipemic drugs such as Atorvastatin are prescribed to reduce cholesterol and help prevent atherosclerosis.
Hypertension
Chronically elevated blood pressure is known clinically as hypertension. Hypertension Canada identity hypertension as blood pressure over 130/85 using an automated cuff. This lower systolic reading from previous recommendations is to initiate earlier screening and lifestyle changes to avoid cardiovascular disease (Goupil et al, 2025). About 6 million Canadians, or 19 % of our population, currently suffer from hypertension, many of who are unaware of their condition. Unfortunately, hypertension is often a silent disorder, meaning no symptoms occur until complications happen, so clients may fail to recognize the seriousness of their condition and fail to follow their treatment plan. The result is often a heart attack or stroke. Hypertension may also lead to an aneurysm (ballooning of a blood vessel caused by a weakening of the wall), peripheral arterial disease (obstruction of vessels in peripheral regions of the body), myocardial infarction, chronic kidney disease, or heart failure.
Unhealthy lifestyle habits play a major role in the development of hypertension and its associated cardiovascular morbidity and mortality (Goupil et al, 2025). All clients with hypertension should be aware of lifestyle changes to lower their risk. Such changes as lowering dietary salt intake, eating more potassium rich foods, regular moderate intensity exercise (150 minutes per week), weight loss if overweight, and lowering alcohol intake if above 2 drinks/day (Hypertension Canada, 2025). Some clients are also at a higher cardiovascular risk and this includes those with established cardiovascular disease (coronary artery disease, heart failure), diabetes mellitus, chronic kidney disease and those over 75 years of age.
The addition of pharmacological therapy should be used in addition to lifestyle changes. For those with BP 130-139 with no cardiovascular disease risk, trialing lifestyle changes first for 3-6 months, and then if BP is still elevated, then initiating medications.

It is critical to obtain an accurate blood pressure that will be used for the development of a treatment plan for hypertension
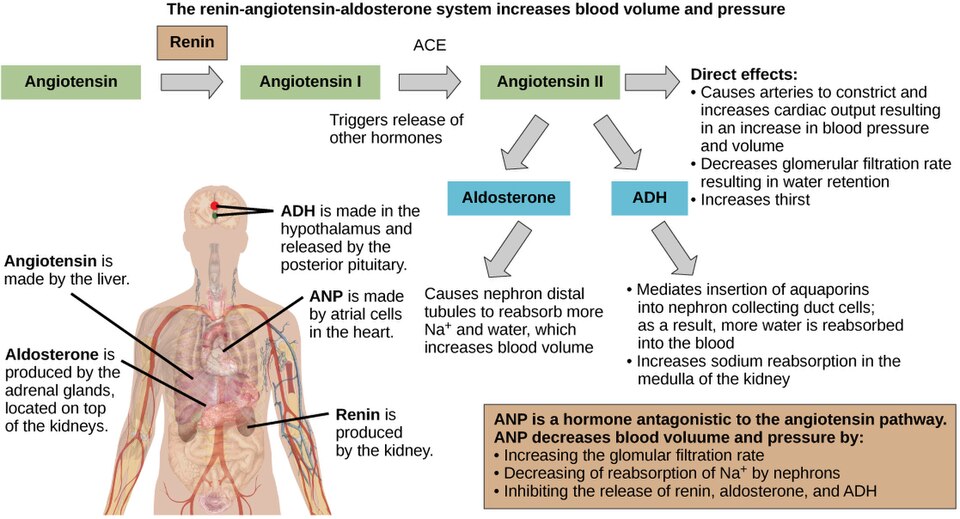
Understanding what causes our blood pressure to increase will help you understand the drugs we use to treat hypertension. Our RAAS system is outlined in the diagram below.
Thrombi and Emboli
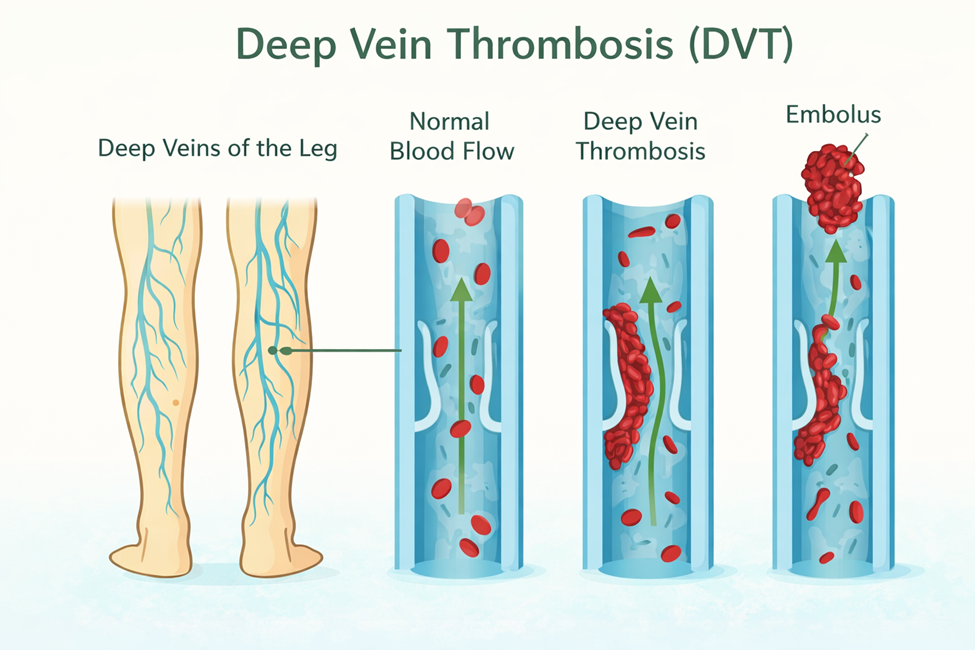
Thrombi are most commonly caused by vessel damage to the endothelial lining, which activates the clotting mechanism. A thrombus can seriously impede blood flow to tissue or organs. Deep vein thrombosis (DVT) can occur when blood in the veins, particularly in the legs, remains stationary for long periods, such as during and after surgery.

When a portion of a thrombus breaks free from the vessel wall and enters the circulation, it is referred to as an embolus. An embolus that is carried through the bloodstream can be large enough to block a vessel critical to a major organ. When it becomes trapped, an embolus is called an embolism. In the heart, brain, or lungs, an embolism may cause a heart attack, a cerebrovascular accident (CVA) – otherwise known as a stroke – or a pulmonary embolism. These are medical emergencies.
Medications such as aspirin and warfarin are used to prevent the formation of clots in people who are at risk. Heparin is a medication that can be used to prevent or treat clots, and tPA is used to dissolve severe clots causing ischemia in the brain, heart, or lungs.
Angina Pectoris
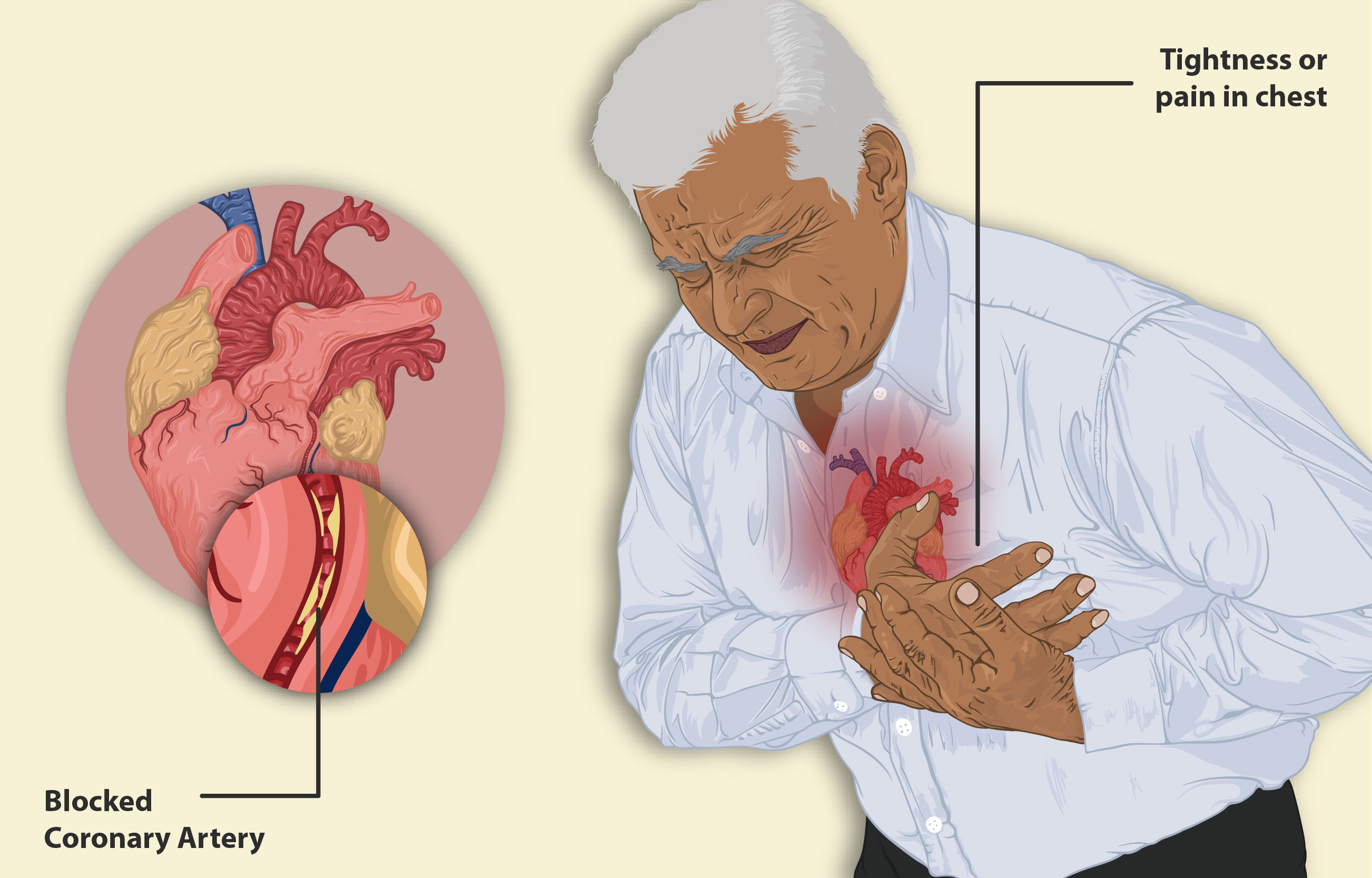
Angina pectoris, or chest pain, is a pressure, squeezing or pain in the center of the chest. It is the most common symptom of ischemic heart disease, a major cause of morbidity and mortality worldwide.
Angina results from an imbalance between myocardial oxygen supply and the myocardial oxygen demand.
Factors that determine myocardial oxygen demand include the contractility of the heart, the heart rate, and the intramyocardial wall tension. Heart contractility and heart rate are influenced by exercise, stress and caffeine, for example, – which all stimulate the SNS leading to increased heart rate and contractility. The myocardial wall tension is determined by preload and afterload. Drugs that reduce these factors, reduce oxygen demand.
The factor that determines oxygen supply is the myocardial blood flow. At rest, the heart extracts nearly all the oxygen that is delivered to the heart by the coronary vessels. When oxygen demand increases, such as during exercise, the coronary arteries dilate and blood flow increases. This increase in blood flow to perfuse the myocardium occurs during diastole (heart is at rest). (Rosenjack Burchum & Rosenthal, 2019). In a healthy heart, this oxygen supply and demand is in balance. A heart with coronary artery disease will not be able to adequately deliver blood to the myocardium, resulting in an imbalance with oxygen needs and anginal pain.
Coronary artery stenosis is the most common cause of myocardial ischemia. During increased myocardial oxygen demand, the stenosis prevents adequate myocardial oxygen supply. So, when there is increased demand without increased oxygen supply, angina results (Gillen & Goyal, 2022).
Angina can be due to non-cardiac and cardiac causes, and thorough history and physical is critical in differentiating these causes and identifying patients experiencing acute coronary syndrome (Gillen & Goyal, 2022). Angina is one of the signs of acute coronary syndrome (ACS). Along with chest pain, clients can experience nausea, shortness of breath and pain that radiates to the jaw, back, and neck.
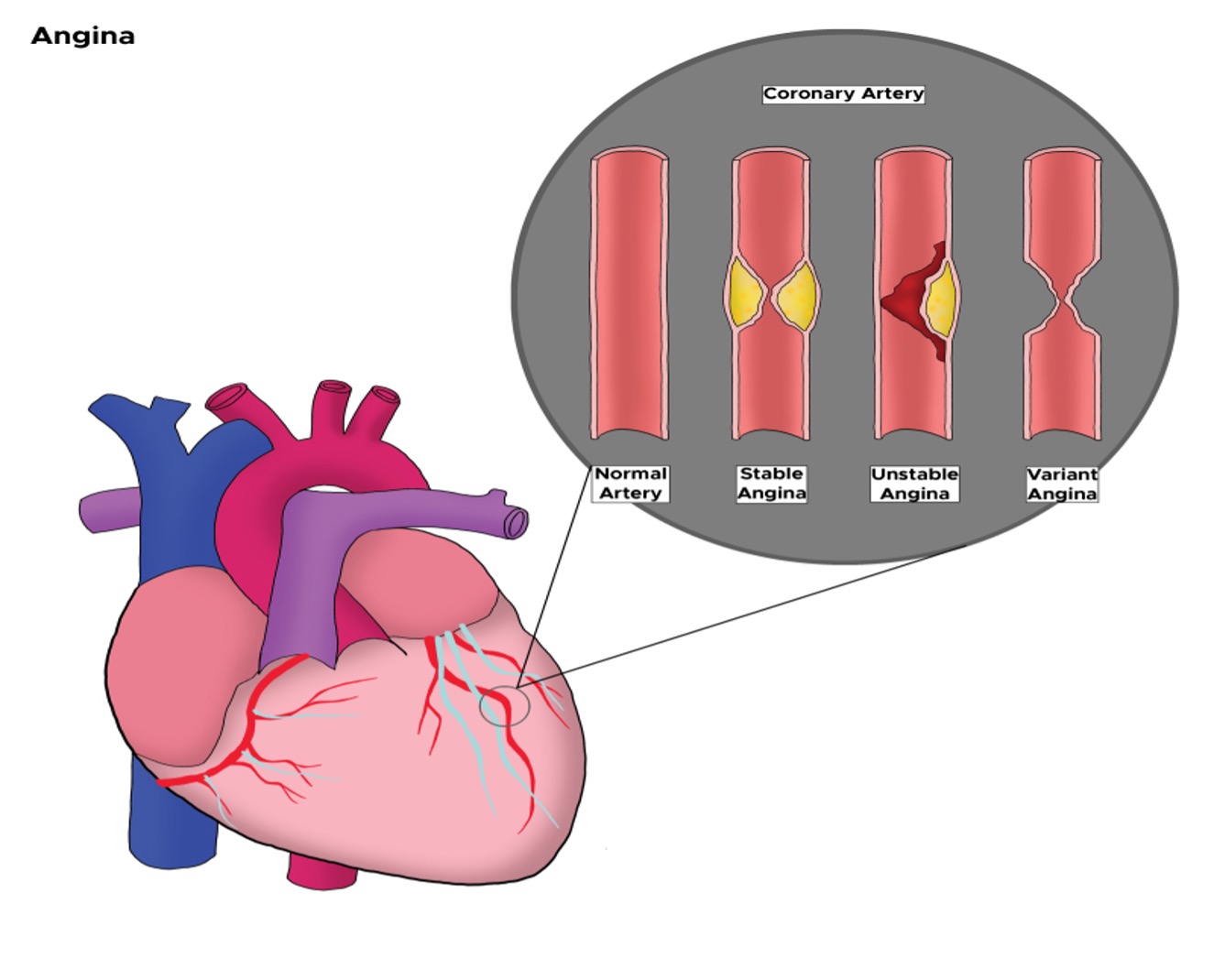
Angina is classified in one of the three categories:
- Stable angina – symptoms occur with exertion only and are due to increased myocardial oxygen demand from increased heart rate, increased blood pressure, and increased myocardial contractility, among other factors.
- Unstable angina – symptoms occur at rest and is the more concerning type of angina. If symptoms don’t resolve, it can lead to myocardial infarction.
- Variant or vasospastic angina, also known as Prinzmetal angina, also occurs at rest but is unrelated to coronary atherosclerosis. It is caused by a spasm in the heart’s arteries that temporarily decreases blood flow. It typically occurs at rest. The spasm can be due to stress, medications, smoking or extreme cold.
Jessica/feb 25: @Copyeditor please advise if the image above can be used.
If left untreated, it can lead to myocardial infarction, stroke, acute coronary syndrome and death. Treatment includes lifestyle changes such as weight loss, quit smoking and to lower cholesterol through diet and medications (i.e. statins). Medications to treat angina include nitrate therapy to improve coronary blood flow and ultimately relief the chest pain and other symptoms. Other medications are prescribed depending on the type and severity of angina, and can include antihypertensives, anticoagulants, antilipemic (HMG-CoA reductase inhibitor), and anti-platelet medications (Tan & Yang, 2024).
Myocardial Infarction
Myocardial infarction (MI) is the medical term for what is commonly referred to as a “heart attack”. It results from a lack of blood flow and oxygen to a region of the heart, due to a partial or full thickness blockage of one or more coronary arteries. Each coronary artery supplies blood to a specific area of the heart’s muscular wall, so if that artery is blocked, that region of the heart will have less oxygen supply and subsequent ischemia. This blockage is often due to a buildup of atherosclerotic plaque and becomes a thrombus or when a portion of an unstable atherosclerotic plaque travels through the coronary arterial system and lodges in one of the smaller vessels. If blood supply is not restored to that area, infarction or myocardial cell death can occur.
Watch the short video on myocardial infarction:
Merck Manual (2025). Video: Myocardial Infarction-Merck Manual Consumer Version
Symptoms of myocardial infarction can vary, with some people experiencing mild symptoms such as nausea and mild chest discomfort. Other clients experience sudden, sharp retrosternal pain, dizziness and diaphoresis. Many of the symptoms are shared with other medical conditions, including anxiety attacks and simple indigestion, so accurate diagnosis is critical for survival. It is important for nurses to ask detailed questions to ensure subtle symptoms are not missed. Symptoms can include:
- Chest pain that may feel like pressure, tightness, pain, squeezing or aching.
- Heart palpitations
- Pain or discomfort that spreads to the shoulder, arm, back, neck, jaw, teeth or sometimes the upper abdomen.
- Diaphoresis
- Fatigue
- Heartburn or indigestion. Pain can be mild or severe substernal pain.
- Light-headedness or sudden dizziness
- Nausea
- Shortness of breath

Jessica/Feb 25: @Copyeditor please review the image above and advise back- DC: Wrote to request permission from https://www.army.mil/article/217669/women_love_your_heart
To diagnose a coronary artery occlusion, in the emergency department, the following examinations will be completed:
- Physical exam: BP, HR, RR and oxygen saturations, along with a physical assessment.
- 12 lead ECG: assess for changes in the ST and Q wave components of the ECG complex. ST-segment elevation in two contiguous lead (measured at J-point) or ST depression and T wave changes (Ojha & Dhamoon, 2023).
- Blood work: troponin, which is a serum cardiac marker that detects chemicals released by the damaged heart muscle.
Types of MI include ST elevation (STEMI) and non-ST elevation (non-STEMI).
- STEMI: this is a complete blockage in a coronary artery resulting in complete lack of blood flow to that area of the heart. The full thickness of the heart muscle can die if blood (oxygen) is not returned right away.
- Non-STEMI: this is a partial blockage of blood flow in a coronary artery. As only part of the heart wall thickness is damaged, the ST segment is often not elevated.
Treatment includes aspirin, nitroglycerine, morphine and possibly supplemental oxygen if oxygen saturations are less than 94% or per agency protocol. Bedrest is also required.
Longer-term treatments depend on the extent of blocked coronary artery (partial or full blockage, one vessel or multiple vessels impacted) and may include: injections of thrombolytic agents, such as the tissue plasminogen activator also known as tPA, that dissolve the clot; the anticoagulant heparin; a balloon angioplasty with stents to open blocked vessels; or bypass surgery to allow blood to pass around the site of blockage. Please note that drugs such as tPA are used in Emergency and Intensive Care Units (Ojha & Dhamoon, 2023).
Cerebrovascular Accident (CVA)
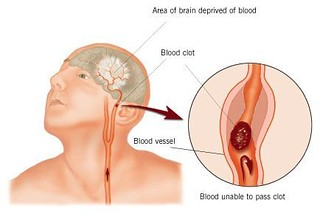
The internal carotid arteries, along with the vertebral arteries, are the two primary suppliers of blood to the human brain. Given the central role and vital importance of the brain to life, it is critical that blood supply to this organ remains uninterrupted. However, blood flow may become obstructed due to atherosclerosis or an embolus that has traveled from elsewhere in the blood. For example, an arrhythmia called atrial fibrillation can cause clots to form in the heart and then move to the brain. When blood flow is interrupted, even for just a few seconds, a transient ischemic attack (TIA), or mini-stroke, may occur, resulting in loss of consciousness or temporary loss of neurological function. Loss of blood flow for longer periods produces irreversible brain damage or a stroke, also called a cerebrovascular accident (CVA) (Open Stax, n.d.). There are two types of cerebrovascular accidents: ischemia and hemorrhagic. Ischemic strokes are caused by atherosclerosis, or a blood clot that blocks the flow of blood to the brain (see Figure 7.2i).
Eighty percent of strokes are ischemic. Hemorrhagic strokes are caused by a blood vessel that ruptures and bleeds into the brain. Risk factors for a stroke include smoking, high blood pressure, and cardiac arrhythmias. Treatment of a stroke depends on the cause (Andersen & Townsend, 2015). Ischemic strokes are treated with thrombolytic medication such as tPA to dissolve the clot, whereas hemorrhagic strokes often require surgery to stop the bleeding.
Arrhythmias
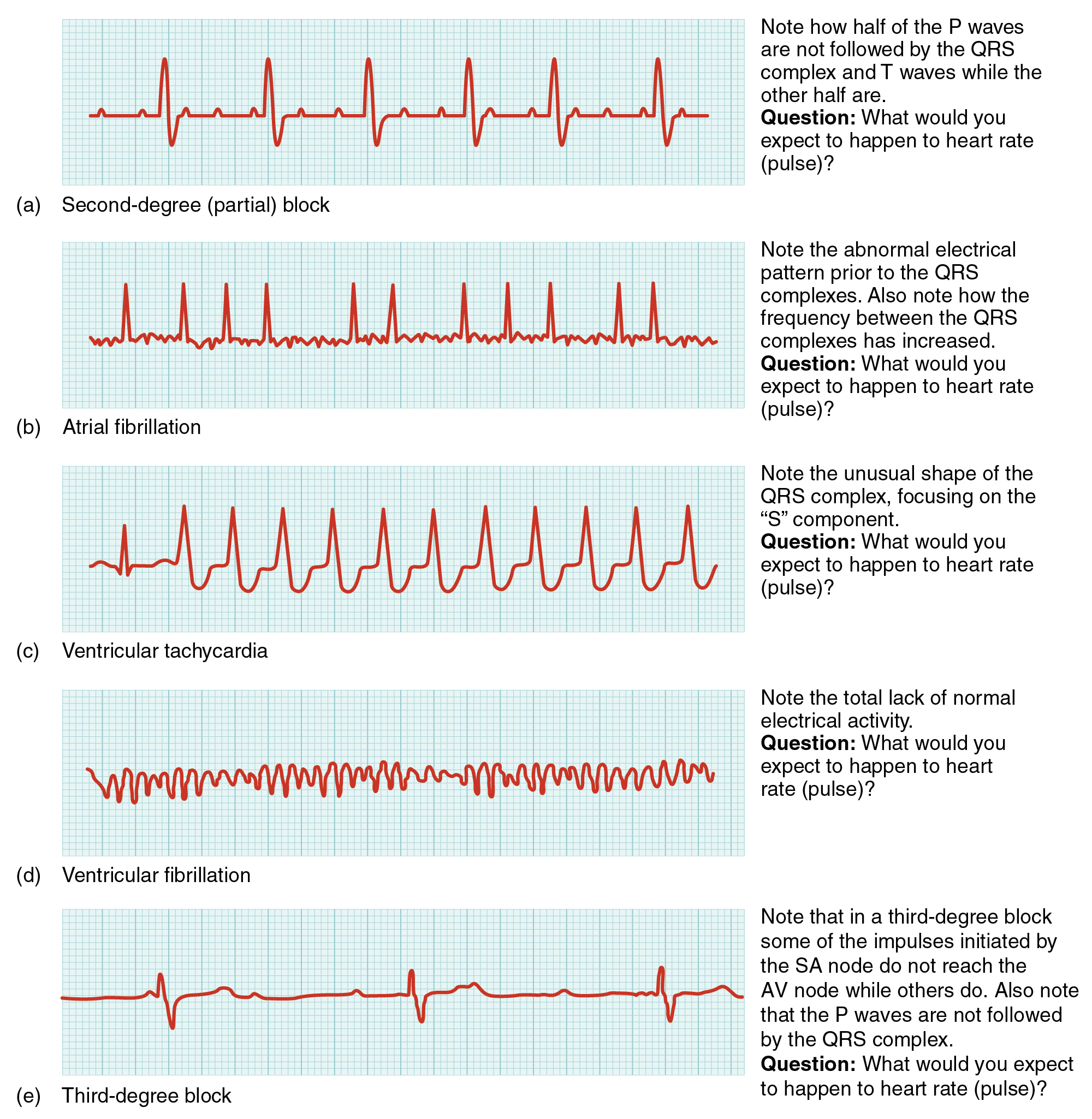
Occasionally, an area of the heart other than the SA node will initiate an impulse that will be followed by a premature contraction. Such an area is known as an ectopic focus. An ectopic focus may be stimulated by localized ischemia, exposure to certain drugs, elevated stimulation by both sympathetic or parasympathetic divisions of the autonomic nervous system, or several diseases or pathological conditions. Occasional occurrences are generally transitory and nonlife threatening, but if the condition becomes chronic, it may lead to either an arrhythmia, a deviation from the normal pattern of impulse conduction and contraction, or to fibrillation, an uncoordinated beating of the heart. Severe arrhythmias can lead to cardiac arrest, which is fatal if not treated within a few minutes.
Abnormalities that may be detected by the ECGs are shown in Figure 7.2j. Antiarrhythmic medications such as Sotalol, Diltiazem, and Amiodarone are used to treat arrhythmias.
Heart Failure
Heart failure (HF) “is a complex clinical syndrome characterized by the heart’s inability to pump blood effectively due to structural or functional impairments.” (Shams, Malik & Chhabra, 2025). In similar terms, it is the inability of the heart to pump enough blood to meet the body’s needs. It is characterized by ventricular dysfunction, reduced cardiac output, insufficient tissue perfusion and signs of fluid retention (Burchum Rosenjack & Rosenthal, 2019).
Heart failure has remained the leading cause of cardiovascular morbidity and mortality in Canada despite advances in treatment. In Canada, more than 100,000 people are diagnosed with HF each year with over 800,000 currently living with heart failure. These numbers are expected to increase due to the aging population and more people surviving from cardiac conditions such as myocardial infarctions (Almufeh et al, 2025).
Heart failure has previously been classified into two types of heart failure. Right sided heart failure or heart failure with left ventricular (LV) systolic dysfunction is when the right ventricle is too weak to pump enough blood to the lungs, leading to a build up in the veins, increased pressure and volume overload. These clients have fluid back up in the rest of the body with symptoms of fatigue, palpitations, enlarged liver, and jugular vein distention. Left sided heart failure or diastolic HF is when the LV ejection fraction is preserved. The left ventricle can’t relax normally because the muscle has become stiff. These clients present with fluid back up in the lungs with symptoms of shortness of breath, cough and fatigue (Informed Health.org, n.d.). Left heart failure is more common.
HF is classified based on left ventricular ejection fraction (LVEF) and clinical staging. Treatment options have evolved and now take into account the broad spectrum of left ventricular ejection fraction from preserved, mildly reduced, reduced or improved LVEF. In this text we will generally discuss standard therapy options for heart failure. According to the Cardiovascular Society of Canada, treatment goals are to prevent further deterioration, treat symptoms and remove the underlying causes if possible (McDonald et al, 2023).
The extent of medications depends on LV dysfunction and clinical presentation. Routine treatment includes three types of drugs:
- Diuretics (thiazide, potassium-sparing, loop)
- Agents that inhibit RAAS (ACE inhibitors, angiotensin II receptor blockers, aldosterone blockers, direct renin inhibitors, angiotensin receptor neprilysin inhibitors)
- Beta blockers (carvedilol, metoprolol)
With more compromised clients with reduced LV dysfunction (EF <40%), quadruple therapy is recommended that includes the following medications:
- ACEi, ARBs or ARNIs
- Beta blockers
- MRAs (mineralocorticoid receptor antagonist)
- Sodium-glucose cotransporter-2 inhibitors (SGLT2i’s)
In addition, depending on symptoms, an individualized plan that includes the addition of diuretics, digoxin and other classes of meds (McDonald et al, 2023).
Overall, the management of heart failure has become increasingly complex. Medication advancements are ongoing. Other non-pharmacological interventions to support symptom management include exercise, sodium and fluid restrictions, limiting alcohol and smoking cessation.
Image Description
The renin-angiotensin-aldosterone system image description: The renin-angiotensin-aldosterone system, illustrated in Figure 7.2e proceeds through several steps to produce angiotensin II, which acts to stabilize blood pressure and volume. Renin (secreted by a part of the juxtaglomerular complex) is produced by the granular cells of the afferent and efferent arterioles. Thus, the kidneys control blood pressure and volume directly. Renin acts on angiotensinogen, which is made in the liver and converts it to angiotensin I. Angiotensin converting enzyme (ACE) converts angiotensin I to angiotensin II. Angiotensin II raises blood pressure by constricting blood vessels. It also triggers the release of the mineralocorticoid aldosterone from the adrenal cortex, which in turn stimulates the renal tubules to reabsorb more sodium. Angiotensin II also triggers the release of anti-diuretic hormone (ADH) from the hypothalamus, leading to water retention in the kidneys. It acts directly on the nephrons and decreases glomerular filtration rate. Medically, blood pressure can be controlled by drugs that inhibit ACE (called ACE inhibitors).
Image description by Open Stax College found on OER Commons is licensed under a CC BY NC license.
Andrea: Jessica – note the inclusion of two images and the subsequent numbering change. The two new images were created by Sheila
Jessica/Feb 26: Done all the image captions have been updated with their correct number/letter
Media Attribution
Jessica/Feb 26: @Copyeditor please review the citations provided below
- 7.2a Lipid metabolism
- 7.2b “máu nhiễm mỡ – cholesterol” by LÊ VĂN THẢO is licensed under CC BY-SA 2.0 ↵
- 7.2c “2113ab Atherosclerosis.jpg” by OpenStax College is licensed under CC BY 4.0. Access for free at https://openstax.org/books/anatomy-and-physiology/pages/20-2-blood-flow-blood-pressure-and-resistance
- 7.2d Monthly check up.” by Bryan Mason is licensed under CC BY 2.0 ↵
- This work is a derivative of “Deep vein thrombosis of the right leg.jpg” by James Heilman, MDis licensed under CC BY-SA 3.0 ↵
- 7.2e Renin-angiotensin-aldosterone system Open Stax College Renin angiotensin found on OER Commons is licensed under a CC BY NC license.
- 7.2f This work is a derivative of “Deep vein thrombosis of the right leg.jpg” by James Heilman, MD is licensed under CC BY-SA 3.0 ↵
- 7.2g Deep vein thrombosis formation
- 7.2h Diagram of the heart showing different forms of angina.
- StatPearls Publishing LLC. (2023). Retrieved from https://openstax.org/books/pharmacology/pages/18-1-hypertension-and-angina
- 7.2i Symptom differences between men and women with myocardial infarction
- Modern Heart and Vascular Cardiac Differences Between Women and Men
- 7.2j “A man having a Heart Attack.png” by https://www.myupchar.com/en is licensed under CC BY-SA 4.0 ↵
- 7.2k “Stroke Diagram” by ConstructionDealMkting is licensed under CC BY 2.0 ↵
- 7.2l “Common ECG Abnormalities” by CNX OpenStax is licensed under CC BY 4.0. Access for free at https://openstax.org/books/anatomy-and-physiology/pages/19-2-cardiac-muscle-and-electrical-activity
References
A.D.A.M. Medical Encyclopedia [Internet]. Atlanta (GA): A.D.A.M., Inc.; c2019. High blood cholesterol levels; [reviewed 2018 February 22; updated 2018 March 28; cited 2019 November 29]. https://medlineplus.gov/ency/article/000403.htm. ↵
Anderson, P. & Townsend, T. (2015) Preventing high-alert medication errors in hospital patients. Nurse Today, 10(5). https://www.americannursetoday.com/wp-content/uploads/2015/05/ant5-CE-421.pdf ↵
Brunham, L., Lonn, E. & Mehta, S. (2022). Dyslipidemia and the Current State of Cardiovascular Disease: Epidemiology, Risk Factors, and Effect of Lipid Lowering. Canadian Journal of Cardiology, 40(8), S4-S12. https://onlinecjc.ca/article/S0828-282X(24)00338-6/fulltext
Canadian Cardiovascular Society (2021). Canadian Cardiovascular Society Dyslipidemia Guidelines. 90364 CCS – Dyslipidemia 2022 rev5
Davidson, M. & Altenburg, M. (2025). Dyslipidemia. Merck Manual. Dyslipidemia – Hormonal and Metabolic Disorders – Merck Manual Consumer Version
Gillen, C. & Goyal, A. (2022). Stable angina. National Library of Medicine. StatPearls [internet]. Stable Angina – StatPearls – NCBI Bookshelf
Goupil, R., Tsuyuki, R., Santesso, N., Terenzi, K., Habert, J., et al (2025, May 26). Hypertension Canada guideline for diagnosis and treatment of adults in primary care. Canadian Medical Association Journal, 197, E549-64. doi: 10.1503/cmaj.24177 Hypertension Canada guideline for the diagnosis and treatment of hypertension in adults in primary care
Government of Canada, (2025). High Blood Pressure. https://www.acc.org/latest-in-cardiology/ten-points-to-remember/2017/11/09/11/41/2017-guideline-for-high-blood-pressure-in-adults. ↵
Government of Canada. (2022). Surveillance of heart diseases and conditions. Public Health Agency of Canada. Surveillance of heart diseases and conditions – Canada.ca
Hussain, K., Mandras, S., Desai, S. (2024). Right Heart Failure. National Library of Medicine. Right Heart Failure – StatPearls – NCBI Bookshelf
Hypertension Canada (2025). Primary care guidelines: treatment. Treatment – Hypertension Canada | For Healthcare Professionals
Informed Health.org (2023). Heart Failure: learn more-types of heart failure. Heart failure: Learn More – Types of heart failure – InformedHealth.org – NCBI Bookshelf
McDonald, B., Virani, S., Zieroth, S., & Turgeon, R. (2023). Heart failure management in 2023: a pharmacotherapy and lifestyle focused comparison of current international guidelines. Canadian Cardiovascular Society, 5(8), 629-640.
National Heart, Lung, and Blood, National Institute of Health (2019). Heart failure. https://www.nhlbi.nih.gov/health-topics/heart-failure ↵
Ojha, N. & Dhamoon, A. (2023). Myocardial Infarction. National Library of Medicine.https://www.ncbi.nlm.nih.gov/books/NBK537076/
OpenStax College (n.d.). Cerebral vascular accident. OER Commons is licensed under a CC BY NC license. StatPearls Publishing LLC. (2023). Retrieved from https://openstax.org/books/pharmacology/pages/18-1-hypertension-and-angina
Pearson, G. et al (2021). Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in Adults. Canadian journal of Cardiology 37, 1129-1150.
Rosenjack Burchum, J., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
Tan, W. & Yang, E. (2024). Unstable angina. Medscape. Unstable Angina: Practice Essentials, Background, Pathophysiology
When a portion of a thrombus breaks free from the vessel wall and enters the circulation. An embolus that is carried through the bloodstream can be large enough to block a vessel critical to a major organ. When it becomes trapped, an embolus is called an embolism. In the heart, brain, or lungs, an embolism may accordingly cause a heart attack, a stroke, or a pulmonary embolism.
Occurs when blood flow is interrupted to the brain, even for just a few seconds, resulting in loss of consciousness or temporary loss of neurological function.
Lack of blood flow to the brain that can cause irreversible brain damage, often referred to as a “stroke”.
A deviation from the normal pattern of impulse conduction and contraction of the heart, which if serious and untreated, can lead to decreased cardiac output and death.
An uncoordinated beating of the heart, which if serious and untreated, can lead to decreased cardiac output and death.

{kind=link}
{kind=link}
{kind=link}
{kind=link}