6.8 Anesthetics V2
Learning Outcomes
- Describe the purpose of local and general anesthetic agents.
- Understand the mechanism of action, indications for use, adverse effects and nursing considerations for local anesthetics.
- Understand the indications for use and nursing considerations for general anesthetics.
- Understand the mechanism of action, indications for use, adverse effects and nursing considerations for NDMA agents: Ketamine.
For many clients, the treatment of pain is often managed with taking a non-steroidal anti-inflammatory and depending on the severity, they may also be treated with an opioid medication. Opioids provide excellent pain relief but have significant side effects such as sedation, nausea, constipation and the risk of tolerance. Adjunct pain medications are often used for chronic pain, including neuropathic pain syndromes but have some limitations with the degree of pain relief provided. Local anesthetic agents provide an option for pain relief for situations that more localized relief is needed, which can be for both acute and chronic pain.
Anesthetic agents are categorized into local and general anesthesia. For very localized pain situations, such as dental work or a painful joint, local anesthetics provide total or partial loss of sensation targeting just the painful site. General anesthetics produce a general loss of consciousness and sensation and is used for most surgical procedures that require the client to be without pain and be unconscious for a long period of time.
As a nurse, you may care for a client prior to preoperative, perioperative, or postoperative. It is important that you are aware of the type of anesthetic that your client has received or been prescribed, which will direct your assessment, monitoring for adverse side effects and other interventions.
In this unit, we will focus mostly on local anesthetic agents and ketamine with an emphasis on nursing considerations.
Local Anesthesia
Local anesthetics produce a rapid loss of sensation to a localized part of the body. These agents produce a total or partial loss of sensation, particularly tactile sensation and pain (Drugbank, 2025).
Indications for Use:
Local anesthetics are used for many different purposes. Most are effective for short term pain relief such as for procedures or acute pain situations. For some clients with chronic myofascial pain syndromes, local anesthetics can be injected to a number of tissues, including nerve, joint and muscle. For example, post-herpetic pain or fibromyalgia (Bagshaw et al, 2015).
There are different routes of local anesthesia which are outlined in the table 6.8a. The route selected depends on the purpose of anesthesia. For example, epidural injection for labour, direct injection into tissue for dental work, or topical application for painful hemorrhoids (Bagshaw et al, 2015; Adams et al, 2019).
Types of local anesthetics:
There are two types of local anesthetics: ester-type such as procaine and amide-type agents such as lidocaine. Ester and amide refer to their chemical structure. Typically, amides have replaced ester anesthetics due to less side effect and longer duration of action.
Ester: procaine, cocaine
Amide: bupivacaine, lidocaine, ropivacaine
The physician chooses the type of agent and the route based on client specific factors such as allergies and the purpose of the procedure (acute vs chronic pain) and the extent of loss of sensation required. Lidocaine has moderate potency and duration of action. Bupivacaine has high potency and duration of action. Both agents also come in different concentrations, such as lidocaine 1% or 2% or bupivacaine 0.25 or 0.50%. This will increase potency but also increase systemic effects (Bagshaw et al, 2015).

Figure 6.8a Vial of lidocaine 1% for local anesthesia
Lidocaine hci.jpg https://commons.wikimedia.org/wiki/File:Lidocaine_hci.jpg
Mechanism of Action
The mode of action is the same for all commonly used local anesthetics. Local anesthetics reversibly block conduction of neural impulses along nerve fibers by binding to sodium channels in the nerve. When the nerve cannot uptake sodium it cannot transmit an impulse.
Adverse/Side Effects
For each route, there are benefits and risks. Refer to the chart for a brief overview of each anesthetic route.
| Route | Example in practice | Additional comments |
| Topical
|
Applied to mucous membranes, eyes, throat. Lidocaine is widely used.
· ointment for painful hemorrhoids · patch or ointment for sore muscles, · applied to skin before painful procedure (IV insertion for peds).
|
Very little systemic effects if applied in small amounts. Risk of toxicity if large amount applied or to broken skin.
Low skin penetration |
| Infiltration | Injected directed into tissue to block specific group of nerves at the surgical site. Lidocaine or bupivacaine. Epinephrine can be added to prolong effect. | |
| Nerve block | Injected near or distant to surgical field/target site. Lidocaine or bupivacaine.
· Blocks sensation to limb for 12-24 hours. |
Benefit of early ambulation but risk with infection, nerve injury or hematoma. |
| Spinal (subarachnoid) | Injected into cerebral spinal fluid (CSF) at lumbar region. | Autonomic blockade can cause urinary or fecal incontinence.
Spinal headache (posture dependent). |
| Epidural | Injected into epidural space within spinal column but outside dura mater. Blocks conduction of nerve roots in that area. Lidocaine or bupivacaine. Continuous infusion or one time dose.
· During delivery · Painful bowel surgeries
|
Adams et al, 2019; Drugbank, 2025; Professional Practice Network of Ontario, 2021, March; Urban, & Bleckwenn, 2002.
Local Anesthetic Toxicity
For all routes there is a risk of the anesthetic entering the bloodstream. Epidural injections have a higher risk of puncture due to the location near thin-walled arteries/veins, compared to a nerve block which is injected near thick-walled veins. Topical application can pose a risk if ointment is applied to broken skin.
Client presentation includes:
- CNS: dizziness, drowsiness, disorientation, tinnitus, twitching, apneic, LOC
- CVS: arrythmias (prolonged PR interval, bundle branch blocks, ectopy), hypotension, cardiac collapse
- GI: nausea, vomiting, diarrhea
Monitoring includes BP, HR, RR and oxygen saturations, and level of consciousness.
Hypersensitivity:
pruritic rash may develop at site within 72 hours. Actual allergic reaction is rare.
Respiratory symptoms:
Diaphragm paralysis. Due to phrenic nerve is blocked (C3, C4, C5). Assess for decreased breath sounds potentially only on one side, elevated hemidiaphragm on chest X-ray.
Pneumothorax – if supraclavicular nerve block, risk of pneumothorax.
Hematoma formation:
Inadvertent puncture of nearby vascular structures can lead to perineural hematoma with regional nerve block. Apply pressure to the site to stop the bleeding and hematoma..
Neonatal Depression:
for epidurals during labour and delivery, there is a risk of neonatal bradycardia and CNS depression. Monitor cardiac and respiratory status.
Nursing Considerations
Depending on the route of delivery, the nurse’s role will be to prepare the client for the procedure, and provide monitoring afterwards. For each route of administration, different assessments and monitoring are required. Below are nursing considerations for a few of the routes.
Topical application: this includes any ointments, patches, creams.
- Assess: pain assessment, assess area for broken skin or infection.
- Wear gloves for application
- Avoid broken skin
- Apply smallest amount needed and only to the affected area
- Avoid wrapping the site or applying heat, unless directed, as this will accelerate absorption.
- Adverse effects: Very little systemic effects if applied in small amounts. Risk of toxicity if large amount applied.
Epidural: For clients with an epidural catheter for pain management post-operatively or during delivery, refer to the hospital policy and procedures. Close assessment and monitoring are important to avoid risk of respiratory depression or cardiovascular effects (hypotension, bradycardia).
The Epidural solution is often ordered as a combination of an opioid and anesthetic agent in normal saline. The bag is specially prepared in the pharmacy and is labelled for epidural infusion. It is always preservative free.
For example: Bupivacaine 0.25% with Fentanyl 2 mcq/mL in 0.9% sodium chloride 100 mL.
Post-insertion and after client is stable, monitor client q 4 hours and PRN.
- Sedation score
- Pain score
- Motor block (Bromage scale): flex ankles and knees. Potential for motor nerves affected. Score can be 0 block, 1 (just able to move knees), 2(able to move feet only), 3 (unable to move feet or knees). Can be unilateral or both sides.
- Sensory block (Dermatome level): ice test to determine the upper and lower levels of dermatome involvement. Numbness should only be within a few dermatomes above and below the site of insertion.
- Vital signs: blood pressure, heart rate, resp rate and oxygen saturations.
Adams et al, 2019; Professional Practice Network of Ontario (2021, March).
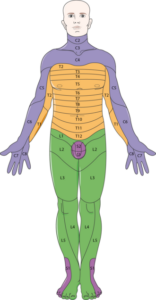
Figure 6.8b File:Nervous system – Dermatomes 1 — Smart-Servier.png This file is licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license.
https://commons.wikimedia.org/wiki/File:Nervous_system_-_Dermatomes_1_–_Smart-Servier.png
General Anesthesia
General anesthesia is a medication-induced reversible unconsciousness with loss of protective reflexes. All sensation including loss of consciousness is lost. In comparison to local anesthetics, the loss of sensation is throughout the whole body.
General anesthesia is usually accomplished with more than one drug to achieve a balanced anesthesia with rapid induction of unconsciousness, muscle relaxation and to maintain a deep anesthesia (Adams et al, 2019). Due to the generalized effect, general anesthesia requires the establishment and maintenance of airway control (Frandsen & Pennington, 2018).
General anesthetics are administered by the anesthesiologist prior and during surgery either intravenously or by inhalation. In the post-anesthetic recovery room, nurses will closely monitor the client for CNS depression, respirations and oxygen saturations, and any vital sign changes, along with assessing for nausea and vomiting and any post-op bleeding (Adams et al, 2019).
Alternative to Anesthetics for Painful Procedures: Conscious Sedation
For some clients, a short duration procedure is required, such as resetting a dislocated shoulder or for a scheduled colonoscopy. In these cases, physicians will do a conscious sedation. Conscious sedation is an approach that provides sedation, dissociation and analgesia for non-invasive or minimally invasive procedures outside the operating room A combination of medications are injected through a intravenous that allows the client to be relaxed (benzodiazepine: midazolam) and free of pain (opioid: fentanyl) during the medical procedure. This allows the client to remain awake and aware, without feeling discomfort (Frandsen & Pennington, 2018). The client may or may not be able to speak or respond in this state and will be drowsy. Midazolam is a short acting benzodiazepine. Fentanyl has a rapid onset of action, within a minute, and also a short duration action. Both meds work well together for short procedures. Sometimes, propofol is given in place of midazolam. Ketamine can also be used, in particular for children. Nurses assist in the procedure with completing the pre-procedural vital signs, ongoing assessment and airway monitoring during the procedure and then post-procedure monitoring for airway management, cardiovascular status and pain.
There are a number of other drugs used for anesthetic purposes that is beyond the scope of this textbook. In specialized areas such as the operating room and critical care areas, nurses will receive additional training to assess and monitor clients receiving those medications.
NMDA antagonists: Ketamine
Ketamine provides sedation, amnesia, and analgesia with a lower risk of respiratory depression. It is used effectively for anesthesia induction, procedural sedation, pain management and psychiatry. It produces a dissociative anesthesia where the person feels dissociated from their environment (Rosenbach Burchum & Rosenthal, 2019).
Indications for use:
Ketamine is used for anesthesia either on its own or in combination with other medications. It is also highly effective for brief surgical procedures that does not require skeletal muscle relaxation. For example, for emergencies that require short-term procedural sedation and rapid sequence intubation (Rosenbaum et al, 2024).
It is also used for pain management in the hospital following surgery, in particular for clients with opiate use disorder when the plan is to use opiates sparingly but with there is a need for strong analgesics. Other off label uses are fortreatment-resistant depression, managing suicidal ideation, and treating refractory status epilepticus (Rosenbaum, Gupta, Patel & Palacios, 2024).
Dosing:
Ketamine can be given IV or IM, dosing depends on the use(Benzoni, Agarwal & Cascella, 2025).
Procedural sedation and anesthesia induction:
IV: initial dose of 1-2 mg/kg with additional doses of 0.5 -1.0 mg/kg q 5-10 minutes. IV onset of action is less than 30 seconds, with duration of action 5-10 minutes
IM: dosing is 5 mg/kg with duration of action 10-25 minutes.
Low-dose ketamine infusion:
For clients with chronic pain issues that have become opiate dependent or where the risk factors using opiates are best avoided (Ead, 2022). Low-dose ketamine infusion or intermittent prn administration is used either alone or along with other adjunct pain-relieving medications. The dosing is much lower than for anesthetic purposes. For example, 10 mg IV given over 30 minutes (compared to anesthetic doses of 1-2 mg/kg). This low dose avoids many of the adverse effects, but may cause brief elevated blood pressure and transient tachycardia (Ead, 2022).
Mechanism of action
Ketamine is a noncompetitive N-methyl-D-aspartate (NMDA) and glutamate receptor antagonist that blocks HCN1 receptors. It also inhibits glutamate, an excitatory neurotransmitter involved in pain transmission. Further, cholinergic, aminergic, and opioid systems appear to play both a positive and negative modulatory role in both the sedative and analgesic effects (Rosenbaum et al, 2024). It desensitizes central pain pathways and modulates opioid receptors.
Adverse effects
CNS: during the recovery period following ketamine, some clients will experience vivid dreams and delirium, even hallucinations. These are usually short lived but can last 24 hours. To minimize these effects, co-administer a benzodiazepine, such as midazolam or lorazepam.
CVS: May increase heart rate and blood pressure due to sympathetic stimulation.
GI: can cause nausea and vomiting. Pretreat with ondansetron.
Nursing Considerations
Ketamine is contraindicated with clients with poorly controlled hypertensions or elevated intracranial pressure. It is not recommended for pregnant clients.
Following ketamine administration for procedural sedation, it is important to monitor cardiovascular and respiratory status. Anticipate the client may experience a dissociative state with short term delirium or confusion.
For intermittent ketamine for pain management: monitor BP and HR. anticipate hypertension and possible transient tachycardia. Other adverse effects include nausea, increased salivation, blurred vison and dizziness (Ead, 2022).
Ketamine with propofol:
For emergency or procedural sedation, ketamine can be administered with propofol. This combination mitigates some of the adverse effects of each med. Propofol reduces ketamine induced vomiting. Ketamine reduces the hypotensive effects of propofol.
References
Adams, M., Urban, C., El-Hussein, M., Osuji, J. & King, S. (2018). Pharmacology for Nurses. A pathophysiological approach (2ndCanadian ed.). Pearson Canada Inc: Ontario.
American Society of Anesthesiologists. (2021). Regional anesthesia. https://www.asahq.org/madeforthismoment/anesthesia-101/types-of-anesthesia/regional-anesthesia/
Bagshaw, K., Hanenbaum, C., Carbone, E., Lo, K., Laurencin, C., Walker, J. & Nair, L. (2015). Pain management via local anesthetics and responsive hydrogels. Therapeutic Delivery, 6(2), 165-176. doi: 10.4155/tde.14.95
Benzoni, T., Agarwal, A., Cascella, M. (2025). Procedural Sedation. National Library of Medicine. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK551685/
Drugbank (2025). Anesthetics. https://go.drugbank.com/drugs/DB00297
Ead, H. (2022). Low-dose Ketamine: overcoming stigmas to optimize pain management
Frandsen, G., & Pennington, S. (2018). Abrams’ clinical drug: Rationales for nursing practice (11th ed.). pg. 305, 310, 952-953, 959-960. Wolters Kluwer. ↵
Professional Practice Network of Ontario (2021, March). Nursing Management of Patients Receiving Regional Nerve Blocks. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.ppno.ca/wp-content/uploads/2022/02/Self-Directed-Learning-Package-Nursing-Management-of-Patients-Receiving-Regional-Nerve-Blocks.pdf
Rosenjack Burchum, J., & Rosenthal, L. (2023).Lehne’s pharmacology for nursing care (10th ed.). Elsevier: Canada
Rosenbaum, s., Gupta, l., Patel, P., Palacios, L. (2024). Ketamine. National Library of Medicine. StatPearls. Ketamine – StatPearls – NCBI Bookshelf
The Royal Children’s Hospital Melbourne (n.d.). Nursing guidelines : Epidural Analgesia Nursing Management
Urban, Bernd W. & Bleckwenn, Markus. (2002). Concepts and correlations relevant to general anaesthesia. British Journal of Anaesthesia. 89(3-16). 10.1093/bja/aef164.
Images
Figure 6.8a Vial of lidocaine 1% for local anesthesia Lidocaine hci.jpg https://commons.wikimedia.org/wiki/File:Lidocaine_hci.jpg
Figure 6.8b File:Nervous system – Dermatomes 1 — Smart-Servier.png. Creative Commons Attribution-Share Alike 3.0 Unported license. https://commons.wikimedia.org/wiki/File:Nervous_system_-_Dermatomes_1_–_Smart-Servier.png

{kind=link}