3.11 Medication Safety in Transitions of Care V2
A third area of the World Health Organization’s (WHO, 2019a) Medications Without Harm initiative relates to medication safety during transitions of care. View the interactive activity below to see how medications are reconciled during transitions of care from admission to discharge in a hospital setting.
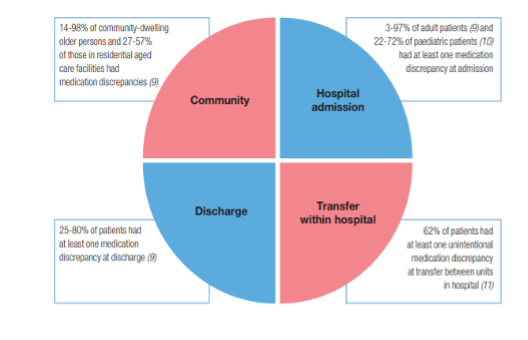
Medication errors can occur during these changes in settings. Figure 3.11a is from the WHO and shows ranges of the percentage of errors that occur during common transitions of care (WHO, 2019b).
Some suggested strategies for improving medication safety include:
- Implementing formal structured processes for medication reconciliation at all transition points of care. Steps of effective medication reconciliation include: building the best possible medication history by interviewing the client and verifying with at least one reliable information source; reconciling and updating the medication list; and communicating with the client and future healthcare providers about changes in their medications.
- Partner with clients, families, caregivers, and healthcare professionals to agree on treatment plans, ensuring clients are equipped to manage their medications safely and have an up-to-date medication list.
- Where necessary, prioritize clients at high risk of medication-related harm and provide enhanced support, such as post-discharge contact by a nurse. (WHO, 2019)
Medication Reconciliation Process
Medication reconciliation is a formal process for creating the most complete and accurate list possible of a patient’s current medications and comparing the list to those in the patient record or medication orders (Institute for Safe Medication Practices Canada [ISMP Canada], 2012). It is a systematic process to obtain a comprehensive list of medications to avoid medication errors due to omissions, duplications, dosing errors, or drug interactions.
All healthcare facilities across Canada have adopted a medication reconciliation process. This is in response to the frequency of medication errors across all healthcare settings. Nurses are very often the healthcare provider completing the ‘Best Possible Medication History’ (BPMP), which is the first step in the medication reconciliation process. Refer to the policy and procedure on the MedRec process in your own facility.
Completing MedRec in primary care involves four main activities:
- Collect and document an accurate and up-to-date medication list (the BPMH)
- Compare the BPMH with information in the patient’s medical records and identify any discrepancies (i.e., differences between various sources of medication information)
- Correct the discrepancies as appropriate through discussion with the primary care provider and the patient; then, update the BPMH with the resolved discrepancies, thereby creating a reconciled list.
- Communicate the resulting medication changes to the patient and verify the patient’s understanding of their medication regimen. (ISMP Canada, 2012)
Medication Reconciliation
Who completes a med rec? Any practitioners, nurses, pharmacists, and allied health professionals, along with the client, families, and other care providers.
What medications are included? All prescription medications, herbals, vitamins, nutritional supplements, over-the-counter drugs, vaccines, diagnostic and contrast agents, radioactive medications, parenteral nutrition, blood derivatives, and intravenous solutions (hereafter referred to collectively as medications)
When is it completed? It is completed at the onset of care and with every transition of care, such as a change in setting, practitioner, or service. For example, a client has been in a long-term care facility and is transferred to an acute care hospital for ongoing care, and then eventually transferred back to long-term care. A MedRec would be done for each transition.
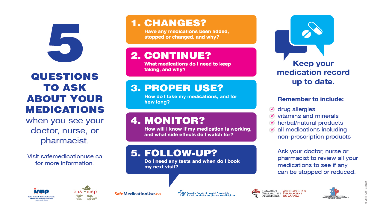
The client, family, or caregiver should be actively involved with the medication reconciliation process. The following brochure (Figure 3.11b) provides clients and families some direction of the types of questions they can ask or expect to be asked when seeing their health care provider.
Andrea: Retrieved from https://www.ismp-canada.org/medrec/
Permission needed
Clinical Reasoning and Decision Making
A nurse is performing medication reconciliation for an elderly client admitted from home. The client does not have a medication list and cannot report the names, dosages, and frequencies of the medication they take at home.
What other sources can the nurse use to obtain medication information?
Note: Answers to the Clinical Reasoning activities can be found in the “Answer Key” sections at the end of the book.
References
Institute for Safe Medication Practices Canada. (2012). Primary care MedRec guide. https://www.ismp-canada.org/primarycaremedrecguide/overviewMedRec.htm
World Health Organization. (2019a). Medication safety in key action areas. Internet Archive. https://web.archive.org/web/20220130041159/http://www.who.int/patientsafety/medication-safety/technical-reports/en/
World Health Organization. (2019b). Medication safety in transitions of care. https://www.who.int/publications/i/item/WHO-UHC-SDS-2019.9
Media Attributions
- Figure 3.11a Figure 5. Medication discrepancies at various transitions of care and frequency of medication-related harm from Medication Safety in Transitions of Care by the World Health Organization is used under a CC BY-NC-SA 3.0 IGO license.
- Figure 3.11b
Long Descriptions
Figure 3.11a Long Description: This is is a circle divided into 4 quadrants to depict 4 areas where medication discrepancy can occur:
- Community: 14–98% of community-dwelling older persons and 27–57% of those in residential aged care facilities had medication discrepancies.
- Hospital admission: 3–97% of adult patients and 22–72% of paediatric patients had at least one medication discrepancy at admission.
- Discharge: 25–80% of patients had at least one medication discrepancy at discharge.
- Transfer within hospital: 62% of patients had at least one unintentional medication discrepancy at transfer between units in hospital.
