3.10 Medication Safety Across Lifespans — Older Adults V2
Anyone working in healthcare has experienced the influx of clients in the aging population, many who have at least one chronic health challenge and often have lifelong medications to manage chronic or acute health conditions. In 2016, one-quarter of Canadian seniors were prescribed 10 or more medications (Farrell et al., 2023). Furthermore, the prevalence of potentially inappropriate medications and polypharmacy has increased over the last 20 years, along with an increased risk of adverse drug events, drug-drug interactions, hospital admission, and mortality. Contributing to the risk of adverse effects is the pharmacokinetic and pharmacodynamic changes occurring in older adults.
Polypharmacy in Older Adults
Polypharmacy is the concurrent use of multiple medications. Although there is no standard definition, polypharmacy is often defined as the routine use of five or more medications. This includes over-the-counter, prescription, traditional, and/or complementary medicines used by a client. As the population ages, more people are likely to suffer from multiple long-term disorders or diseases and take multiple medications. The average intake of medications in an older adult is two to five prescription medications on a regular basis, and polypharmacy occurs in 20–50% of patients (Klotz, 2008). Although medications are quite often needed for treating or managing the symptoms of health issues, the concern is more the unnecessary use of multiple medications that does not lead to optimal client health outcomes. As such, the definition of polypharmacy as ‘more than five medications’ is arbitrary, with the focus on unnecessary medication use.
Polypharmacy is one factor in the occurrence of adverse drug reactions (ADRs) in the older population, increasing the risk of drug interactions and side effects significantly. An adverse drug effect (ADE) is an injury from drug use, whereas an adverse drug reaction (ADR) is an ADE that refers to harm caused by a drug at usual dosages (Varghese et al., 2024). ADRs are seven times more likely in older adults (Burchum & Rosenthal, 2023), with the majority of these reactions related to dosages or the older adult being more sensitive to the medications. Adverse drug reactions can cause significant economic and quality of life costs related to more hospitalizations, falls, permanent injury, or death (Vallerand & Sanoski, 2024).
Therefore, it is essential to take a person-centered approach to ensure that medications are appropriate for an individual, to gain the most benefits without harm, and to ensure that clients are integral to the decision-making process.
Appropriate polypharmacy is present when:
- all medicines are prescribed for the purpose of achieving specific therapeutic objectives with which the client has agreed;
- therapeutic objectives are actually being achieved or there is a reasonable chance they will be achieved in the future; or
- medication therapy has been optimized to minimize the risk of adverse drug reactions, and the client is motivated and able to take all medicines as intended.
Inappropriate polypharmacy is present when:
- one or more medicines are prescribed that are not or no longer needed, either because there is no evidence-based indication, the indication has expired, or the dose is unnecessarily high;
- one or more medicines fail to achieve the therapeutic objectives they are intended to achieve;
- a medicine or the combination of several medicines puts the client at a high risk of adverse drug reactions; or
- the client is not willing or able to take one or more medicines as intended.
High-Risk Medications
Some medications can result in potential harm to the older adult. These include:
- warfarin,
- oral antiplatelets,
- insulin and oral hypoglycemics,
- opioids, and
- digoxin.
These medications have a higher risk of harm due to their narrow therapeutic index, risk of sedation and fall risk, patient characteristics, and monitoring requirements (Institute for Safe Medication Practices Canada [ISMP Canada], n.d.). Other drugs with increased risk are those with anti-cholinergic properties. Older adults experience more cumulative effects with these drugs; for example, they can experience impaired balance, dizziness, blurred vision, or cognitive impairment.
Drug-drug interactions pose a significant risk for adverse drug events. For example:
- Warfarin taken with NSAIDs: Risk of upper GI hemorrhage.
- Calcium channel blockers (verapamil, amlodipine) taken with macrolide antibiotics (erythromycin): Risk of hypotension (CYP3A4 inhibited by macrolides and calcium channel blockers are metabolized by CYP 3A4, leading to increased effects). (ISMP Canada, n.d.)
Drug-disease interactions also increase susceptibility for older adults. For example:
- Antihistamine medications prescribed to clients with dementia: The anticholinergic properties of antihistamines can lead to increased confusion, exacerbated confusion, or memory issues. (ISMP Canada, n.d.)
Prescribing Cascades
A prescribing cascade occurs when a client experiences a new symptom that is actually a side effect of one of their medications. They are then prescribed a new medication to treat the new symptom, leading to a cascade of prescriptions. This can continue as more medications are prescribed to treat the side effects of the new medications. It may seem implausible, but refer to the example below.
Example in Practice:
A 70-year-old client has chronic pain from a back injury:
- They have been taking NSAIDs, specifically ibuprofen, on a regular basis for a long time.
- They develop hypertension from the ibuprofen, which is then treated with the calcium channel blocker amlodipine.
- Amlodipine can cause peripheral edema, so they are prescribed the thiazide diuretic hydrochlorothiazide (HCTZ).
- HCTZ can cause dizziness, so they receive a prescription for prochlorperazine.
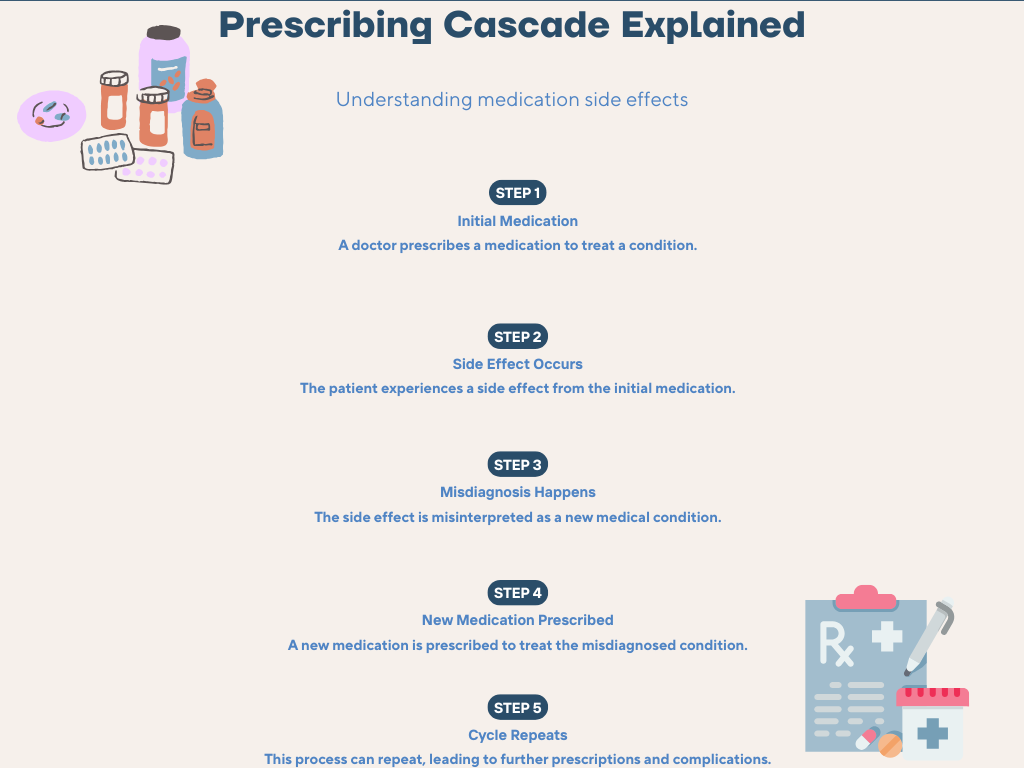
Figure 3.10a Prescribing Cascades Explained (Sheila Odubote/ TRU Open Press)
From the above example, it is easy to see how side effects can easily be treated as a new health condition but then lead to the client taking more medications and experiencing more negative effects.
It is not just older adults who are more at risk; those using multiple medicines, women, and people using ‘high-risk medicines’ (including cardiovascular drugs, NSAIDs, anticoagulants, and antibiotics) also have a higher risk of adverse drug reactions (Kalisch et al., 2011).
To minimize problematic polypharmacy in nursing:
- obtain a comprehensive health history;
- complete a medication reconciliation;
- check for medication adherence;
- identify any symptoms, including onset and duration;
- identify the client’s concerns, preferences, and goals regarding medication treatment;
- collaborate with the prescriber and other healthcare providers to share findings and perspectives on deprescribing any medications;
- consider non-pharmacological interventions to facilitate deprescribing or when a new symptom arises; and
- if a medication is deprescribed, monitor the client for improvements, worsening symptoms, and overall management. Ensure the client and their caregivers have the needed education on recognizing any symptoms early and provide additional health teaching.
References
Burchum, J., & Rosenthal, L. (2023). Lehne’s pharmacology for nursing care (11th ed.). Saunders.
Farrell, B., Raman-Wilms, L., Sadowski, C. A., Mallery, L., Turner, J., Gagnon, C., Cole, M., Grill, A., Isenor, J. E., Mangin, D., McCarthy, L. M., Schuster, B., Sirios, C., Sun, W., & Upshur, R. (2023). A proposed curricular framework for an interprofessional approach to deprescribing. Medical Science Educator, 33, 551-567. https://doi.org/10.1007/s40670-022-01704-9
Institute for Safe Medication Practices Canada. (n.d.). Safer medication use in older persons information page. https://www.ismp-canada.org/beers_list/#l=tab2
Kalisch, L. M., Caughey, G. E., Roughead, E. E., & Gilbert, A. L. (2011). The prescribing cascade. Australian Prescriber, 34(6), 162–166. https://doi.org/10.18773/austprescr.2011.084
Klotz, U. (2009). Pharmacokinetics and drug metabolism in the elderly. Drug Metabolism Reviews, 41(2), 67–76. https://doi.org/10.1080/03602530902722679
Vallerand, A., & Sanoski, C. (2024). Davis’s Canadian drug guide for nurses (19th ed.). F.A. Davis Company.
Varghese, D., Ishida, C., Patel, P., & Koya, H. H. (2024). Polypharmacy. StatPearls. Retrieved October 30, 2025, from https://www.ncbi.nlm.nih.gov/books/NBK532953/
Media Attributions
- Figure 3.10a Prescribing Cascade. (Sheila Odubote/ TRU Open Press)
