1.9 Examining a Drug’s Effects V2
How do we know if the medication that was prescribed is effective? How is it determined how much of a dose is required? How much of a dose is too much leading to toxicity? This unit will examine concepts that are important for supporting safe medication dosing and therapeutic drug monitoring.
Learning Objectives
- Apply the principles of onset, peak and duration to understand dose scheduling and monitoring for effects.
- Explain the meanings of half-life and steady state of a drug and its importance in drug dosing.
- Correlate a drug’s therapeutic index to its margin of safety.
- Differentiate between loading and maintenance dosing.
- Differentiate between peak and trough levels for therapeutic drug testing, and their importance for drug safety.
Onset, Peak, and Duration
Dosing considerations play an important role in understanding the effect that a medication may have on a client. During administration, the nurse must pay close attention to the desired effect and therapeutic response, as well as the safe dose range for any medication. The nurse should have an understanding of medication efficacy in order to ensure its appropriateness. If a nurse is provided different medication choices according to a provider’s written protocol, the nurse should select the option with the anticipated desired therapeutic response. Additionally, the nurse must be aware of the overall dose response based on the dosage selected.
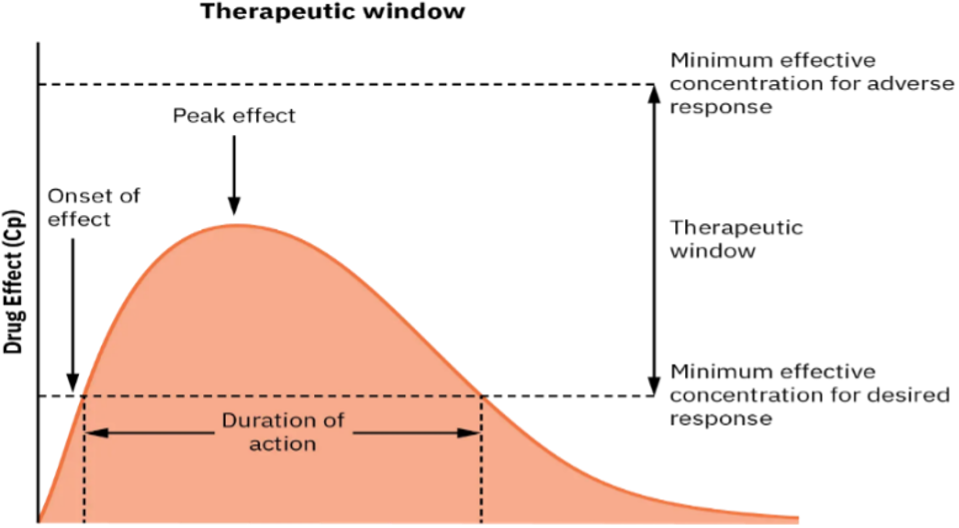
Three additional principles related to the effect of a medication on a client are onset, peak, and duration.
Onset: the onset of medication refers to when the medication first begins to take effect
Peak : the peak of medication refers to the maximum concentration of medication in the body, and the point at which the client shows evidence of greatest therapeutic effect
Duration: the duration of medication refers to the length of time the medication produces its desired therapeutic effect
Referring to the diagram below, the therapeutic window includes the onset, peak and duration of a medication. Nurses consider these three principles when preparing to administer medications to be able to know when a med will take effect, when it will be at its peak or have the strongest response and how long the med will last.
Consider this client care example and apply the principles of onset, peak, and duration: Gurmeet, a 67-year-old female client, who has just undergone hip replacement surgery earlier today, rings the call light to request medication for pain. She notes her pain is “excruciating, a definite 9 out of 10.” Her brow is furrowed, and she is grimacing in obvious discomfort. As the nurse providing care for Gurmeet, you examine her post-operative medication orders and consider the pain medication options available to you. In reviewing the various options, it is important to consider how quickly a medication will work (onset), when the medication will reach maximum effectiveness (peak), and how long the pain relief will last (duration). Understanding these principles is important in effectively relieving the client’s pain and constructing an overall plan of care.
Clinical Reasoning and Decision-Making Activity 1
- At 0500, your client, who had a total knee replacement yesterday, rates his pain while walking as 7 out of 10. Physical therapy is scheduled at 0900. The client has acetaminophen (Tylenol) 650 mg ordered every four hours as needed for discomfort. What should you consider in relation to the administration and timing of this client’s pain medication?
- Your client is prescribed NPH insulinto be given at breakfast and supper. As a student nurse, you know that insulin is used to decrease blood sugar levels in clients with diabetes mellitus. During report, you hear that the client has been ill with GI upset during the night, and the nursing assistant just informed you he refused his breakfast tray. While reviewing this medication order, you consider the purpose of the medication and information related to the medication’s onset, peak, and duration. When reviewing the drug reference, you find the NPH insulin has an onset of about 1 – 3 hours after medication administration. What should you consider in relation to the administration and timing of the client’s insulin?
Note: Answers to the Clinical Reasoning and Critical Thinking activities can be found in the “Answer Key” sections at the end of the book.
Therapeutic Window
For every drug, there exists a dose that is minimally effective (minimum effective concentration for desired response), anything below this level would be an ineffective dose, or subtherapeutic dose. Further, for every drug, there is a dose that is a maximum effective concentration (minimally effective concentration for adverse response), anything above this dose can cause adverse effects and toxic effects. In between these two doses is the therapeutic window, where the safest and most effective treatment will occur (see Figure 1.11a). Think of this area as the dosing “sweet spot.” Therapeutic window is sometimes referred to as therapeutic range.
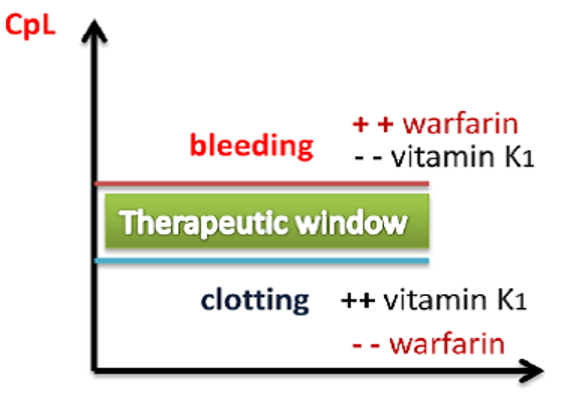
For example, warfarin (Coumadin) is a medication used to prevent blood clotting and is monitored using a blood test called INR. Too high a dose of warfarin would cause the INR to increase above the therapeutic window and put the client at risk of bleeding. Conversely, too low a dose of warfarin would cause the INR to be below the therapeutic window and put the client at risk of clotting. It is vital that the nurse frequently monitor INR levels for a client receiving warfarin to ensure the dosage appropriately reaches the therapeutic window and does not place the client at risk for bleeding or clotting.
Therapeutic Index
Therapeutic Index: is a quantitative measurement of the relative safety of a drug. It is a comparison of the amount of drug that produces a therapeutic effect versus the amount of drug that produces a toxic effect. It refers to the range of dosing that is both safe and effective. Ideally, the range is wide, so the distance from peak effect and maximum concentration is large; this would be a safe med and less chance to cause toxicity.
- Small (narrow) therapeutic index: means there is a small therapeutic window between the effective concentration and the toxic concentration. This means there is little difference between toxic and therapeutic doses. So, only a small amount of extra drug causes toxicity and a small decrease in the dosage may cause subtherapeutic effects. For example, warfarin, an anticoagulant, has a narrow therapeutic range. Too much, and the client will bleed and have a risk of hemorrhage. Too little of a dose, and the risk of blood clots is high, leading to a stroke. Medications with a narrow therapeutic range are typically monitored through therapeutic drug blood testing.
- Large (or high) therapeutic window: this means there is a large therapeutic window between the effective concentration and the toxic concentration of a medication, so the drug is relatively safe. Many drugs have a large therapeutic window and are considered quite safe and do not require drug monitoring. For example, many over-the-counter drugs are considered safe for this reason. If a client took a bigger dose than recommended, they might have more adverse effects, but not toxic effects (this does not apply to an overdose where an excessive amount is taken).
Defining Terms
You will see both therapeutic window and therapeutic index to describe the desired or therapeutic drug levels. There are differences in what they are both describing:
- Therapeutic Window. The dose range of plasma drug concentrations between the minimum concentration that is effective and the maximum concentration that is barely toxic. Between them is the therapeutic window where most safe and effective treatment will occur.
- Therapeutic Index. This is the ratio of toxic to effective doses at the level of 50% response: TD50/ED50. Therapeutic Index is a quantitative measurement of the relative safety of a drug.
Rosow, Standaert & Strichartz, n.d.
Plasma Half-life and Steady State
Plasma Half-life (t ½)
The half-life is the amount of time for serum drug concentrations to decrease by 50%. It is the rate at which the drug is eliminated from the body. Simply, it measures the drug’s effects over a period of time. After 4 t1/2’s, 94% of a drug is eliminated from the body. At five half-lives, 97% of a drug will be eliminated. So, after 4-5 half-lives, the amount of the drug left in the body so small to have any therapeutic effect. Plasma half-life’s for drugs vary, with some only a few minutes and some drugs taking days (Rosenjack Burchum & Rosenthal, 2019).
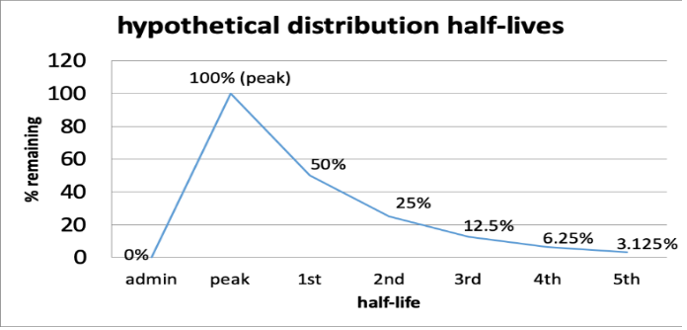
Example: A client is ordered drug X for blood pressure control. The dose is 100mg. The half-life of drug X is 60 minutes. After 4 half-lives, how much of the drug is left in the body?
- 60 minutes after administration, 50mg remains (first half life)
- 120 minutes after administration, 25mg remains (second half life)
- 180 minutes after administration, 12.5mg remains (third half life)
- 240 minutes after administration, 6.25mg remains (fourth half life)
- 300 minutes after administration, 3.125mg remains (fifth half life)
After the 4 half-lives (in 4 hours), only 6.25% remains and will have negligible therapeutic effects
How to calculate a drug’s half-life: There are formulas to determine a drug’s half-life which is directly proportional to the volume of distribution (how the drug distributes in the body) and inversely to clearance (how fast a body excretes the drug). There are online half-life calculators (to make it easy) or formulas available. Most drug manuals state the half life, along with onset, peak and duration.
Prescribers and pharmacists examine half life to help determine drug scheduling. For nurses, it helps understand how drugs are scheduled (q 2hr vs q 4hr), when the drug will be at its peak, and how long it will have a therapeutic effect. Although a drug has a specific half-life, note that other factors such as client and drug factors will lead to variations.
Client-specific factors: There are many factors to consider and can include age (pediatric vs middle aged vs geriatric), blood flow, diet, fluid status (dehydration vs fluid overload), sex, other drugs, kidney and liver function, and genetics.
Drug-specific factors: Drug formulation (i.e. immediate release vs controlled release preparations), pharmacokinetics, route of administration, protein binding, lipid vs water solubility. (Carmen, 2025)
Look at the different examples of drug half-lives. Consider how this information impacts the nursing process:
- Fentanyl IV 3-7 hours
- Morphine IV 2 hours
- Ramipril 15 hours
- Warfarin one week
Vallerand & Sanoski, 2024
Steady State of a drug
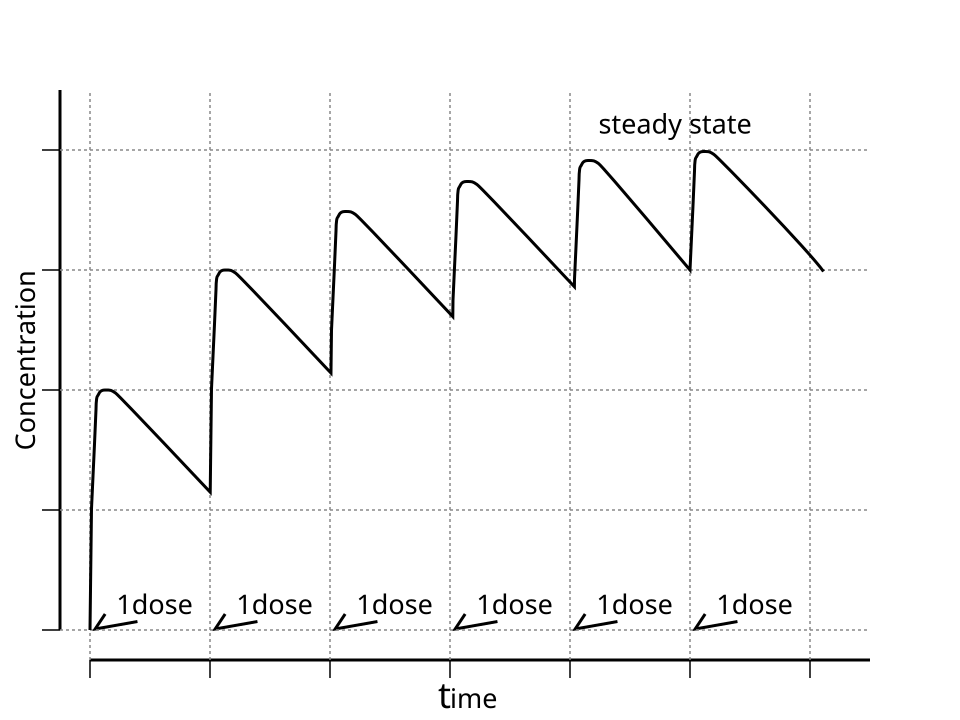
One objective of drug administration is to have a steady amount of the drug in the body so the drug can have its therapeutic effect.
Steady state = amount of drug removed/eliminated = amount of drug absorbed with each dose.
After approximately five half-lives, with the same dose and dosing interval (ie. Every 2 hours or every 4 hours), a plateau concentration or steady state of drug concentration in the blood has been achieved. Many factors can influence achieving a steady state, which are outlined above.
Duration and Dosing
What is the significance of knowing the half life, and how does this impact the drug dosing and duration of action?
Let’s consider the implication of duration and dosing. Remember the duration of medication is correlated with the elimination. If a medication has a short half-life (and thus is eliminated more quickly from the body), the therapeutic effect is shorter. These medications may require repeated dosing throughout the day in order to achieve steady blood levels of active free drug and a sustained therapeutic effect. Other medications have a longer half-life (and thus a longer therapeutic duration) and are only given once or twice per day. For example, oxycodone immediate release is prescribed every 4 to 6 hours for the therapeutic effect of immediate relief of severe pain, whereas oxycodone ER (extended-release) is prescribed every 12 hours for the therapeutic effect of sustained relief of severe pain.
Loading Dose vs Maintenance Dose
Most drugs are given in multiple doses, over a period of time, to achieve a steady state of the drug and to ultimately have the desired therapeutic effect. From what you have learnt about half-lives, this steady state can be achieved quickly if the half-life is short, or it may take days if the half life is long. But what if it is desired to speed up the time it takes to achieve therapeutic effect? For example, a client has an infection and there is concern of sepsis. The doctors would want to achieve a therapeutic dose of an antibiotic as quickly as possible. We would want to ‘load’ the drug to achieve the target plasma concentrations rapidly.
A loading dose is a higher amount of the first dose of the drug and is administered to prime the bloodstream to quickly achieve therapeutic effect. They can be only a single bolus (sometimes ordered IV with maintenance doses oral) or require multiple loading doses over a several hours or days.
Maintenance doses, are the subsequent doses to keep the plasma drug concentration in the therapeutic range.
Example in practice:
A client has a bleeding duodenal ulcer and is ordered pantoprazole IV. Loading dose: Pantoprazole 80 mg IV bolus, with maintenance dose 8 mg/hr continuous IV infusion for 24 hours. In this case, we would want to achieve steady state as quickly as possible due to the risk of hemorrhage.
Peak and Trough Levels
Now let’s apply the idea of the therapeutic window to the administration of medications that require close monitoring. For example, some antibiotics need to be titrated to achieve a desired therapeutic effect. Titration is often accomplished by closely monitoring the blood levels of the medication. A drug is said to be within the “therapeutic window” when the serum blood levels of an active drug remain consistently above the level of minimal effective concentration (so that the medication is achieving its desired therapeutic effect) and consistently below the toxic level (so that no toxic effects are occurring).
A peak drug level is drawn at the time when the medication is known to be at the highest level in the bloodstream. A trough level is drawn when the drug is at its lowest in the bloodstream right before the next dose is given.
Medications have a predicted reference range of normal values for peak and trough levels. These numbers assist the pharmacist and prescriber in gauging how the body is metabolizing, protein-binding, and excreting the drug, and will assist in the adjustment of the prescribed drug doses to keep the medication within the therapeutic window. When administering IV medications that require peak or trough levels, it is vital for the nurse to time the administration of the medication according to the timing of these blood draws.
Monitoring the Effects
As medications are administered, the nurse should perform careful client assessments, trend the assessment results, and monitor for side effects or any adverse effects. Careful assessment and monitoring are needed for each medication, especially those that have a low therapeutic window or for clients more at risk of adverse effects.
Therapeutic Effects: Therapeutic effects are the intended, beneficial, desired effects of a drug. Sometimes a drug will have more than one therapeutic effect. Aspirin is an example of a drug with multiple therapeutic effects—it can reduce fever, pain, and inflammation.
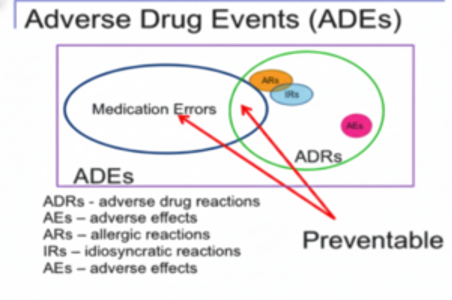
Adverse Drug Event: is the undesirable and potentially harmful action caused by the administration of a medication (Adams et al., 2018). Medication errors that cause harm are called adverse drug events.
Adverse Drug Reactions: This is any noxious, unintended and undesired effect that occurs at therapeutic or normal doses. They can range from mildly annoying to life threatening. They are more common in the children and the older adult but can occur at any age, especially in clients who are very ill or are taking many medications (Rosenjack Burchum & Rosenthal, 2019). Medication errors that cause are also called an adverse drug event (Adams et al, 2018).
Under the term of adverse drug reactions, are side effects, allergic reactions and idiosyncratic reactions.
- Side effects: A drug may cause responses that are undesirable, unintended, or secondary effects. These are known as side effects and they are usually mild and predictable (Rosenjack Burchum & Rosenthal, 2019). For example, nausea is a common side effect for many drugs. Some side effects may even be desirable. Diphenhydramine is a histamine antagonist. Because it has the side effect of drowsiness, it is sometimes used at night to occasionally aid in sleep.
- Allergic reaction: This is an immune response that can range from mild symptoms such as itching, to a severe rash and hives to anaphylaxis. Other allergy symptoms include hives, swelling, nausea, wheezing, joint pain, or anaphylaxis. The intensity of the allergic reaction is dependent on the degree of sensitization of the immune system. Fortunately, very few medications cause severe allergic reactions.
- Idiosyncratic reaction: This is a reaction that is uncommon, unpredictable and results from a genetic predisposition or immune-mediated. It is an adverse reaction that does not occur in most clients treated with a drug and does not involve the therapeutic effect of the drug. They can be life-threatening (Uetrecht & Naisbitt, 2013).
Adverse drug reactions can be mild and annoying, to being harmful and lead to injury. Let’s use aspirin as an example. An example of a common side effect is nausea, definitely annoying but often mild. A serious adverse drug effect of aspirin is gastrointestinal bleeding. Another example is morphine. Morphine, an opioid agonist, often has the side effect of constipation. However, respiratory depression is an adverse drug reaction sometimes seen with the administration of morphine and can lead to harm to client.
Drug Toxicity: Drug toxicity can occur when there is an excess accumulation of a drug in the system. The ingestion of an excessive amount of a drug might cause toxicity; however, even therapeutic doses of some drugs may cause toxicity in some clients.
Drug concentrations can also accumulate if the client has liver or renal disease and the dose was not adjusted. When a client with liver dysfunction is given a drug that is metabolized in the liver, the dosage may need to be decreased to prevent the accumulation of the drug in the body. The same is true for a client with kidney dysfunction. If the drug is primarily excreted through the kidneys, then the dosage and frequency of the drug may need to be modified. A drug excreted by the kidneys will usually be safe for the client with liver dysfunction, and vice versa (Kommu, Carter & Whitfield, 2024).
In summary:
The aim of this chapter is to introduce the learner to the basics of pharmacology and to provide a strong foundation that is needed to safely administer medications. A firm grasp on the principles of pharmacology allows the nurse to understand the drugs actions, predict adverse effects and drug interactions, and maximize drug combinations. Using clinical judgment, this knowledge will allow the nurse to effectively monitor and evaluate the client, report any possible or occurring drug effects, and provide effective client teaching so they can safely manage their medications at home. As part of the interprofessional health care team, nurses work along side other health care providers to optimize patient outcomes with minimizing adverse medication events.
Clinical Reasoning and Decision-Making Learning Activities 2
Mr. Parker has been receiving gentamicin 80 mg IV three times daily to treat his infective endocarditis. He has his gentamicin level checked one hour after the end of his previous gentamicin infusion was completed. The result is 30 mcg/ml. Access the link below to determine the nurse’s course of action.
View information on Therapeutic Drug Levels
(Within the activity link, be sure to select “click to keep reading” in order to view drugs that are commonly checked, their target levels, and what abnormal results mean).
Based on the results in the above client scenario, what action will the nurse take based on the result of the gentamicin level of 30 mcg/mL?
Note: Answers to the Clinical Reasoning and Critical Thinking activities can be found in the “Answer Key” sections at the end of the book.
Media Attributions
- Figure 1.11a Figure 1.11a The therapeutic window of a medication [Figure 2.4] is adapted from Pharmacology at Open Stax (n.d.), ©Rice University, and used under a CC BY 4.0 license.
- Figure 1.11b “Therapeutic Window” by Shefaa Alasfoor is licensed under CC BY-SA 3.0 ↵
- Figure 1.11c Distribution of Half-lives. Retrieved from Pressbooks OER https://ohiostate.pressbooks.pub/swk5805coursebook/chapter/ch-3-name/ SW5805:Theories and biological basis of substance misuse https://ohiostate.pressbooks.pub/swk5805coursebook/front-matter/introduction-to-the-coursebook1/
- Figure 1.11d Half-life steady state is by タバコはマーダー on Wikimedia Commons and used under the CC BY-SA 3.0 license.
- Figure 1.11e Adverse drug events. (Sheila Obudote/ TRU Open Press)
References
- Adams, M., Urban, C., El-Hussein, M., Osuji, J. & King, s. (2018). Pharmacology for nurses. A pathophysiological approach (2nd Canadian edition). Pearson: Ontario, Canada.
- Chippewa Valley Technical College; Egert, A., Lee, K, Gill, M. (2023). Fundamentals of Nursing Pharmacology (1stCanadian ed.). Open access Pharmacology
- https://opentextbc.ca/nursingpharmacology/chapter/1-9-examining-effect/
- Kommu, S., Carter, C., & Whitfield, P. (2024). Adverse drug reactions. StatPearls. Retrieved October 29, 2025, from https://www.ncbi.nlm.nih.gov/books/NBK599521/
- OpenStax. (n.d.). The therapeutic window of a medication includes the onset, peak, and duration of the medication (Figure 2.4). In Pharmacology. Rice University. https://openstax.org/books/pharmacology/pages/2-2-pharmacokinetics-and-pharmacodynamics
- Pope, C. (2025). Drug half-life explained. Drugs.com. Retrieved from Drug Half-life Explained: Calculator, Variables & Examples
- Rosenjack Burchum, J. & Rosenthal, L. (2019). Lehne’s Pharmacology for Nursing Care (10th ed.) Toronto: Mosby ELSEVIER
- Rosov, C., Standaert, D., & Strichartz, G. (n.d.). Principles of Pharmacology. LibreTexts. CC BY-NC-SA 4.0 licence
- Sealock, K. & Seneviratne, C. (2021). Lilley’s Pharmacology for Canadian health care professionals (4th edition). Toronto: Mosby ELSEVIER.
- Uetrecht, J. & Naibitt, D. 2013). Idiosyncratic adverse drug reactions: current concepts. Pharmacology Review, 65(2):779-808. doi: 10.1124/pr.113.007450. PMID: 23476052; PMCID: PMC3639727.
The maximum effect of which the drug is capable.
As the dose of a drug increases, the response should increase. The slope of the curve is characteristic of the particular drug-receptor interaction.
When a medication first begins to work and exerts a therapeutic effect.
When the maximum concentration of drug is in the body.
The length of time that a medication is available within the body and producing its desired therapeutic effect.
The trough level of medication indicates the lowest concentration of that medication in a person's body. Troughs of medication concentration occur after the drug has been broken down and metabolized by the body.

{kind=link}
{kind=link}