11.3 Clinical Reasoning and Decision Making for Diabetes
Assessment
Type 1 diabetes mellitus results from the autoimmune destruction of the islets of Langerhans, which are pancreatic cells responsible for producing insulin; the body is then unable to produce insulin. Most clients who first develop diabetes, present with hyperglycemia. Hyperglycemia cues include polyuria, polydipsia and polyphagia which are the typical signs. Other cues that can be present are weight loss, fatigue, irritability and blurred vision. For diagnostic testing, along with hyperglycemia and an elevated A1C level, glucosuria is present. A new onset of type 1 diabetes can lead to diabetic ketoacidosis if left untreated, which can lead to coma and death. All clients with type 1 diabetes will be on insulin therapy lifelong (Goyal et al, 2023).
In type 2 diabetes mellitus, the pancreas is capable of producing insulin but the body cannot properly utilize insulin, commonly referred to as “insulin resistance.” Overtime, the insulin production can eventually decrease. Type 2 diabetes can initially go undetected as the blood sugars may be elevated but not to the degree that serious symptoms occur. Symptom onset is usually gradual, and may include blurred vision, fatigue and recurrent infections. Clients should be assessed routinely over the age of 40 years, or if they have any predisposing risk factors (Diabetes Canada, 2026).
Risk factors for type 2 diabetes include:
- belonging to a certain ethnic group (Indigenous, Arab, African, Hispanic, South Asian),
- over the age of 40,
- overweight or obese,
- family history of diabetes,
- history of heart disease or hypertension,
- hyperlipidemia,
- history of gestational diabetes.
For type 2 diabetics who are newly diagnosed, diet and exercise are important and can sometimes increase the sensitivity of insulin receptors enough to help keep the blood sugars close to target range (HbA1C less than 7%). Exercise plays an important role in managing diabetes. Exercise increases cellular responsiveness to insulin, lowering the amount of insulin needed. The oral anti-diabetic medication, the biguanide metformin, is typically the initial drug therapy. As the disease progresses, other medications are added depending on the client’s other health issues such as heart disease, obesity or renal dysfunction.
Along with pharmacological management, all diabetic clients need to follow healthy eating habits, exercise regularly and not smoke as part of their treatment plan to prevent long term complications. Complications result from long term damage to arteries, which can lead to heart disease, stroke, kidney disease (nephropathy), and vision alterations (diabetic retinopathy). With chronically high blood sugars, there is a higher risk of infections. There can also be nerve damage with the resulting peripheral neuropathy. Lastly, it is important for the client to avoid blood glucose fluctuations from hyperglycemia to hypoglycemia within a short time frame (Goyal et al, 2023).
Hemoglobin A1C:
what it is and why is it important? To learn more about A1C, watch the following YouTube video:
Khan Academy (2011). A1C levels
Hypoglycemia is a life-threatening condition. Nurses must be acutely aware of the risk of hypoglycemia and to provide immediate treatment. Hyperglycemia is less likely to occur if medications are taken as prescribed. Report symptomatic hyperglycemia to the prescriber. For clients who have an illness or if they are under stress, anticipate blood sugar alterations and monitor more closely.
Hypoglycemia Signs and Symptoms
| Mild-to-Moderate | Severe |
|
|
Pre-assessment
- Obtain a complete health history, including allergies
- Obtain a complete medication profile, including drug interactions
- Vital signs
- Blood glucose monitoring. If infection or stress, assess more frequently for hyperglycemia
- Physical assessment may include: skin assessment for wounds, eye examination (blurred vision), numbness or tingling in feet
If on insulin therapy
- Assess appetite and plan to eat the next meal
- Blood glucose monitoring: before each meal and as needed
- Assess for hypoglycemia. For long term diabetic clients, hypoglycemia symptoms can be subtle
- Assess subcutaneous areas for insulin injections, rotate sites to avoid lipodystrophy
Implementation
The nurse should follow agency policy and ISMP guidelines for safe insulin administration. Onset and peak times of insulin and sulfonylureas, in association with anticipated meal times, should always be considered to avoid hypoglycemia episodes. If a hypoglycemia episode occurs, the nurse should intervene quickly using the agency’s established hypoglycemia protocol, and the event should be reported to the provider and in the shift-to-shift report.
Hypoglycemia Protocol
In the event of hypoglycemia, with blood sugars less than 4.0 mmol/L or if a change in mood or mental status or other signs of hypoglycemia, quickly follow the agency protocol. Hypoglycemia protocols contain orders for immediate treatment by the nurse.
This will include:
- give a fast-acting carbohydrate (simple sugar): 15-20 grams glucose tablets, 125 ml of juice, honey or glucose tablets. If unable to swallow, the nurse may give honey, but be aware of aspiration risk. If NPO or unconscious, give dextrose 50% IV or glucagon 1 mg IM/SQ.
- goal of therapy is blood glucose greater than 4 mmol/L. Repeat blood glucose every 15 minutes x 2 and give fast-acting carbohydrate until blood sugar is above 4 mmol/L,
- after 3 rounds of simple sugar, and if more than one hour before next meal, eat a snack of a starch (crackers, toast) and protein (milk, cheese, peanut butter).

Orange juice (50531482356).jpg (amanda.sophia.ac at https://flickr.com/photos/190653512@N07/50531482356)
Monitor closely for the following 24 hours because they are at increased risk for another episode. The provider and the oncoming nurse should be notified of hypoglycemia episodes todiscuss the possible cause of the hypoglycemic event and make insulin adjustments, if needed, to avoid additional hypoglycemia. Tracking hypoglycemia episodes and analyzing causes are important performance improvement activities (Seggelke & Everhart, 2012).
Client education is a vital component of effectively managing diabetes. Client education should be provided to clients, family members, and/or caregivers according to ISMP guidelines.
-
- All clients must know the signs or symptoms of hypoglycemia
- All clients must know how to avoid and treat hypoglycemia
- Ensure clients follow a healthy diet and exercise plan
- Check blood sugars as required by their prescriber and as needed.
- Follow the recommendations for insulin therapy or for oral anti-diabetic medications to avoid adverse effects (see insulin therapy or oral anti-diabetic medication sections for more detailed information).
Evaluation
Monitor for complications
As mentioned in the assessment, complications will occur with long term diabetes or with diabetes that is poorly managed. Assessing for any signs of complications such as blurred vision, numbness or tingling in the feet, or poorly healing wounds. Routinely ask the client about these symptoms to identify early any changes.
Avoid hypoglycemia and hyperglycemia
Effective management requires a client who is able to follow the treatment plan such as check blood sugars as required, take their anti-diabetic medications as prescribed, and avoid hyperglycemia or hypoglycemia episodes. Along with blood sugar levels, completion of routine A1C levels to determine effectiveness of the treatment regimen.
Diabetic Ketoacidosis
Although severe hyperglycemia is less common than hypoglycemia, recognizing cues is important to avoid diabetic ketoacidosis. Severe hyperglycemia cues include the 3 P’s: polyuria, polydipsia and polyphagia along with abdominal pain and nausea. The characteristic fruity breath is another cue. Hyperglycemia can be due to infection, inadequate insulin or skipping doses. So, any uncontrolled elevations in blood sugars must be examined.
Acetone fruity odour to the breath can occur when glucose is unable to enter cells, and lipids are used as an energy source and keto acids are produced as waste products. The keto acids give the client the fruity breath odor. The high levels of ketones lower the pH of the blood, leading to diabetic ketoacidosis. This is a life-threatening condition that can result in coma and death if not treated promptly (Adams et al, 2018).
If hyperglycemia occurs while on insulin therapy, notify the prescriber and anticipate a trip to the emergency department for a thorough assessment and treatment. Treatment includes IV insulin, electrolyte and fluid replacement (Lizzo, Goyal & Kaur, 2025).
Management of blood sugars for all diabetic clients includes:
- healthy diet, physical activity and a healthy lifestyle (i.e. no smoking, minimal alcohol intake).
- A goal of tight glycemic control that includes an A1C less than 7% and to maintain blood glucose levels within normal range.
Type 1 diabetics will be on insulin that includes both basal and bolus (prandial) insulin.
Type 2 diabetics will be on one or more oral anti-diabetic medications, depending on their glycemic control. If the oral meds are no longer effective, insulin may be added.
Hypokalemia
Hypokalemia is one of the most common electrolyte disturbances secondary to poor glycemic control. All insulin products cause a shift in potassium from the extracellular to intracellular space, which can possibly lead to hypokalemia. Hypokalemia is defined as serum potassium concentration less than 3.5 mEq/L. The main causes of hypokalemia in diabetics are the use of high doses of insulin or when attempting to correct diabetic ketoacidosis or hyperglycemic hyperosmolar state. The other cause of hypokalemia is the use of diuretics such as thiazides or loop diuretics (Coregliano-Ring, Nishide & Rangel, 2022). Mild cases of hypokalemia can present as muscle weakness, fatigue, cramping and heart palpitations. If severe, cardiac dysrhythmias, respiratory failure and severe abdominal pain. Monitor potassium levels in clients at risk for hypokalemia due to other medications such as diuretics.
Glycemic control during sick days
Clients who are sick, either at home or in the hospital, will need closer monitoring. Blood sugars should be checked every 2-4 hours, and if blood sugars are high, then also check urine ketones every 2 – 3 hours. Hydration and food are important so drinking at least 250 cc of fluids and eating 15 grams of carbohydrates every hour. If the client is on insulin, continue to take insulin and anticipate higher prandial dose needs. If the client is on oral anti-diabetic meds such as metformin or SGLT-2 inhibitors, the prescriber may temporarily stop these meds until they are feeling better. For clients managing their illness at home, advise them that if blood sugars are over 16.1 mmol/L, there is high ketones in the urine, or they cannot eat or drink, they should plan to go to the hospital.
Alcohol and Diabetes
Clients with diabetes can continue to drink alcohol but need to drink in moderation, which is considered 1-2 drinks/day or depending on if their diabetes is under control, or if they have other health considerations. Key points to consider if a client plans to consume alcohol and they are on insulin:
- Before consuming alcohol, continue to eat regular meals. While drinking, eat carbohydrate-rich foods and consider alternating between alcoholic and non-alcoholic beverages. After drinking, ensure there is a responsible person who knows how to monitor for signs of hypoglycemia.
- Delayed hypoglycemia: hypoglycemia may occur up to 24 hours after alcohol consumption
- Morning hypoglycemia: if a client consumes alcohol 2-3 hours following an evening meal, hypoglycemia may occur in the morning
- Check blood sugars more often for the next 24 hours.
For more information, go to Diabetes Canada (2026). Alcohol and Diabetes: https://guidelines.diabetes.ca/GuideLines/media/Docs/Patient%20Resources/alcohol-and-diabetes.pdf
Lifespan Considerations
Older Adult
The older adult are at higher risk for hypoglycemia episodes. The following are evidence-based recommendations for elderly clients with diabetes:
- In older adults at increased risk of hypoglycemia, medication classes with low risk of hypoglycemia are preferred.
- Overtreatment of diabetes is common in older adults and should be avoided.
- Deintensification (or simplification) of complex regimens is recommended to reduce the risk of hypoglycemia, if it can be achieved within the individualized A1C target (American Diabetes Association, 2019).
Children and Adolescents
Type 1 diabetes is the most common form of diabetes in youth. Unique aspects of care and management of children and adolescents with type 1 diabetes must be considered, such as changes in insulin sensitivity related to physical growth and sexual maturation, ability to provide self-care, supervision in the child care and school environment, neurological vulnerability to hypoglycemia and hyperglycemia in young children, as well as possible adverse neurocognitive effects of diabetic ketoacidosis (DKA). Evidence-based recommendations for glycemic control for children and adolescents include:
- The majority of children and adolescents with type 1 diabetes should be treated with intensive insulin regimens, either via multiple daily injections or continuous subcutaneous insulin infusion.
- All children and adolescents with type 1 diabetes should self-monitor glucose levels multiple times daily (up to 6–10 times/day), including pre-meal, pre-bedtime, and as needed for safety in specific situations such as exercise, driving, or the presence of symptoms of hypoglycemia.
- Continuous glucose monitoring should be considered in all children and adolescents with type 1 diabetes, whether using injections or continuous subcutaneous insulin infusion, as an additional tool to help improve glucose control. Benefits of continuous glucose monitoring correlate with adherence to ongoing use of the device.
- Automated insulin delivery systems appear to improve glycemic control and reduce hypoglycemia in children and should be considered in children with type 1 diabetes.
- An A1C target of <7.5% should be considered in children and adolescents with type 1 diabetes but should be individualized based on the needs and situation of the client and family (American Diabetes Association, 2019).
The following concept map provides a summary of key information to help understand glucose regulation. You can revisit this map after you have completed the chapter. The information for the map was informed by several resources (Giddens, 2017, pg. 241).
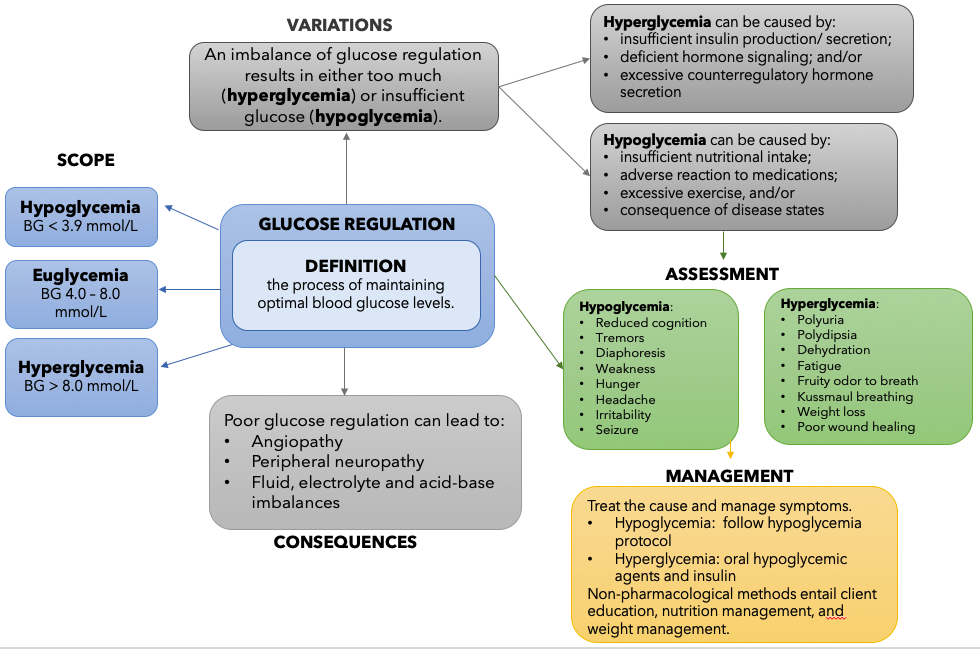
Image Description
Figure 11.3b Glucose Regulation Concept Map description: This flowchart describes the Concept of Glucose Regulation. In the centre of the chart, Glucose Regulation is defined.
The definition of the Concept of Glucose Regulation is: the process of maintaining optimal blood glucose levels.
Next, there are 3 arrows pointing from the definition to the Scope of Glucose Regulation. The scope is divided into 3 categories: Hypoglycemia (BG < 3.9 mmol/L), Euglycemia (BG 4.0 – 8.0 mmol/L), and Hyperglycemia (BG > 8.0 mmol/L).
Next, one arrow points from the definition to the Variation of Glucose Regulation. An imbalance of glucose regulation results in either too much (hyperglycemia) or insufficient glucose (hypoglycemia). Both hyperglycemia and hypoglycemia are further described.
- Hyperglycemia can be caused by: insufficient insulin production/ secretion; deficient hormone signaling; and/or excessive counterregulatory hormone secretion.
- Hypoglycemia can be caused by: insufficient nutritional intake; adverse reaction to medications; excessive exercise, and/or consequence of disease states.
Next, an arrow points down towards Assessment for Glucose Regulation. Here, a summary of hypoglycemia and hyperglycemia symptoms are listed.
- Hypoglycemia: Reduced cognition, Tremors, Diaphoresis, Weakness, Hunger, Headache, Irritability, Seizure.
- Hyperglycemia: Polyuria, Polydipsia, Dehydration, Fatigue, Fruity odor to breath, Kussmaul breathing, Weight loss, Poor wound healing.
Media Attributions
- Figure 11.3a Orange juice (50531482356).jpg (amanda.sophia.ac/ Wikimedia Commons) at https://flickr.com/photos/190653512@N07/50531482356)
- Figure 11.3b Glucose Regulation Concept Map [Image Description]
References
Adams, M., Urban, C., El-Hussein, M., Osuji, J. & King, S. (2018). Pharmacology for Nurses. A pathophysiological approach (2nd Canadian ed.). Pearson Canada Inc: Ontario.
American Diabetes Association (2019). Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2019. Diabetes Care 42(S1). https://doi.org/10.2337/dc19-S009 ↵
Coregliano-Ring, L., Nishide K., & Rangel, E. (2022). Hypokalemia in diabetes mellitus setting. Medicina (Kaunas), 58(3):431. doi: 10.3390/medicina58030431
Diabetes Canada (2026). Managing diabetes. https://www.diabetes.ca/about-diabetes
Goyal, R., Singhal, M., Jialal, I. & Castano, M. (2023). Type 2 Diabetes (Nursing). National Library of Medicine. StatPearls [Internet]. Type 2 Diabetes (Nursing) – StatPearls – NCBI Bookshelf
Lizzo, J., Goyal, A. & Kaur J. (2025). Adult diabetic ketoacidosis. National Library of Medicine. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK560723/
Seggelke, S., Everhart, B. (2012, September 11) Managing glucose levels in hospital patients. American Nurse Today. https://www.americannursetoday.com/managing-glucose-levels-in-hospital-patients/.
