3.9 Medication Safety Across the Lifespans — Pediatrics
Amanda Egert
Medication Safety in the Pediatric Population
Children are particularly vulnerable to adverse drug events, particularly infants and young children. Children are more likely to experience an adverse drug reaction compared to adults, regardless if they are in a hospital or community setting. Adverse drug reactions in children range from 0.4–10.3% (Meyers et al., 2020). Other studies found that the potential for adverse drug events (ADEs) in children was three times higher compared to hospitalized adults (Goldman & Konen, 2007). Many ADE are preventable.
Factors that increase adverse drug reactions in pediatrics include:
Drug prescribing and dosing, such as medication labelling issues, calculating errors based on weight, and lack of available dosage forms and concentrations. Most adverse reactions are due to dosing errors. For example, the ’10-fold error’ with weight based calculations involves a misplaced decimal point when converting milligrams to micrograms for drug dosing.
Pharmacokinetic variations are inherent in maturational changes in body composition and organ function, especially with young children. As children age, total body water decreases and body fat increases, which will affect drug transport and metabolizing enzymes. Neonates are particularly vulnerable to ADEs. For example, neonates have thinner skin, leading to increased absorption through the skin. The development of renal function (glomerular filtration) is complete by the first year of life, but prior to that, drugs will have a delayed excretion leading to prolonged effects (Meyers et al., 2020).
Communication, such as using non-verbal communication with young children as an early detector of symptoms (Goldman & Koren, 2007). Very young children are less able to clearly communicate than an older child. Language barriers can also be a factor. Nurses need to be skilled in assessing for subtle changes.
Polypharmacy for children with complex or chronic diseases (Meyers et al., 2020). Children on multiple medications are at risk of drug interactions and more side effects, similar to the adult population, except these effects are often more pronounced. As with adults, always consider the appropriateness of all prescribed and OTC medications.
Lack of published information on labelling, safety, efficacy, and clinical use of drugs (Goldman & Koren, 2007). Clinical trials of medications on children are sparse due to ethical reasons and safety concerns. One of the challenges with drugs in pediatric clients is the limited testing when researching the drug. In general, almost all information about drugs is related to dosing in adult clients. The risk of performing research in the pediatric population and obtaining informed consent makes researching drugs a problem.
KIDs List
To improve med safety, pediatric pharmacists developed a list of medications, called the KIDs List (Key Potentially Inappropriate Drugs in Pediatrics), to identify those associated with a high risk for ADEs; they planned to evaluate and enhance the quality of care, decrease costs, and identify areas of pediatric research (Meyers et al, 2020). The potentially inappropriate medications are those that should be avoided in persons younger than 18 years of age due to a high safety risk. There are 39 drugs and drug classes on the list, which is intended to be a guide and not an absolute contraindication. The KIDs List includes two recommendation levels: avoid and use with caution.
For example:
- Codeine: Risk of respiratory depression and death.
- Bismuth subsalicylate: Risk of Reye’s syndrome.
- Tetracycline: Risk of tooth discoloration and enamel hypoplasia.
The same principles for safe medication administration for adults are identical for children, such as performing seven (or 10) rights of medication administration or verifying unclear orders. Nursing strategies to reduce med errors in children should include:
- performing the seven rights of med administration;
- Having an independent second nurse verifier;
- confirming the correct weight on each drug chart;
- updating skills in calculating drug doses (consider age, weight, height, maturational state, and body surface area);
- verifying unusual drug volumes or doses; and
- listening to the client, parent, or caregiver (listen, answer questions, and double check orders).
Always check with your facility on procedures for drug administration with children. Many facilities will have standard policies in place to minimize drug errors.

Figure 3.9b Illustration of Boy Taking Pharmaceutical Oral Dosage Pills with Glass of Water
Calculating Pediatric Drug Dosages
Two common ways to calculate pediatric dosages are the body weight method and the body surface area method. Sometimes, the order is already taking into account the child’s weight, which is verified with the pharmacist. In this case, the calculation can simply be done with ‘desire or have’ formula.
Desire over Have Formula
Example in practice:
order reads: Famotidine 100mg po BID.
The suspension is 40 mg/5 mL
Desire: 100mg = x mL Have: 40 mg 5 mL 40mgx = 500 x= 500/40 = 12.5 mL
Body Weight Method (mg/kg)
The body weight method uses the child’s weight to calculate milligrams of drug (mg/kg). Time may also be included. Although relatively easy to use, this method does not consider pharmacokinetic variables or serum concentrations of many drugs that are not proportional to body weight. Additionally, care must be taken to ensure pounds are converted to kilograms (1 kg = 2.2 lb).
Example in practice: A three-year-old child has a fever and is prescribed acetaminophen.
The order reads: Acetaminophen 10-15 mg/kg/dose every 6 hours as needed. Do not exceed 3 gms.
The child weighs 30 pounds. The nurse assesses the child’s pain and decides to give the lower dose.
Acetaminophen concentration (suspension) is 160 mg in 5 mL.
| Step | Calculation |
|---|---|
| Step 1. Convert pounds to kg. | 30 lb × 1 kg/2.2 lb = 13.6 kg |
| Step 2. Calculate the dose in mg. | 13.6 kg × 10 mg/kg/dose = 136 mg/dose |
| Step 3. Convert the mg dose to mL. | 136 mg/dose ÷ 160 mg/5 mL = 4.25 mL |
Example in practice: A one-year-old child is diagnosed with otitis media. They weigh 22 lb (10 kg)
The order reads: Amoxicillin oral suspension 40 mg/kg/day in 2 divided doses.
The suspension is available at a concentration of 400 mg/5 mL. How many milliliters should be administered to the child for each dose?
| Step | Calculation |
|---|---|
| Step 1. Convert pounds to kg. | 22 lb × 1 kg/2.2 lb = 10 kg |
| Step 2. Calculate the dose in mg. | 10 kg × 40 mg/kg/dose = 400 mg/dose |
| Step 3. Divide the dose by the frequency. | 400 mg/day ÷ 2 = 200 mg/dose |
| Step 4. Convert the mg dose to mL. | 200 mg/dose ÷ 400 mg/5 mL = 2.5 mL |
Body Surface Area Method (mg/m2)
Calculating pediatric drug dosages using the body surface area (BSA) method can be done using a nomogram or formula. It is used less often but still used for chemotherapy drugs. The BSA is the most accurate method as it considers physiological and pharmacokinetic differences.
Nomogram: The child’s height and weight are plotted on a nomogram. The line drawn between two points and where it intersects is the BSA.
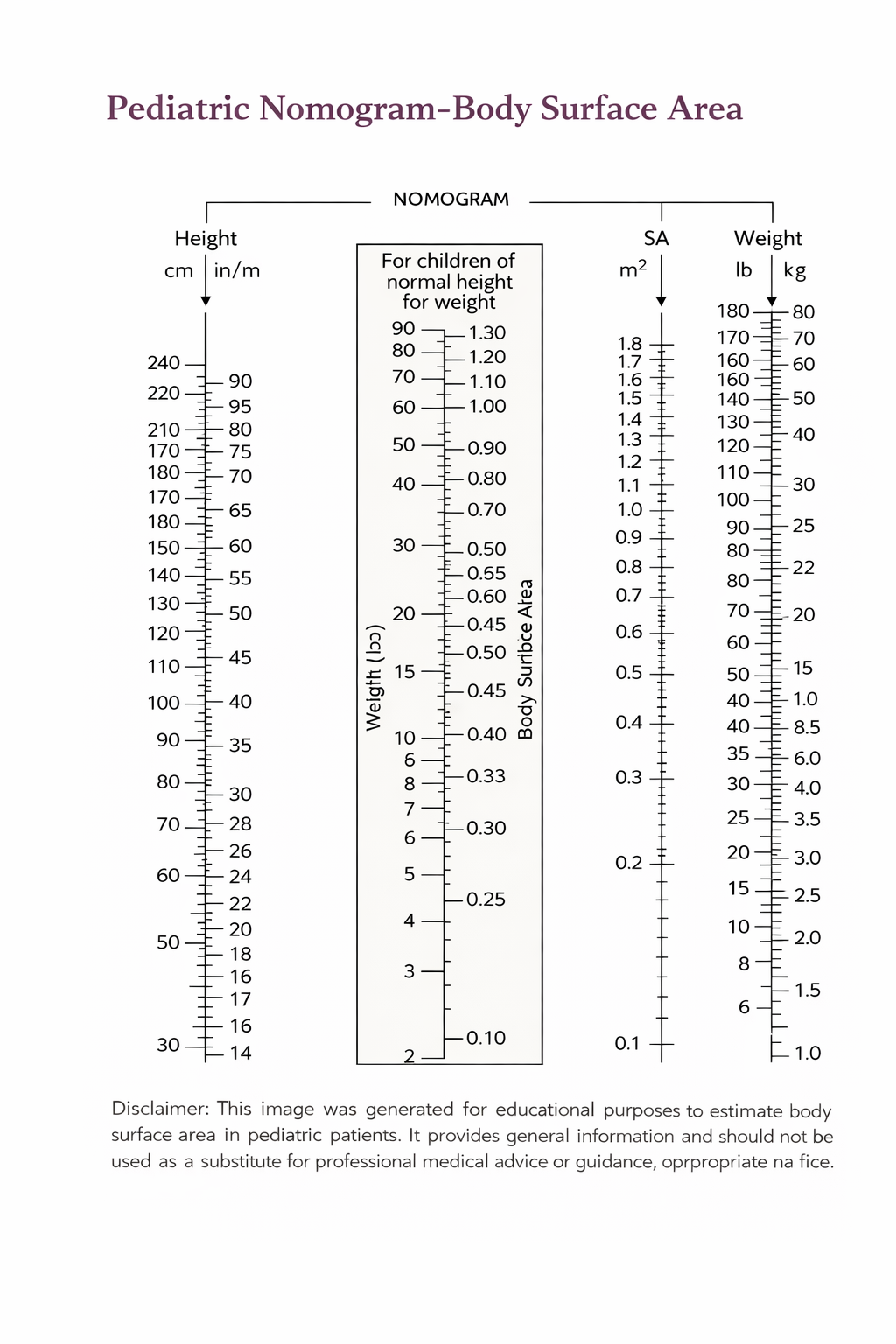
Figure 3.9b Pediatric Nomogram for Body Surface Area (Sheila Odubote/ TRU Open Press).
The responsibility for preventing medication errors is a multidisciplinary approach beginning with facility policies, electronic order sets to avoid written errors (misspelled drugs or doses), prescriber actions, pharmacy guidelines and actions, nursing interventions, and client involvement (Adams et al., 2018).
Clinical Reasoning and Decision Making Activity
- The 6-month old infant is ordered a liquid medication that is 0.75 mL. The nurse is deciding what is the best way to draw up and give this med. He looks over the syringe options (1-mL, 3-mL, 5-mL), or a calibrated plastic med cup. Which is the best option and what is your rationale?
- A child is to receive 60 mg of phenytoin. The med is available as an oral suspension that contains 125 mg/5 mL. How many milliliters should the nurse administer?
- Based on a child’s report of pain, the plans to administer the prescribed morphine. The med is available in a 10mg predrawn syringe. The nurse will have 4 mg of waste. The wasting of the med is done by the nurse and a witness. Who can be a witness?
Check your answers in the Chapter 3 answer key section.
Note: Answers to the Clinical Reasoning activities can be found in the “Answer Key” sections at the end of the book.
Supplemental Resource
Below are supplementary learning resources related to client safety and error prevention during medication administration.
Client Example of Medical Errors
Watch the Josie King Story to gain perspective from a family who has experienced a medical error with their child.
Introducing the Partnership for Patients with Sorrel King [4:50min] by HealthCare.gov (2011).
https://youtube.com/watch?v=ak_5X66V5Ms%3Ffeature%3Doembed%26rel%3D0
References
Adams, M. P., Urban, C. Q., El-Hussein, M., Osuji, J. & King, S. (2018). Pharmacology for nurses. A pathophysiological approach (2nd Canadian ed.). Pearson.
Goldman, R. & Koren, G. (2007). Keeping it safe in the paediatric emergency department – drug errors and ways to prevent them. Paediatric Child Health, 12(6), 461–464.
Meyers, R., Thackray, J., Matson, K., McPherson, C., Lubsch, L., Hellinga, R., Hoff, D. (2020). Key potentially inappropriate drugs in pediatrics: the KIDs list. Journal of Pediatric Pharmacology Therapeutics, 25(3), 175–191.
Vallerand, A. H. & Sanoski, C. (2024). Davis’s Canadian drug guide for nurses (19th ed.). F.A. Davis Company.
Media Attributions
- Figure 3.9a Illustration of Boy Taking Pharmaceutical Oral Dosage Pills with Glass of Water https://www.wannapik.com/vectors/12542
- Figure 3.9b Figure 3.9b Pediatric Nomogram for Body Surface Area (Sheila Odubote/ TRU Open Press). Figure 3.9b Pediatric Nomogram for Body Surface Area (Sheila Odubote/ TRU Open Press). https://www.scribd.com/document/53587761/Nomogram
