3.12 Strategies Towards Medication Safety in Older Adults
Since many adverse drug events are avoidable, a few tools have been developed to assist healthcare providers in identifying medications of concern. Some tools include STOPP/START, Appropriate Medication Index, and the ones we will focus on in this unit, Beer’s Criteria and Deprescribing for Safer Care.
Beers Criteria for Potentially Inappropriate Medication Use in Older Adults
To help mitigate the risk for older adults, the American Geriatric Society publishes the “Beers Criteria” (or “Beers List”), which represents a consensus list of potentially inappropriate medications that all healthcare providers can refer to. The Beers List was originally developed by Dr. Mark Beers and an American panel of experts in 1991. It was recently updated and is used to improve the safety of prescribing and use of drugs in older adults.
There are close to 100 medications or medication classes on the Beers Criteria list. The criteria to list potentially inappropriate medications for adults over 65 are ones that can put the client at risk such as drugs that have higher risk of adverse drug interactions, harmful side effects that outweigh the benefits and meds to use short term due to impaired kidney function. Some medication classes include anti-cholinergic medications, proton pump inhibitors, and benzodiazepines.
The Beers List is a tool that helps prescribers consider other medication options or dosing to minimize the client’s risk. It is designed to highlight potentially inappropriate medications; these medications are not absolutely unacceptable in all cases or for all people.
Beers Criteria can be accessed in most drug guides, or you can access it from the Guideline Central website at Beers Criteria for Potentially Inappropriate Medication Use in Older Adults (American Geriatrics Society, 2025).
To learn more about the Beers Criteria, refer to the Institute for Safe Medications Canada’s (n.d.) Safer Medication Use in Older Persons Information Page.
Deprescribing for Safer Care
Deprescribing involves reducing or stopping medications that are causing more harm than good or are no longer needed. It is an important approach to managing polypharmacy and is not just for prescribers but also all healthcare providers (Canadian Medication Appropriateness and Deprescribing Network [CADeN], n.d.). It is also a client-centered, planned, and supervised process of drug reduction or stopping of a medication that may be causing harm or no longer providing benefit (Farrell et al., 2023).
The overall aim of deprescribing is to:
- improve quality of life;
- avoid the worsening of disease or causing withdrawal effects;
- reduce pill burden; and
- improve control of chronic conditions.
Is this medication the best choice for this client at this time? Clients are started on medications and over time, even years, they are still on that same medication. As a client gets older or has other health issues arise, that medication might not be the best choice anymore. To best manage chronic health conditions and avoid adverse effects, the goal of deprescribing is to minimize medication burden and improve quality of life.
Can the prescriber just stop medications or switch the client to a different medication? Sometimes this is possible, but with some medications, abruptly stopping it will produce withdrawal effects or worsen the client’s condition. Deprescribing is the best option and is a planned and supervised process of dose reduction. It sometimes involves stopping a medication if it is causing harm or is not beneficial. Deprescribing is client-centred and often involves a collaborative approach between the client and their healthcare providers.
The Canadian Medication Appropriateness and Deprescribing Network (CADeN) has developed algorithms and guidelines to provide support to practitioners. For example, the Proton Pump Inhibitor Deprescribing Guidelines includes a detailed algorithm and patient information sheets. To view this deprescribing algorithm along with other algorithms and guidelines, go to deprescribing.org’s (n.d.a) Deprescribing Guidelines and Algorithms page.
Other medications that have deprescribing guidelines include benzodiazepines, anti-hyperglycemics, and antipsychotics.
Deprescribing involves all healthcare providers. To understand the client’s medication experience, the expertise and knowledge of all healthcare providers involved with the client is invaluable. For example, physiotherapists can offer non-pharmacological strategies in managing pain or be alert to adverse reactions from prescribed medications.
What is the nurse’s role in deprescribing? Registered nurses do not prescribe medications, but they do have an important role in deprescribing. When a client is actively involved in the deprescribing process, client education, ongoing assessments, and monitoring are some important roles for nurses. Take a look at some of the deprescribing algorithms or guidelines and consider how nurses have an active role in the process. To view these deprescribing algorithms and guidelines, go to deprescribing.org’s (n.d.a) Deprescribing Guidelines and Algorithms page.
Deprescribing Competencies
As part of a larger deprescribing initiative, the CADeN has identified the following framework (Figure 3.12.1) that all entry-to practice physicians, pharmacists and nurses should perform successfully. The seven competencies are to be applied in collaboration with the client and their family members.
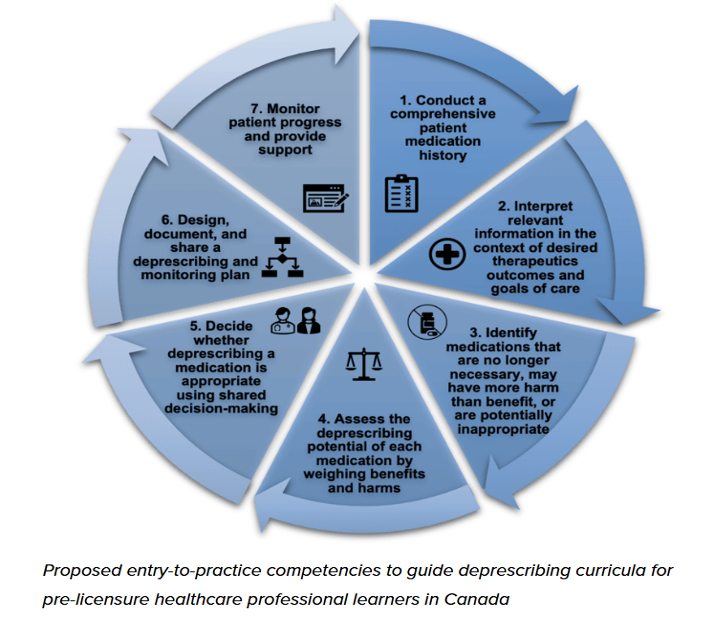
Retrieved from Deprescribing Network at Educational framework for deprescribing — Do I still need this medication? Is deprescribing for you?
Look at each competency and consider how nurses’ involvement in each is invaluable. As part of nurse’s role in safe medication administration, and the nursing process overall, consider how adding a deprescribing lens to medication administration can be easily included.
Learning Activity
Deprescribing in Ontario Long-Term Care
Go to the Deprescribing in Ontario Long-Term Care page on deprescribing.org (n.d.b).
On the page, watch the case scenario for Agatha Smith. (The video is also available on YouTube.)
Observe how the family members’ concerns are addressed. Although the family member is speaking with a physician, the nurse is very often one of the first healthcare provider families will speak to about concerns.
Healthcare providers’ role to minimize the risk:
- Assess clients for new onset of symptoms that could be an adverse reaction, especially if they started on a new medication therapy. Most ADRs occur within the first four months of prescribing a new medication, so it is important to do follow-up appointments and specifically ask about any new symptoms, including onset and duration of effects.
- Provide health teaching to clients so they are aware of potential effects from their medications. Provide clear information and use take-home pamphlets or other resources.
- Recognize that lower doses are often prescribed for older, frail clients. Inquire about orders that may be a regular or larger dose.
- When drug reactions occur, non-drug treatment strategies are likely the most appropriate first-line management, rather than starting a second medicine to counteract adverse effects.
To learn more about deprescribing, go to deprescribing.org’s (n.d.c) Resources for Patients and Healthcare Providers page.
Putting It All Together
This unit focused on the many variables that can impact medication safety, including barriers and strategies to improve safety. Nurses have an important role in ensuring that clients have the least amount of risk with their medications. It starts with a thorough medication history and a patient-centered medication review. A holistic approach will help identify any barriers or supports, such as literacy levels and cultural or social factors. Nurses also need to consider medication safety across lifespans as some medications can put some clients more at risk, which will require strategies to overcome that risk. Lastly, there are many strategies and tools already developed to assist nurses and healthcare teams. It begins with an awareness of the strategies, good collaboration between healthcare team members, and a commitment to incorporate those strategies into our practices.
BC Patient Safety and Quality Council
The BC Patient Safety and Quality Council (BCPSQC) was the basis for many references in this chapter; it also has several other resources that may be beneficial to your learning about client safety related to medication administration.
The council provides system-wide leadership for efforts designed to improve the quality of healthcare in British Columbia. Through collaborative partnerships with health authorities, clients, and those working within the healthcare system, BCPSQC promotes and informs a provincially coordinated, client-centred approach to client safety and quality. The council also provides numerous resources for healthcare professionals to help build competence in safety and quality.
To view and register for upcoming learning programs related to client safety and quality, visit the BCPSQC website.
Acknowledgements
This chapter is adapted from information provided by the Canadian Medication Appropriateness and Deprescribing Network’s Healthcare Providers Committee and Education Committee.
References
American Geriatrics Society. (2025). Beers Criteria for potentially inappropriate medication use in older adults. Guideline Central. https://www.guidelinecentral.com/guideline/340784/
Canadian Medication Appropriateness and Deprescribing Network. (n.d.). What is deprescribing? https://www.deprescribingnetwork.ca/deprescribing
Deprescribing.org. (n.d.a). Deprescribing guidelines and algorithms. https://deprescribing.org/resources/deprescribing-guidelines-algorithms/
Deprescribing.org. (n.d.b). Deprescribing in Ontario long-term care. https://deprescribing.org/resources/deprescribing-in-ltc-framework/
Deprescribing.org. (n.d.c). Resources for patients and healthcare providers. https://deprescribing.org/resources/
Farrell, B., Raman-Wilms, L., Sadowski, C. A., Mallery, L., Turner, J., Gagnon, C., Cole, M., Grill, A., Isenor, J. E., Mangin, D., McCarthy, L. M., Schuster, B., Sirios, C., Sun, W., & Upshur, R. (2023). A proposed curricular framework for an interprofessional approach to deprescribing. Medical Science Educator, 33, 551-567. https://doi.org/10.1007/s40670-022-01704-9
Health Quality BC. (n.d.). Sharpen your Skills. https://healthqualitybc.ca/sharpen-your-skills/
HealthCare.gov. (2011, May 25). Introducing the partnership for patients with Sorrel King [Video]. YouTube. https://youtu.be/ak_5X66V5Ms?si=esdwCyRhtczPV5yp
Institute for Safe Medication Practices Canada. (n.d.). Safer medication use in older persons information page. https://www.ismp-canada.org/beers_list/#l=tab2
Media Attributions
Figure 3.12a Deprescribing Competencies. Retrieved from Deprescribing Network at Educational framework for deprescribing — Do I still need this medication? Is deprescribing for you?
- Systems Factors” was adapted from Medication Safety in High Risk Situations by World Health Organization, which is licensed under a CC BY-NC-SA 3.0 licence.
- “Medication Safety in Polypharmacy” was adapted from Medication Safety in Polypharmacy by World Health Organization, which is licensed under a CC BY-NC-SA 3.0 licence.
- Healthcare.gov. (2011, May 25). Introducing the Partnerships for Patients with Sorrel King [Video]. YouTube. https://youtu.be/ak_5X66V5Ms ↵
Long Descriptions
Figure 3.12.1 Long Description: This is a circle divided into 4 quadrants to depict 4 areas where medication discrepancy can occur:
- Community: 14-98% of community-dwelling older person and 27-57% of those in residential aged care facilities had medication discrepancies.
- Hospital admission: 3-97% of adult patients and 22-72% of pediatric patients had at least one medication discrepancy at admission.
- Discharge: 25-80% of patients had at least one medication discrepancy at discharge.
- Transfer within hospital: 62% of patients had at least one unintentional medication discrepancy at transfer between units in hospital. [Return to Fig 3.12.1]
