1.6 Pharmacokinetics — Excretion
Excretion is the process by which a drug and its metabolites are eliminated from the body. Although the kidneys are the primary organ for excretion, some drugs may also be excreted through the liver by the biliary system with minimal amounts excreted through other routes such as saliva and tears.
Drug elimination is a complex process that includes excretion of an unmetabolized drug in an intact form or excretion following a metabolic transformation (Garza et al., 2023). Other factors also impact excretion such as the drug characteristics and client factors such as age, genetics, and other health issues. For example, if a client has dysfunction with their kidney or liver, drug excretion will be prolonged and can lead to undesirable adverse effects and prolonged therapeutic effects. Nurses need to consider how a delayed excretion can alter their assessment and client monitoring.
In this unit, we will look at the many factors that can impact drug excretion, including drug characteristics, routes of excretion and lifespan considerations.
Drug Characteristics
Drug excretion is impacted by the drug’s characteristics, such as the polarity of the drug or the size of the drug metabolite.
Hydrophilic drugs are typically directly excreted by the kidneys. These drugs or their metabolites get filtered by the kidneys and usually do not undergo reabsorption. Drugs that are lipophilic need to first undergo biotransformation to become more polar before undergoing elimination through the kidneys (Garza et al., 2023).
Other drug characteristics, such as its molecular weight, and drug conjugation, influence its excretion characteristics. For example, drugs with molecular weights greater than 300 Da, either polar and lipophilic groups, are more likely to be excreted in bile.
Many drugs are hydrophilic and are excreted unchanged by the kidney. Some examples include metformin (anti-diabetic med), gabapentin, many antibiotics (ampicillin, amoxicillin), lithium and the ACE inhibitor lisinopril. For clients with impaired renal function, dose adjustments may be necessary as the drug will take a longer time to be excreted.
Routes of Excretion
Kidney
The most common route of excretion is the kidney. After the drug is metabolized by the liver into a more polar metabolite, the kidneys then filters the blood and the majority of drug byproducts and waste are excreted in the urine. Medications may be filtered at the glomerulus, active tubular reabsorption, or active tubular secretion, where a portion may go back into the bloodstream with the rest excreted in urine.
Free drugs, water-soluble drugs, and electrolytes are easily filtered by the glomerulus and then readily excreted. Lipid-soluble drugs cross the renal tubular membrane and are reabsorbed back into circulation, as they need to be more hydrophilic for excretion. Most drugs are polar compounds by the time they reach the kidney and are excreted. Some drugs are excreted by more than one process in the kidney. For example, for the antibiotic Penicillin G, only 10% is filtered by the glomerulus and 90% is secreted by the renal tubules (Adams et al., 2018).
Glomerular Filtration and Drug Excretion
The kidney filters approx. 180 L of fluid per day.
Glomerular barriers restrict passage of plasma proteins and red blood cells. Drugs that are bound to albumin will not be effectively filtered.
Renal blood flow influences the rate of delivery of a drug to the kidney.
GFR (glomerular filtration rate) is affected by age or disease. GFR declines with age, generally by 1% per year. Diabetes accelerates the decrease in GFR.
Factors Affecting Kidney Function
The rate of excretion can be estimated by taking into consideration several factors: age, weight, biological sex, and kidney function. With aging, the renal drug excretion decreases. By the age of 80, renal function is typically half of what it was at age 30 (Le, 2024).
Excretion can also be impacted by disorders such as acute or chronic kidney disease. Kidney function is measured by lab values such as serum creatinine, glomerular filtration rate (GFR), and creatinine clearance (CrCl). If a client’s kidney function decreases, it affects their ability to excrete medication, and drug dosages must be reduced to avoid toxicity.
Other health disorders can impact drug clearance such as hypoperfusion from sepsis, disorders that affect antidiuretic hormone release or heart failure.
Drug Half-life: Recall that a drugs elimination half-life (T1/2) is the time required for the plasma concentration to decrease by 50%. What do this mean for drug dosages?
example: Metformin t1/2 is 17 hours. The client has CrCl of 50 mL/min. No dose adjustment is needed for mild-moderate renal impairment. If the CrCl is less than 30 mL/min, then the risk of lactic acid increases and then metformin will likely be discontinued.
example: Morphine t1/2 is 2-4 hours. This means that in 4 hours, 50% of the drug is eliminated from the body. If there is renal insufficiency, morphine’s active metabolites will not be excreted as readily, and its effects (pain control) and adverse effects (i.e. sedation) will linger (longer duration of action). But, if there is renal dysfunction, morphine’s active metabolites accumulate especially if there is moderate to severe renal failure. Dose reduction is 75% for mild renal insufficiency, and 50% for moderate disease.
For nursing practice, clients should be more closely monitored for therapeutic and adverse effects. Nurses should know common adverse effects of the meds they are giving. When considering drug dosage adjustments, it is worth noting that in practice, doses rarely need to be altered before the GFR drops below 50 ml/min (Tom et al, 2018).
Liver and Intestinal Tract
The process of metabolism begins in the excretion phase of drug metabolites. Whether the drug is polar or non-polar will determine the degree of transformation needed for the metabolite to be more readily excreted. Hepatic metabolism increases a drug’s polarity and water solubility leading to easier excretion.
Excretion in the bile is another significant form of drug elimination. As the liver filters blood, some drugs and their metabolites are actively transported by the hepatocytes (liver cells) into bile. Bile moves through the bile ducts to the gallbladder and then on to the small intestine. During this process of biliary excretion, some drugs may be partially absorbed by the intestine back into the bloodstream. Other drugs are biotransformed (metabolized) by intestinal bacteria and reabsorbed. Unabsorbed drugs and byproducts/metabolites are excreted via the feces. This enterohepatic recirculation of drugs can prolong the action of the drug and is considered when determining drug dosages.
Enterohepatic Recirculation
Enterohepatic recirculation is the cycle of drug, solutes, or bile acids as they are eliminated from the liver into the bile, then reabsorbed by the intestines, then returned to the liver.
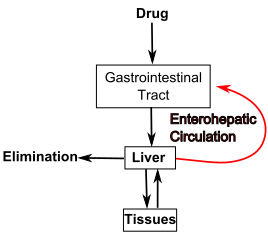
Figure 1.6a Hepatic Recirculation
If a patient is experiencing decreased liver function, their ability to excrete a medication is affected and drug dosages must be decreased. Lab studies used to estimate liver function are called liver function tests and include measurement of the ALT and AST enzymes that the body releases in response to damage or disease.
Renal Function Lab Values
Nurses need to know their client’s renal function to ensure safe med administration.
Se Creatinine (waste product of muscle metabolism):
- Men: 0.74-1.35 mg/dL
- Women: 0.59-1.04 mg/dL
Estimated glomerular filtration rate (eGFR) (how well kidneys filter waste from the blood):
- Normal: greater than or equal to 90 mL/min/1.73 m²
- Mildly decreased: 60–89 mL/min/1.73 m²
- CKD: less than 60 mL/min/1.73 m²
Other renal function labs include urine albumin, blood urea nitrogen (BUN), and creatine clearance.
Other Routes to Consider
Some medications are excreted through other routes such as the lungs, breast milk, and even minimally through tears, reproductive fluids (seminal fluids), and the skin. Drugs excreted by the lungs are anesthetic gases that are eliminated through exhalation. Following surgery, drug excretion via exhalation is dependent on the client’s respiratory function, such as respiratory rate and pulmonary blood flow (Adams et al., 2018).
Drugs excreted by saliva is primarily transferred through passive diffusion from the plasma and is dependent on such factors as a drug’s low protein-binding ability, ionization, polar surface area, and lipophilicity. Factors such as the saliva’s pH also play a role. There are over 40 medications that can be detected in saliva including the benzodiazepine Midazolam, opioids, cannabis, and some antibiotics.
Saliva Sample for Drug Monitoring
Although the amount of the actual drug excreted through saliva is negligible, where it is valuable is with therapeutic drug monitoring and testing. Typically, therapeutic drug monitoring for high-risk medications is done through blood tests, but new research shows that testing the saliva is less invasive and just as accurate as serum testing (Nyugen et al., 2024).
Drug Excretion in Breast Milk
Drugs excreted in breast milk require special consideration even if drug levels are minimal. Breastfeeding mothers may inadvertently transfer a drug by-product to their breastfeeding infant, which can prove dangerous to the infant. Numerous medications are contraindicated for breastfeeding mothers, such as the mood stabilizer lithium which can cause lethargy and hypotonia in the infant. Many psychoactive medications such as antidepressants (Fluoxetine) can cause irritability and feeding problems. Many other medications are detectable in breast milk but pose a theoretical risk (detectable in breast milk but no studies have been done to determine if they harm infants) and, as such, should be avoided. Similar to medication use throughout a pregnancy, medication use while breastfeeding needs to be discussed with their healthcare provider to weigh any risks versus benefits. It is important for the nurse to obtain a good health history and medication profile and to provide good health teaching to ensure infant safety.

Figure 1.6b Breastfeeding mother
Lifespan Considerations
Neonates & Pediatrics: Young patients have immature kidneys with decreased glomerular filtration, resorption, and tubular secretion. As a result, they do not clear medications as efficiently from the body. Dosing for most medications used to treat infants and pediatric patients is commonly based on weight in kilograms, and a smaller dose is usually prescribed. In addition, pediatric patients may have higher levels of free circulating medication than anticipated, which may quickly become toxic. Therefore, frequent assessment of infants and children is vital for early identification of drug toxicity (Fernandez et al., 2011).
Older Adults: Kidney and liver function often decreases with age, which can lead to decreased excretion of medications. Subsequently, medication may have a prolonged half-life with a greater potential for toxicity due to elevated circulating drug levels. Smaller doses of medications are often recommended for older patients due to these factors, commonly referred to as “Start low and go slow” (Fernandez et al., 2011).
See the final unit in this chapter, Lifespan Considerations for Pharmacological Principles for more discussion on lifespan variables.
Critical Thinking Out Loud
A nurse is reviewing a 65-year-old client’s lab work and sees that the eGFR for this client is 50 (normal eGFR is greater than 60mL/min). They have type 2 diabetes mellitus and have been admitted for a wound debridement. The nurse notices that many of the clients’ medications are prescribed at the same dosage as pre-admission. Is this a concern? Should clients with renal insufficiency have lower dosages of all their meds?
The answer to this question is not straightforward. Many factors impact drug clearance. For example, some drugs are only 30% renally cleared, so a decreased renal function is not a concern. Some drugs are considered a low-toxicity drug and only prescribed for a short period of time so the risk of accumulation is minimal. For example, if oral penicillin is prescribed for only a few days. Some drugs are taken for long term and have a high intrinsic toxicity, for example metformin or lithium. In these meds, a dose adjustment may be required to prevent high drug accumulation and to avoid toxicity. For example, the t1/2 of some meds will double after a 50% decrease in clearance due to impaired kidney function. This could lead to drug accumulation and risk of toxicity especially for chronic drug therapy (Tom et al, 2018; Hallare & Gerriets, 2025).
There is no absolute parameter of kidney function that necessitates a dose reduction for all meds as it depends on many variables. When considering drug dosage adjustments, it is worth noting that in practice, doses rarely need to be altered before the GFR drops below 50 ml/min. In this clients case, the nurse reviewed the adverse effects of the meds the client was taking, and made note to monitor the lab work each day. The nurse also spoke with the prescriber about any med they were concerned about and if a dose reduction or closer renal monitoring was needed.
Note: Answers to the Clinical Reasoning and Critical Thinking activities can be found in the “Answer Key” sections at the end of the book.
Putting It All Together
Prescribing and administering medications in a safe manner to clients is challenging. The ultimate goal of any medication use is to have a positive therapeutic outcome with minimal adverse effects. How a drug moves throughout the body is important to understand to ensure correct drug dosing, monitor for drug response, and evaluate the overall effect. Aging clients or other lifespan considerations, acute or chronic health conditions, drug-drug interactions, and other variables can all impact the pharmacokinetics of the drug. Safe and efficient pharmacotherapy requires collaboration with and within the healthcare team, including prescribers, pharmacists, nurses, and other allied health care members.
The next section, pharmacodynamics, will examine what the drug does to the body.
Watch Pharmacokinetics: How drugs move through the body [7:54] by Professor Dave Explains (2020).
References
Adams, M., Urban, C., El-Hussein, M., Osuji, J., & King, S. (2018). Pharmacology for nurses. A pathophysiological approach (2nd Canadian ed.). Pearson.
Burcham, J. R., & Rosenthal, L. (2019). Lehne’s pharmacology for nursing care (10th ed.). Elsevier.
Fernandez, E., Perez, R., Hernandez, A., Tejada, P., Arteta, M., & Ramos, J. T. (2011). Factors and mechanisms for pharmacokinetic differences between pediatric population and adults. Pharmaceutics, 3(1), 53–72. https://doi.org/10.3390/pharmaceutics3010053
Garza, A. Z., Park, S. B., & Kocz, R. (2023). Drug elimination. StatPearls. Retrieved October 20, 2025, from https://www.ncbi.nlm.nih.gov/books/NBK547662/
Grogan, S., & Preuss, C. (2023). Pharmacokinetics. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK557744/
Johnson, S. (2007). Opioid safety with patients with renal or hepatic dysfunction. Pain Treatment Topics. www.Pain-topic.org Opioid Safety in Patients With Renal or Hepatic Dysfunction
Le, J. (2024). Drug excretion. Merck Manual. https://www.merckmanuals.com/professional/clinical-pharmacology/pharmacokinetics/drug-excretion
Nyugen, T. A., Chen, R. H., Hawkins, B. A., Hibbs, D. E., Kim, H. Y., Wheate, N. J., Groundwater, P. W., Stocker, S. L., Alffenaar, J-W. C. (2024). Can we predict drug excretion into saliva? A systematic review and analysis of physicochemical properties. Clinical Pharmacokinetics, 63, 1067–1087. https://doi.org/10.1007/s40262-024-01398-9
Professor Dave Explains. (2020, March 24). Pharmacokinetics: How drugs move through the body [Video]. YouTube. https://www.youtube.com/watch?v=L1W0q1kEof4
Rosow, C., Standaert, D., Strichartz, G. (N.d.). Principles of Pharmacology. LibreTexts. CC BY-NC-SA 4.0
Sealock, K., & Seneviratne, C. (2021). Lilley’s pharmacology for Canadian health care practice (4th ed.). Elsevier.
Tom, L., Carland, J., Stocker, S., Sevastos, J., Roberts, D. (2018). Clinical Pharmacokinetics in Kidney Disease: Fundamental Principles. Clinical Journal of the American Society of Nephrology 13(7):p 1085-1095. DOI: 10.2215/CJN.00340118
Media Attributions
Figure 1.6a Hepatic Recirculation. Enterohepatic.svg https://commons.wikimedia.org/wiki/File:Enterohepatic.svg
Figure 1.6b Breastfeeding mother. https://www.needpix.com/photo/794304/breast-feeding-motherhood-mother-breast-milk-child-the-birth-of-love-a-small-child

{kind=link}